Transcription
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching Hospitals-1-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching Hospitals(AL-QURAN)-2-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsStandard Operating ProceduresFor Health Professionals & Teaching HospitalsMuhammad UmarMBBS, MCPS, FCPS, FRCP (Glasg), FRCP (London), FACG, AGAFChairman & Professor of MedicineRawalpindi Medical College RawalpindiChief Gastroenterology & Hepatology DivisionHoly Family Hospital RawalpindiHamama-tul-Bushra KhaarBSc, MBBS, FCPS, FRCP (Glasg), FACGProfessor of MedicineRawalpindi Medical College RawalpindiConsultant Gastroenterologist & HepatologistHoly Family Hospital RawalpindiJawad ZaheerMBBS, FCPSAssistant Professor of AnesthesiaHoly Family HospitalRawalpindi-3-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsContributorsDr. Zahid Mahmood MinhasDr. Jahangir SarwarMD-DCPSSenior Registrar MedicineHoly Family HospitalMBBS, FCPSAssociate Professor of SurgeryHoly Family HospitalDr. Raja Adnan ArifMDHouse PhysicianHoly Family HospitalDr. Muhammad KhurramMBBS, FCPS, FRCPAssistant Professor of MedicineHoly Family HospitalDr. Abdul NaeemDr. Masood AhmadMBBSMedical OfficerHoly Family HospitalMBBS, FCPSAssistant Professor of MedicineHoly Family HospitalDr. Muhammad SaleemMBBSPost Graduate TraineeHoly Family HospitalDr. Athar TehseenMBBSAdditional Medical SuperintendentHoly Family HospitalDr. Marina KhanMBBSHouse PhysicianHoly Family HospitalDr. Saima AmbreenMBBS, FCPSSenior Registrar MedicineHoly Family HospitalMuhammad BilalFourth Year Medical StudentArmy Medical College, RawalpindiDr. Abrar AkbarMBBS, FCPSSenior Registrar MICUHoly Family HospitalJahanzeb KhanIT Administrator-4-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsForewordThese SOP’s are aimed to provide an objective format for working of professional staff,administrators, paramedics, nurses, junior doctors, patient care as well as working of differentdepartments and sections of hospital. This document will be first of its kind in the publicinstitutions of Punjab, which provides clear guidelines for working of different components ofhospital as well as health professionals. It will advocate the performance based working andevaluation of health institutions. SOP designing is a dynamic process which keeps on changing.This booklet is first step toward this process which will be refined by future authors.The SOP’s for Surgical ICU patient care and equipment maintenance are exclusivelywritten by Dr. Jawad Zaheer, Assistant Professor Anesthesia Department, Holy Family Hospital.This section which provide base line parameters for an important section of this hospital.I really appreciate Prof. Mussadiq Khan Chief of Rawalpindi Medical College andAllied Hospitals, who stressed the need to formulate these SOP’s. I also want to extend mygratitude to Dr. Athar Tehseen Additional Medical Superintendent Holy Family Hospital, whodid tremendous efforts to develop these SOP’s. I am also thankful to Medical SuperintendentHoly family Hospital, Dr. Abid Hussain Shah for finalizing these SOP’s. I think it will be unfairnot to mention the efforts of Dr. Shahzad Ahmad staff officer of principal, Rawalpindi MedicalCollege to coordinate all activities in developing these SOP’s.Finally I am grateful to my team including Prof. Hamama-tul-Bushra Khaar, Dr.Masood Ahmad, Dr. Saima Ambreen, Dr. Zahid Mahmood Minhas, Dr. Adnan Arif, Dr. AbdulNaeem, Dr. Marina Khan and Jahanzeb Khan for their cooperation to formulate these SOP’s.Prof. Muhammad UmarDecember – 2009-4-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsAbout the AuthorsMuhammad UmarMBBS, MCPS, FCPS, FRCP (L), FRCP (Glasg), FACG, AGAFGraduated in 1981 from Rawalpindi Medical College with distinction and Presidential Gold Medal by Presidentof Pakistan. Started his professional career as Assistant Professor of Medicine after obtaining membership(MCPS) and then fellowship (FCPS) from College of Physicians & Surgeons Pakistan in 1985. He was awardedfellowship from American College of Gastroenterology (FACG) in 2002, Royal College of Physicians London(FRCP), Royal College of Physicians Glasgow (FRCP) in 2006, and American Gastroenterological Association(AGAF) in 2007. First Governor of American College of Gastroenterology (ACG) for Pakistan. He was appointedAssistant Professor, Associate Professor and currently the Professor & Chair of Medicine and Chief ofGastroenterology & Hepatology Division in RMC. He had keen zest for gastroenterology and specificallyhepatology, so he started pursuing his career in this field. He established GI & Liver Clinic, GI & Liver LearningResource Centre, and Liver Research data base at Holy Family Hospital Rawalpindi in 1998.He had contributed to gastroenterology by publishing more than 70 review and original research papers invarious national and international journals, two books on hepatology; Evidenced Based Approach to Hepatitis CManagement and Hepatitis C in Pakistan. Moreover, he published National Hepatitis Practice Guidelines. Hewas awarded SJZ Research Award by Pakistan Society of Gastroenterology & GI Endoscopy in 2004. He was thePast President of Pakistan Society of Gastroenterology & GI Endoscopy, President Elect Pakistan Society ofHepatology, and President of Rawalians' Research Forum on GI & Liver Diseases. Medical Director of HolyFamily Hospital Rawalpindi (2009), Member of Board of Management of Rawalipindi Medical College and AlliedHospitals He is on Editorial Board of Journal of Rawalipindi Medical College, Associate Editor of Journal ofPakistan Society of Gastroenterology. Editorial Board of Bangladesh Journal of Hepatology, Editorial Board ofLibyan Journal of Gastroenterology, and Member of International Cor-Curriculam Committee on GI Endoscopyof OMED, Member Global Guideline Committee of World Gastroenterology Organization (WGO), ClinicalCoordinator of National Prevention and Control Program of Hepatitis. He is Chairman ASIAHEP Pakistan. He isauthor of “Standards in Gastrointestinal Endoscopy Training” “MD Training Program for Gastroenterology” and“Basic Skills in Gastrointestinal Endoscopy Training Manual” and Medical Emergencies ManagementGuidelines. He is a member of foreign graduate evaluation committee of PMDC.Hamama-tul-Bushra KhaarBSc, MBBS, FCPS, FRCP (Glasg), FACGShe graduated from Rawalpindi Medical College Pakistan being Best Graduate in 1981. She obtained fellowshipfrom College of Physicians & Surgeons Pakistan (FCPS) in 1985 and started her career in medicine. She washonored with fellowships from Royal College of Physicians Glasgow (FRCP) and American College ofGastroenterology (FACG) in 2007. She was appointed Assistant Professor, Associate Professor and currently theProfessor of Medicine at Rawalpindi Medical College and consultant gastroenterologist at Holy Family HospitalRawalpindi Pakistan. She had strong interest in gastroenterology and hepatology, so she started pursuing hercareer in it. She started practicing gastroenterology and developed and Endoscopy Suit at District HeadquartersHospital Rawalpindi in 1995.She has a long list of publications including original and review papers, books, guidelines, and manuals. She haspublished about 80 research papers, two books on hepatology; Evidenced Based Approach to Hepatitis CManagement and Hepatitis C in Pakistan. Moreover, she published National Hepatitis Practice Guidelines and“Basic Skills in Gastrointestinal Endoscopy Training Manual”, MD Training Program, Standards inGastrointestinal Endoscopy,. She is Editorial Board of Pakistan Journal of Gastroenterology and ResearchDirector of Rawalians Research Forum since 1998.-5-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSection – IContentsSOP’s for Patient Care8¾Emergency Department9¾Reception and Treatment of Patient in ER13¾Process Flow for Medical Patients in E.R.15¾Process Flow for Surgical Patients in E.R.16¾Intensive Care Unit17¾In-Door Patient Care19¾Out Patient Department23¾Procedure Room27¾Endoscopy Room / Echocardiography28¾Pathology Reception29¾Radiology Department31¾Ultrasound and Doppler Examination32¾Cleaning and Washing33Section – IISOP’s for Health Professionals35¾Job Description of Emergency Staff and Doctors36¾Disaster Management Plan39¾Consultants40¾Professor40¾Associate Professor/Assistant Professor/Senior Registrar40¾Registrars / MOs41¾House Officers41¾Charge Nurses43¾Staff Nurses45¾Ward Servant46¾Ward Cleaners47Section – III - SOP’s for Administrative Departments48¾Admin Office49¾Purchases50¾Procurement of Stores (Medical/General)53¾Issuance of Stores (Medical/General)54¾Repair of Electro Medical Equipment55¾Works ( Development/ M&R) Department56-6-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSection – IVSOP’s for Prevention and Control of Infection58¾Occupational Health Risk59¾Barrier Precautions for Students59¾Healthy Behaviors Adaptation for Prevention and60Control of Hepatitis A, B, C, D and E¾SOP’s for Injection Safety, Device Control and Hospital Waste Management62¾Waste Disposal Policy63Section – VSOP’s for Surgical ICU Patient Care and Equipments Maintenance67¾Surgical Intensive Care Unit68¾DVT and Thrombo-embolism Prophylaxis68¾Thoracic Epidural Catheter Care69¾Nutritional Support of Patients in ICU70¾Criteria for Extubation in ICU71¾Ventilator Checklist72¾Protocol for Starting Ventilatory Support73¾Cleaning and Asepsis of Ventilators75¾Change of Condenser Humidifier of Ventilator76¾Chest Physiotherapy77¾Correction of Base Deficit77¾Care of Central Venous Lines78¾Contents of Emergency Trolley79¾Emergency drug tray80¾Preparation of drug infusions81¾Infection control procedures in ICU82¾Replacement of Potassium84¾Change of Patient’s Position in Bed85¾Visitor Policy in ICU86¾Clinical Audit87-7-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSECTION – ISOP’S FOR PATIENT CARE-8-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSOP’S FOR EMERGENCY DEPARTMENTAll shifts should follow strict timings.Notes and Evaluation¾House officers and residents are primarily responsible for managing patients inEmergency during their call day.¾Referred patients should be seen within 10 minutes of referral by CMO. Immediatelyreceive patient, check vitals before digging through old record, lab results, old dischargesummary and old charts.¾SOAP format should be used for patient notes. Proper documentation of symptoms,management and diagnosis will be done for every patient. Serious patients should beimmediately seen and resuscitated. Procedure of referral & consultation will proceed sideby side. Monitoring notes should be properly maintained including fluids given andoutput of patient.Admissions¾Duty registrar should decide all admission through ER.¾After assessment and patient’s examinations complete admission orders including drugprescription should be written clearly and immediately.¾For stat labs inform nursing staff immediately or carry out by your self.¾Notes on history and examination file should be completed before shifting to In-Patient.¾Complete shifting notes before shifting to the ward.¾Para-medic staff should accompany every admitted patient during shifting to the ward Incase of serious patient, house officer should accompany.¾Before shifting, inform the ward staff on call.¾If beds are not available in wards, retain patients in ER till arrangement are made; Ifrequired discuss with consultant on call or DMS ER.Procedure Notes¾Write notes for every procedure, which should include Name, Site, Indication, Consent,Sterile prep and anesthesia of procedure. Description of specimen of Fluid and what andwhere they are sent for with brief clinical notes.¾Inform patient regarding indications, complications and post-procedure precautions.¾Get signatures on informed consent.¾Never forget pending follow up studies like Post-Procedure X-ray.Discharges¾No patient should be discharged without being evaluated by the duty registrar.¾Keep in mind pending issued and studies.¾Communicate with all involved parties for smooth discharge.¾Give clear instructions regarding medicines schedule/side effects/precautions andrestrictions on activities/travel/diet in Urdu/local language Make sure by repetition thatpatient can repeat/recall your instructions.¾Write discharge diagnosis clearly.¾Notes should include Chief complaints and H/O Present illness, hospital stay course,Your Name, Hospital No/principal and secondary diagnosis and Procedures.¾Mention Follow-up plan/condition on discharge/attach Diet chart if required.-9-
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSignouts¾¾¾For on-call batch, out going House officer will give written information about theirpatient’s Active issues and it should include Name of patient, ward/bed no. diagnosis,active issue or pending critical labs., consultations and procedures. Also, include certaincriteria to act on e.g. Transfuse one unit packed cell if Hct is less than 28.CODE Status must be specified.Highlight worrisome patients, issue of concern and suggestions to deal with them.Death / Expirations¾On being called to pronounce death you must perform certain steps.¾On arrival to bed site observe for respirations, auscultate for heart sound palpate forcarotid pulse, check pupil and corneal reflex.¾Complete death notes on progress sheet and fill death certificate as early as possible.Urgent Thrombolysis¾In patients with indications for Thrombolysis, every possible effort should be made toachieve urgent Thrombolysis to decrease “door-to-needle-time” in order to save preciousmyocardium.Occupational Risks¾¾Standard barrier nursing and isolation techniques should be employed in cases of patientswith infectious communicable diseases.These measures include: Gloves Masks Careful needle/sharp object handling Prophylaxis in cases of exposure if indicated (e.g. meningococcemia).In case of mishap/exposure, event should be reported to consultant on call, immediately.Accountability¾In case of an incident, a committee of ward consultant will review the entire case in detailand will decide about warning/penalty.Ethical Issues¾Best interest of the patient should be watched, in case of conflict or confusion, issuesshould be discussed with consultant on call.Confidentiality of Patient’s Data¾Patient’s record and data should be kept confidential to watch his/her interests anddiagnosis/prognosis should not be discussed with attendants without permission ofpatient/close attendant.- 10 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSenior Consultation¾On call consultant/senior registrar should be contacted on phone if required by theregistrar on call. If he/she may request to see the patient then on call consultant shouldtry to attend the patient personally within I hour of the request.Consultations from Other Departments / Urgent Scans¾Consultants and scans should be decided by the duty registrar and call to the respectivedepartment should be written with clear indications exact questions to be observed andurgency of the consultation.Patient Transfer to Other Facilities¾¾¾¾¾Once decision is made to transfer the patient to the other hospital for management,contact the concerned doctor/staff there first on telephone and discuss the case in detailand request them to make sure the bed is available for the patient.Note down the contact person’s name and designation.Provide detailed notes on the referral slip.Provide ambulance preferably by the hospital through coordination with DMS/CMO, andif patient is serious, a doctor should accompany while transportation.Ambulance should be equipped with resuscitation equipment.Record Keeping¾¾¾¾ER register shall be filled properly with composite diagnosis or relevant differential forevery patient.Duty registrar will sign register at the end of duty, and counter-signed by coveringconsultant for that day before morning meeting.Record of consultations provided to other department should be kept in the registrar.Death notes for patients who expired in ER should be written in the ER registerimmediately after the event.Drugs & Investigations¾List of drugs and lab profile available in hospital for ER patients should be available toeach shift of ER staff.Duty Timings¾House officer¾Registrarunderstanding) 8 am to 8 pm- second shift 8pm to 8am (nm) 8am to 8 am (nm) (batch on call should adjust the timing with mutualBLS/ACLS Training¾House officers and registrar should be trained in BLS/ACLS before performing duties inE.R.- 11 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsDress Code¾¾Dress should be conservative & modest. No informal clothing (jeans & T-shirts for males),party wears or excessive jewelry (for females) is allowed, during duty hours.Every doctor should wear neat & clean overall, with properly displayed ID card or nameplate.- 12 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSOP’S FOR RECEPTION AND TREATMENT OF PATIENTS IN ER1.Patient comes to the ER Department.2.If patient is critically ill. He/she is shifted on trolley or wheelchair, by the Ward Boydeputed for this purpose, to reception.3.At the reception, the patient will be registered and ER slip will be issued along with aclinical notes sheet/ER admission slip. The reception clerk will make entries of thepatients in the computer as well as the register and send the patient to the CausalityMedical Officer (CMO).4.The CMO will examine the patient and if the patient is suffering from minor ailment thenCMO will advise treatment on clinical note sheet as well as ER admission slip and sendthe patient to Charge Nurse for injection (it needed), after which patient is sent home andthe clinical note sheet will be taken by the Charge Nurse.5.If the patient is critically ill the patient will be referred to the concerned Medical/Surgicalunit by the CMO.6.The referred patient will be attended by the MO/PGT of the concerned specialty(Medical/Surgical). The House Officer of the concerned unit will follow the instructionsThe MO/PGT/SR of the concerned unit will write down the treatment plan on the clinicalnote sheet and sign it.7.No treatment plan will be written on the E.R. slip which is to be kept with the patient forfinal disposal.8.The investigations will be ordered by the MO/PGT/SR and House Officer is responsibleto send these investigations to the E.R. Lab/Radiology department.9.If the patient is admitted in the ward, both E.R. slip and clinical note sheet will be attachedwith the admission documents.10. Incase of serious patients the treatment plan should be discussed with the consultant oncall.11. If the patient is discharged/expired after treatment the clinical note sheet will be kept asrecord in the E.R. and Head Nurse/Charge Nurse of E.R. is responsible to keep thisrecord.12. In case of expiry of the patient MO/PGT will prepare the death certificate and sign it. Hewill also write down the death summary in the death register of ER.- 13 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching Hospitals13. The treatment of discharged patients should be written on the E.R. slip and handed overto the patient for follow up. It should be duly signed by the SR/PGT of the concernedunit.14. No House Officer is allowed to discharge the patient without the knowledge of SR/PGT15. Dispenser on duty in E.R. is responsible for the entry of these patients in the MasterRegister.- 14 -
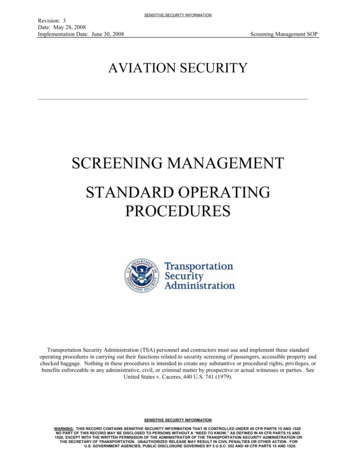
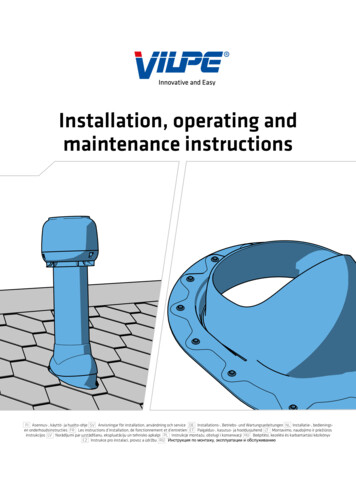
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsPROCESS FLOW FOR MEDICAL PATIENTS IN E.R.- 15 -
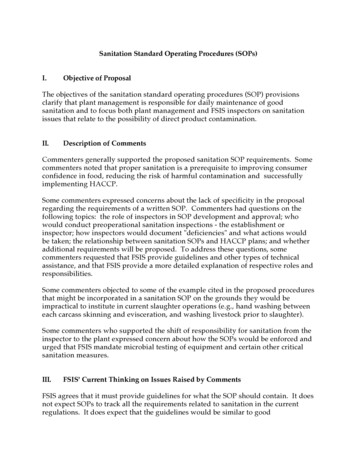
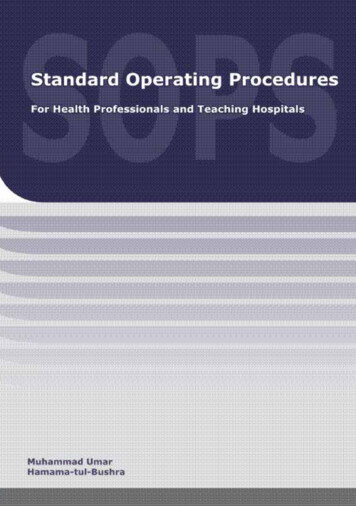
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsPROCESS FLOW FOR SURGICAL PATIENTS IN E.R.- 16 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSOP’S FOR INTENSIVE CARE UNIT1.2.3.4.5.6.7.8.9.10.11.12.13.14.15.All shifts should follow strict timings:a. Morning07:30 14:00b. Evening13:30 20:00c. Night19:30 08:00All fixed ITC staff, if possible, should wear OT dress and doctors will wear gowns.Strict aseptic measures should be taken in ITC i.e. Masks, Gloves, Caps, Shoes etc.No attendant, who so ever he/she is, NOT ALLOWED TO ENTER ITC except duringfollowing hours:a. Morning07:00 07:30b. Evening13:00 14:00c. Night17:30 20:30No staff member except doctor will ask attendants is buy medicines from medical store. Theconcerned doctor will duly sign the prescription slip.a. All lab/radiological tests will be requested on presented request forms signedby MO/PGT of ICU.The decision about the shifting of the patients to ITC must be made by registrars with fullclinical notes and indications and House Officer of the concerned department should bethere to receive the patient. No VIPs/protocols or non bed availabilities in other wardsshould be considered.Patients admitted/shifted in ITC by any Department, the House Officers of concernedDepartment must stay round the clock with their patients, abiding by all the rules andregulations of ITC. No chit system will be entertained; the house officer of concerneddepartment on call will be present at all times.House Officers/Medical Officers/Registrars rosters of all departments should be displayedon ITC notice board.All non-concerned doctors/staff will enter inside ITC after changing shoes.Staff/Doctors on duty in ITC will not leave their place of duty in any case.A complaint box will be placed in ITC for complaints of patients/attendants of ITC.Any complaints/problems/suggestion by any doctors/staffs or any hospital employeeconcerning ITC should be submitted with In Charge ITC.No visitor of any duty staff/doctors of ITC should be entertained during duty hours.There will be three shifts in-charge nurses and they will have their own medicinecupboards and maintain their record.Morning In-charge staff will also keep stock of linen (All shifts).RESIDENTS / HOUSE OFFICERSResidents/House officers will perform shift duties (8 hourly)All shifts should follow strict timings.House officers and residents are primarily responsible for writing daily notes on each of theirpatients.S.O.A.P. format should be used for daily notes.Drug dosage, side effects and interactions should be checked daily and major points should benoted down in patients file.- 17 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsDaily ReviewsDo IV Lines need to be changed?Can IV Meds be changed 100 Oral?Can you discontinue Foley, NG and IV Cannula?Can you advance diet and increase patient’s activities?Is patient moving his/her Bowels?Are all meds are adjusted for Renal and Hepatic Function?Every lab test or study needs to be followed upWhen in doubt ask and ask again.Equipment, Resuscitation Drugs and Crash Cart Check.With the help of duty staff nurse, house officer will daily check for working of equipment, drugavailability.Resident will counter sign daily check list for drugs and equipments.Any discrepancy should be reported to concerned DMS/AMS in writing and record should bekept for every application.FOR DISINFECTION FOLOW DISINFECTION PROTOCOL.FOR ALL ADMISSIONS & DEATHS FOLLOW SOP FOR WARD PATIENT CARE.- 18 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsSOP’S FOR INDOOR PATIENTSInpatient: (Male/Female/Officers/ICU Wards)All shifts should follow strict timingsDaily Notes and Evaluation¾House officers and residents are primarily responsible for writing daily notes on each oftheir patients.SOAP Format should be used for daily notes¾¾¾¾¾¾¾¾Subjective: What patient says and what nursing staff reports in past 24 hoursObjective Factual Information/Vitals/Physical Exam/Lab Results/Lines and tubesinclude X-rays and other studies, intake and output, side effects of drugsAssessment and Plan: Usually categorized by problem or organ system in order ofimportance. Always include Fluids/Electrolytes/Nutrition as well as code status inevery note. Also include Discharge planning/status and Goals etc.Active Medicines are often listed in side column. Review medications daily. Include dayno for Antibiotics and other loading dose medications.Every lab result/investigation report should be analyzed carefully and countersignedby House officer/Resident Abnormal investigations is be highlighted.Formulate Active Problem list.Draw algorithm of patient's symptoms, where applicable.House officers, should write in blue and registrars in red ink.Drug Reviews¾Drug dosage, side effects and interactions should be checked daily and major pointsshould be noted down in patients file.Daily Reviews¾ Do IV lines need to be changed?¾ Can IV medicines be changed to Oral?¾ Can you discontinue Foley, NG and IV Cannula?¾ Can you advance diet and increase patient’s activities?¾ Is patient moving his/her Bowels?¾ Are all medicines adjusted for Renal and Hepatic Function?¾ Every lab test or study needs to be followed up.¾ When in doubt ask and ask again.Admissions¾¾For new admissions immediately receive patient, check vitals before digging throughold records, lab results, old discharge summary and old charts.After assessment and patient's physical exam, complete admission orders includingdrug prescription immediately.- 19 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching Hospitals¾¾¾¾For stat orders inform nursing staff immediately or carry out by yourself.House officer on call should complete notes on History & physical Examination for alladmissionsHouse officer incharge for bed will write his/her initial summary within 24 hours ofadmissions and will complete notes in detail.In case of transfer of patient from one bed/ward to other concerned HO/registrar willwrite his/her own summary.Procedure Notes¾¾¾¾¾Procedures should be done with a proper written consent.Should include name, site, indications, consent, sterile prep and anesthesia ofprocedure, description of specimen, or fluid, what and where they are sent for, withbrief clinical notes.Inform patient regarding indication, complication and past procedure precautions.Never forget pending follow up studies like post procedure X-ray.If certified in a certain procedure only then trainee will be allowed to performindependently other wise procedure should be done under supervision of asenior/certified person.Discharges¾ Keep in mind pending issues and studies.¾ Communicate with all involved parties for smooth discharge.¾ Start discharge planning on admission.¾ Make sure patient and family are aware of possible discharge dates so they can arrange/ schedule transportation.¾ Preferably change IV antibiotics to oral one day before discharge, avoid orders onmorning of discharge unless absolutely necessary.¾ Give clear instructions regarding meds schedule/side effects/precautions andRestrictions on activities/travel/diet in Urdu/local language. Make sure by repetitionthat patient can repeat/recall your instructions.¾ Write discharge diagnosis clearly.¾ D/C summary should include chief complaints and H/O present illness, hospitalcourse, your name/ward name/Hospital name/DOA &DOD/Principal and secondarydiagnosis and procedures.¾ Mention follow-up/condition on discharge/attach diet chart if required.Sign Outs¾¾¾For on-call batch, out going House officer will give written information about theirpatient’s active issues and it should include Name of patient, ward/bed no., diagnosis,active issue or pending critical labs., consultations and procedures. Also, include certaincriteria to act on e.g. Transfuse one unit packed cell if Hct is less than 28.CODE Status must be specified.Highlight worrisome patient’s issue of concern and suggestions to deal with them.- 20 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsDeath/ Expirations¾¾DNAR (Do not attempt resuscitation) status should be decided after discussion withconsultant on call.On being called to pronounce death, you must perform certain steps.o On arrival to bed side observe for respirations, auscultate for heart soundpalpate for pulse, check pupils and corneal reflex.o Complete death notes on progress sheet and fill death certificate as early aspossible.Pre Rounds¾¾¾For pre-rounds allow 30 min to one hour before consultant rounds but it depends on noof patients under your care.Get your sign out from Night flat or cross cover team. You must know any major eventthat happened over night and this will dictate how you spend your time pre-round.Try to read relevant text for your patient from pocket handbook or guide beforeattending rounds.Occupational Risks¾¾¾¾Standard barrier nursing and isolation techniques should be employed in cases ofpatients with infectious communicable disease.These measures include:o Gloveso Maskso Careful needles/sharp objects handling.Prophylaxis in cases of exposure if indicated (e.g. meningococcemia)In case of mishap/exposure, event should be reported to consultant on call,immediately.Accountability¾In case of an incident, a committee of ward consultant will review the entire case indetail and will decide about warning/penalty.Ethical Issues¾Best interest of the patient should be watched, in case of conflict or confusion issueshould be discussed with consultant on call.Confidentiality Of Patient’s Data¾ Patient’s record and data should be kept confidential to watch his/her interests anddiagnosis prognosis should not be discussed with attendants without permission ofpatient/close attendant.- 21 -
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching HospitalsPatient Education¾ During in patient stay, every opportunity should be availed to educate patients andtheir family regarding their illness and management.Ward In-Chage Resident Duties¾¾¾¾¾¾Maintenance and cleanliness of all
STANDARD OPERATING PROCEDURES for Health Professionals and Teaching Hospitals - 5 - About the Authors Muhammad Umar MBBS, MCPS, FCPS, FRCP (L), FRCP (Glasg), FACG, AGAF Graduated in 1981 from Rawalpindi Medical College