Transcription
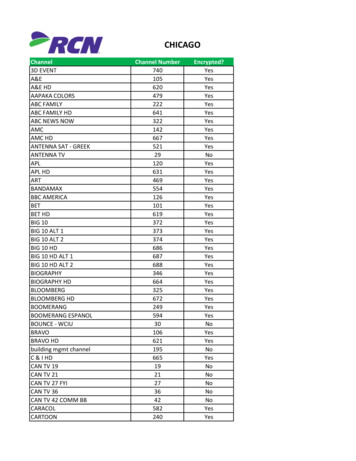
PANDIT NEW PATIENTToday's Date*Crovetti Orthopaedics & Sports MedicineGender:PLEASE COMPLETE THIS FORM ENTIRELYPatient Name- - - - - -- - - - - - - ------SS#------------DOB//MAgeFAddressApt#City State Zip Marital StatusPreferred Phone - Home or Cell?Secondary Phone - Home or Cell?*would you like to receive appointment reminder calls from our automated calling system? Circle one:NOYES*If you agree to receive email communications from our office (which may include information about your medical care, any potential surgeries,appointments, billing, etc.), please provide your email address:EmployerWork Phone, ccupali n***Parent/Spouse-- - -- - ----Pharmacy Name -Pharmacy AddressDt:parlment---------------Phone Number--- - -DOB--------- --------------- *Phone Number -------------------------- Emergency Contact- - - - - - - - - - - -(Not living with you)- Relation to Patient------------- Phone ---------------------*Reason for Visit--------- - - - ------------------- Date symptoms startedIs this related to an injury? YES/ NOIf yes, please describe injuryIs it work related? YES I NOIs it auto related? YES/ NOHa ve you seen a doctor for your problem? YES / NO If yes, when?Were X-rays or scans taken? YE S/ NOIf yes, when & where?Referred by Dr.PhoneHow did you hear about our office? Circle one:Physician ReferralHospital ReferralFriend/FamilyMagazine AdWord of mouthOtherTV AdTheater AdInternetBillboard-------------*Primary Insurance Company ---------------- - - - - - ------ PhonePolicy ID Number Group Numb erPrimary Insured------------------- - - - - DOB --I-- /--- SS# ----Employer Effective dateRelation to Patient:Self Spouse Parent--------*secondary Insurance CompanyPhonePolicy ID NumberPrim ary Insured1:;mployer- - - - - - - - - - - - - - - -- - ---- DOBGroup NumberII-------Effective dateRelation to Patient:SelfSpouse ParentSS#-- - --- - - - - - -
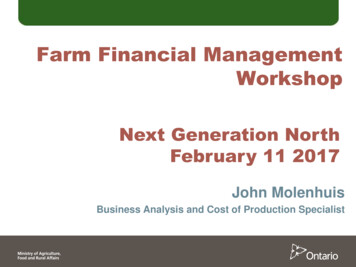
Have you had any of the following?How Many?D Steroid InjectionsLast J:njcctiOJ.1Last InjectionD Viscosupplementation Injections (Synvisc, Orthovisc, Euflexxa, etc)D Bracing - - - - --- Physical TherapyHow Many?How Long?D Anti-Inflammatory Medications (past & present- Aleve, Advil, Ibuprofen, etc)Pain at night?Daily pain level (1-10)Back Pain DYHave you ever experienced or been told by a doctor that you have any of the following conditions?AnemiaIrregular HeartbeatBlood ClotsAutoimmune disease (RA/Lupus etc)Congestive Heart FailureHeart Attack/Coronary DiseaseGastrointestinal BleedingGERD/.Reflux/Stomach UlcerHeart Valve DiseaseKidney or Liver DiseasePeripheral Vascular DiseasePlease elaborate briefly:Stroke/TIAAny other medical history that we should know about not previously listed?DENTAL HISTORYDenturesDental ImplantsGum DiseaseMost recent dental appointment, if no dentures (MM/YYYY)SKIN ISSUESDo you now have, or have you previously had any skin issues to include?Slow or poor wound healing?YesNoEasy bruising or bleeding?YesNoRecurrent rashes?YesNoSkin infection (cellulitis/abscess)YesNoIf yes please briefly explain:---------- - - --- - - - -------------
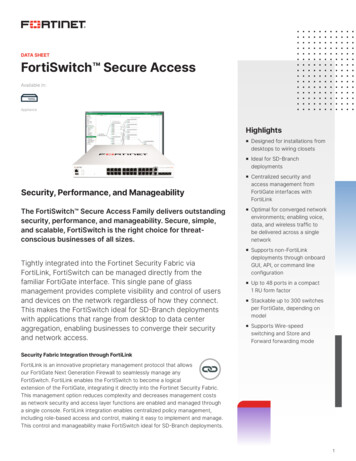
PANDIT NEW PATIENTMEDICAL HISTORYALL Q ESTIONS M rs·:r BE ANSWEREDREASON FOR MEDICATIONDOSEMEDTCATION (prescribed, OTC,and/or supplements)******SIDE EFFECTSCHECK IF A MEDICATION LIST IS ATTACHED.ALLERGIES:REVmW OF SYMPTOMS: Are you currently having or have you had problems with:EyesNOYESEars, Nose, ThroatNOYESLungs, BreathingNOYESDigestionNOYESBowel MovementsNOYESBladder ProblemsNOYESDiabetesNOYESHigh Blood PressureNOYESHeart DiseaseNOYESBleeding ngNOYESPsychological SPolioNOYESTBNOYESEpilepsyNOYES(Please describe all YES responses)PAST MEDICAL HISTORY:Surgcl'ies/1-los[!ilaliwtionsDate & Facility NameCom11lica !'ionsHave you ever had general anesthesia? YES / NOIf yes, did you have any problems with anesthesia? YES / NO If yes, describe
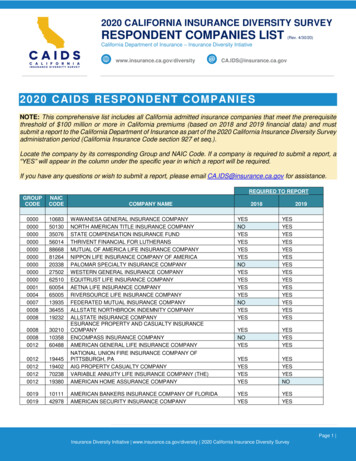
PANDTT NEW PATIENTSOCIAL HISTORYAre you a student? YINDo you work in the home? YINAre you employed? YINFull time/ Part timeDo you have children? Y / NIf yes, how many?Do you exercise? YINHow often?Do you I ive alone? Y / NAre you retired? YINOccupationDailyWeeklyMonthlyWhat type ofexercise?Do you have a history of substance abuse? Y / NDo you currently smoke? Y / NDo you drink alcohol? YINNeverRarelyWhat type?How many packs per day?Have you quit smoking? YIN If yes, when?How many years?Packs per day forThis year l year 5 years l O yearsHow often? Daily, # of daily drinksl-2/week l-2/monthyears1-2/yearNever*MEDICARE PATIENTS:Are you currently in a skilled nursing facility? YIN If yes, which one?---- - - - - -------------- - - - - - - Date of dischargeDate ofadmission------------Have you been in a skilled nursing facility in the past six months? YIN If yes, which one?Date ofdischargeDate of admission-------------HIPAA RELEASEI authorize the following person(s) to be able to obtain my protected health information from Crovetti Orthopaedics & Sports Medicine. By listing someone below (suchas a spouse, child, parent, trusted friend) you are giving our staff permission to communicate to another person about scheduling, treatment, care and billing as itpertains to you, the patient. Ifwe do not have the information below, we CANNOT speak to anyone other than the patient about any protected health information.If patient is a minor, we are allowed to speak to the parent that consented to treatment.Name:Relationsllip: Phone:Name:Relalion hip: Phone:Name:Phone::RelationshipI wish no one to have access to my protected health information.Consent for Treatment and PaymentI hereby request treatment by Crovetti Orthopaedics & Sports Medicine and consent to care and treatment as ordered by my physician(s). I authorizethe release of information related to my treatment to my referring physician(s). I authorize Crovetti Orthopaedics & Sports Medicine to submit thisclaim on my behalf for the medical services provided. I hereby authorize my health insurance company to make payment(s) directly to CrovettiOrthopaedics & Sports Medicine, for any benefits that I may receive. I understand that I am financially responsible for all charges made to myaccount whether or not an insurance company, attorney, or third party payer is involved with payment. I am responsible for all co-payment and co insurance amounts, non-covered supplies and services along with yearly deductibles. Payment for services is expected at the time services arerendered. I authorize the release of any information necessary to process my insurance claims and facilitate payment of my account by a third party.I understand that Crovetti Orthopaedics & Sports Medicine does not discriminate against any person on the basis ofrace, color, religion, gender or gender expression,sexual orientation, age, national origin, disability, or marital status.Print Patient NnrncSignature of Puticnl ----------------------------(*if patient is a minor - DO NOT SIGN - Parent/Guardian to sign next line)- *Signature of Responsible Pmty(*if patient is a minor) Relation lo patient ---Reviewed by Dr.---DateDute----------------------- - - - --------- - - - - - - - - - - - - -----Dale
I hereby request treatment by Crovetti Orthopaedics & Sports Medicine and consent to care and treatment as ordered by my physician(s). I authorize the release of information related to my treatment to my referring physician(s). I authorize Crovetti Orthopaedics & Sports Medicine to submit this claim on my behalf for the medical services provided.