Transcription
Prelims.qxd7/6/049:20 AMPage iAbdominal Ultrasound
Prelims.qxd7/6/049:20 AMPage iiFor Churchill LivingstoneCommissioning Editor: Dinah ThomDevelopment Editors: Kerry McGechieProject Manager: Morven DeanDesigner: Judith Wright
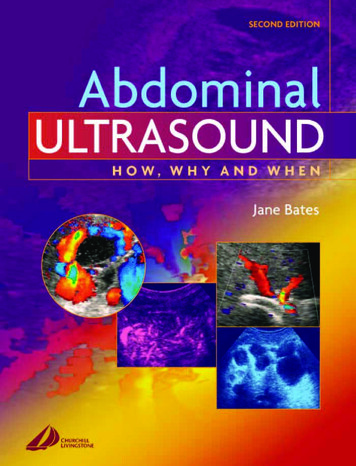
Prelims.qxd7/6/049:20 AMPage iiiAbdominal UltrasoundHow, Why and WhenSECOND EDITIONJane A. Bates MPhil DMU DCRLead Practitioner, Ultrasound Department, St James’s University Hospital, Leeds, UKE D I N B U R G H L O N D O N N E W YO R K O X F O R D P H I L A D E L P H I A S T L O U I S S Y D N E Y T O R O N T O 2 0 0 4
Prelims.qxd7/6/049:20 AMPage ivCHURCHILL LIVINGSTONEAn imprint of Elsevier Limited Harcourt Brace and Company Limited 1999 Harcourt Publishers Limited 2001 2004, Elsevier Limited. All rights reserved.The right of Jane Bates to be identified as author of this work has been assertedby her in accordance with the Copyright, Designs and Patents Act 1988.No part of this publication may be reproduced, stored in a retrieval system, ortransmitted in any form or by any means, electronic, mechanical, photocopying,recording or otherwise, without either the prior permission of the publishersor a licence permitting restricted copying in the United Kingdom issued bythe Copyright Licensing Agency, 90 Tottenham Court Road, London W1T4LP. Permissions may be sought directly from Elsevier’s Health SciencesRights Department in Philadelphia, USA: phone: ( 1) 215 238 7869, fax:( 1) 215 238 2239, e-mail: healthpermissions@elsevier.com. You may alsocomplete your request on-line via the Elsevier homepage (http://www.elsevier.com),by selecting ‘Customer Support’ and then ‘Obtaining Permissions’.First edition 1999Second edition 2004ISBN 0 443 07243 4British Library Cataloguing in Publication DataA catalogue record for this book is available from the British LibraryLibrary of Congress Cataloging in Publication DataA catalog record for this book is available from the Library of CongressNoteKnowledge and best practice in this field are constantly changing. As newresearch and experience broaden our knowledge, changes in practice, treatmentand drug therapy may become necessary or appropriate. Readers are advised tocheck the most current imformation provided (i) on procedures featured or(ii) by the manufacturer of each product to be administered, to verify therecommended dose or formula, the method and duration of administration, andcontraindications. It is the responsibility of the practitioner, relying on theirown experience and knowledge of the patient, to make diagnoses, to determinedosages and the best treatment for each individual patient, and to take allappropriate safety precautions. To the fullest extent of the law, neither thepublisher nor the authors assumes any liability for any injury and/or damage.The PublisherThePublisher'spolicy is to usepaper manufacturedfrom sustainable forestsPrinted in China
Prelims.qxd7/6/049:20 AMPage vvContentsContributors viiPreface ixAbbreviations xi1. Optimizing the diagnostic information 12. The normal hepatobiliary system 173. Pathology of the gallbladder and biliary tree 414. Pathology of the liver and portal venous system 795. The pancreas 1216. The spleen and lymphatic system 1377. The renal tract 1538. The retroperitoneum and gastrointestinal tract 1959. The paediatric abdomen 21510. The acute abdomen 24311. Interventional and other techniques 253Bibliography and further reading 275Index 277
Prelims.qxd7/6/049:20 AMPage viThis page intentionally left blank
Prelims.qxd7/6/049:20 AMPage viiviiContributorsRosemary Arthur FRCR Consultant RadiologistDepartment of X-ray & Ultrasound, The GeneralInfirmary at Leeds, Leeds, UKSimon T. Elliott MB ChB FRCR ConsultantRadiologist Department of Radiology, FreemanHospital, Newcastle-upon-Tyne, UKGrant M. Baxter FRCR Consultant RadiologistWestern Infirmary University NHS Trust,Glasgow, UK
Prelims.qxd7/6/049:20 AMPage viiiThis page intentionally left blank
Prelims.qxd7/6/049:20 AMPage ixixPrefaceUltrasound continues to be one of the mostimportant diagnostic tools at our disposal. It isused by a wide range of healthcare professionalsacross many applications. This book is intended asa practical, easily accessible guide to sonographersand those learning and developing in the field ofabdominal ultrasound. The most obvious drawbacks of ultrasound diagnosis are the physical limitations of sound in tissue and its tremendousdependence upon the skill of the operator. Thisbook seeks to enable the operator to maximize thediagnostic information and to recognize the limitations of the scan.Where possible it presents a wider, more holisticapproach to the patient, including presentingsymptoms, complementary imaging proceduresand further management options. It is not a comprehensive account of all the pathological processeslikely to be encountered, but is intended as aspringboard from which practical skills and clinicalknowledge can develop further.This book aims to increase the sonographer’sawareness of the contribution of ultrasound withinthe general clinical picture, and introduce thesonographer to its enormous potential.The author gratefully acknowledges the helpand support of the staff of the UltrasoundDepartment at St James’s University Hospital,Leeds.Leeds 2004Jane Bates
Prelims.qxd7/6/049:20 AMPage PCDKASTATAVBCSCAPDCBDCDCFCTDICDICOMDMSAautosomal dominant polycysticdisease of the kidneyalpha-fetoproteinacceleration indexacquired immune deficiencysyndromeAmerican Institute forUltrasound in Medicineas low as reasonably achievablealanine aminotransferaseanteroposteriorautosomal dominant (adult)polycystic kidneyautosomal recessive polycysticdisease of the kidneyaspartate aminotransferaseacceleration timearteriovenousBudd–Chiari syndromecontinuous ambulatoryperitoneal dialysiscommon bile ductcommon ductcystic fibrosiscomputed tomographydisseminated intravascularcoagulationDigital Imaging andCommunications in Medicinedimercaptosuccinic VINRIOUSIVCIVUKUBLFTLPVLRVLSLUQMCKDdiethylene triaminepenta-aceticacidend-diastolic flowendoscopic retrogradecholangiopancreatographyextracorporeal shock wavelithotripsyendoscopic ultrasoundfocused assessment withsonography for traumaFood and Drug Administrationframes per secondhepatic arteryhepatocellular carcinomahaemolytic anaemia, elevated liverenzymes and low platelet counthepatic iminodiacetic acidhypertrophic pyloric stenosishepatic veininternational normalized ratiointraoperative ultrasoundinferior vena cavaintravenous urogramkidneys, ureters, bladderliver function testleft portal veinleft renal veinlongitudinal sectionleft upper quadrantmulticystic dysplastic kidney
Prelims.qxd7/6/049:20 AMPage CSPBCPCKDPCSPDPIPIDPRFPSCPTLDPVRASRCCRFRHVmiddle hepatic arterymiddle hepatic veinmechanical indexmain portal veinmagnetic resonance angiographymain renal arterymagnetic resonancecholangiopancreatographymagnetic resonance imagingmain renal veinoutput display standardphotographic archiving andcommunicationsphotographic archiving andcommunications systemsprimary biliary cirrhosispolycystic kidney diseasepelvicalyceal systempancreatic ductpulsatility indexpelvic inflammatory diseasepulse repetition frequencyprimary sclerosing cholangitispost-transplantlymphoproliferative disorderportal veinrenal artery stenosisrenal cell carcinomaradiofrequencyright hepatic ICTIPSTISTORCHTSUTIVUJWRMSDXGPresistance indexright iliac fossaright kidneyright portal veinright renal arteryright renal veinright upper quadrantrenal vein thrombosissplenic arterysystemic lupus erythematosussuperior mesenteric arterysplenic veintuberculosistime gain compensationtissue harmonic imagingthermal indexbone-at-focus indexcranial indextransjugular intrahepaticportosystemic shuntsoft-tissue thermal indextoxoplasmosis, rubella,cytomegalovirus and HIVtransverse sectionurinary tract infectionvesicoureteric junctionwork-related phritisxi
ch01.qxd6/30/045:35 PMPage 11Chapter1Optimizing the diagnosticinformationIMAGE OPTIMIZATIONCHAPTER CONTENTSImage optimization 1The use of Doppler 2Getting the best out of Doppler 5Choosing a machine 6Recording of images 9Safety of diagnostic ultrasound 10Medicolegal issues 12Departmental guidelines/schemes of work 13Quality assurance 13Misinterpretation of ultrasound images is a significant risk in ultrasound diagnosis. Because ultrasoundscanning is operator-dependent, it is imperative thatthe sonographer has proper training in order toachieve the expected diagnostic capabilities of thetechnique. The skill of effective scanning lies in theoperator’s ability to maximize the diagnostic information available and in being able to interpret theappearances properly. This is dependent upon: Clinical knowledge—knowing what to look forand why, knowing how to interpret theappearances on the image and an understandingof physiological and pathological processes. Technical skill—knowing how to obtain themost useful and relevant images, knowledge ofartifacts and avoiding the pitfalls of scanning. Knowledge of the equipment being used—i.e.making the most of your machine.The operator must use the controls to their besteffect (see Box 1.1). There are numerous ways inwhich different manufacturers allow us to makecompromises during the scanning process in orderto improve image quality and enhance diagnosticinformation.The quality of the image can be improved by: Increasing the frequency—at the expense ofpoorer penetration (Fig. 1.1). Increasing the line density—this may be achievedby reducing the frame rate and/or reducing thesector angle and/or depth of field (Fig. 1.2).
ch01.qxd6/30/0425:35 PMPage 2ABDOMINAL ULTRASOUNDBox 1.1 Making the most of your equipmentUse the highest frequency possible—tryincreasing the frequency when examining thepancreas or anterior gallbladder.Use the lowest frame rate and highest linedensity possible. Restless or breathlesspatients will require a higher frame rate.Use the smallest field practicable—sectionsthrough the liver require a relatively wide sectorangle and a large depth of view, but when examining an anterior gallbladder, for example, thefield can be greatly reduced, thereby improvingthe resolution with no loss of frame rate.Use the focal zone at relevant correct depth.Use tissue harmonic imaging to increase thesignal to noise ratio and reduce artefact.Try different processing curves to highlightsubtle abnormalities and increase contrastresolution.Using the focal zones correctly—focus at thelevel under investigation, or use multiple focalzones at the expense of a decreased frame rate(Fig. 1.3). Utilizing different pre- and post-processingoptions, which may highlight particular areas(Fig. 1.4). Using tissue harmonics to reduce artefact (Fig.1.5). This technique utilizes the secondharmonic rather than the fundamental frequencyAusing either filtration or pulse inversion.1 Thisresults in a higher signal-to-noise ratio whichdemonstrates particular benefits in many difficultscanning situations, including obese or gassyabdomens.It is far better to have a scan performed properly ona low-tech piece of equipment by a knowledgeableand well-trained operator than to have a poorly performed scan on the latest high-tech machine (Fig.1.6). A good operator will get the best out of eventhe lowliest scanning device and produce a resultthat will promote the correct patient management.A misleading result from a top-of-the-range scannercan be highly damaging and at best delay the correct treatment or at worst promote incorrect management. The operator should know the limitationsof the scan in terms of equipment capabilities, operator skills, clinical problems and patient limitations,take those limitations into account and communicate them where necessary.THE USE OF DOPPLERThe use of Doppler ultrasound is an integral partof the examination and should not be consideredas a separate entity. Many pathological processesin the abdomen affect the haemodynamics ofrelevant organs and the judicial use of Doppleris an essential part of the diagnostic procedure.This is discussed in more detail in subsequentchapters.Colour Doppler is used to assess the patencyand direction of flow of vessels in the abdomen,BFigure 1.1 The effect of changing frequency. (A) At 2.7 MHz the wires are poorly resolved and the background‘texture’ of the test object looks coarse. (B) The same transducer is switched to a resonant frequency of 5.1 MHz.Without changing any other settings, the six wires are now resolved and the background texture appears finer.
ch01.qxd6/30/045:35 PMPage 3OPTIMIZING THE DIAGNOSTIC INFORMATIONABFigure 1.2 The effect of frame rate. (A) 76 frames per second (FPS). (B) 35 FPS—the resulting higher line densityimproves the image, making it sharper.ABFigure 1.3 The effect of focal zone placement. (A) With the focal zone in the near field, structures in the far field arepoorly resolved. (B) Correct focal zone placement improves both axial and lateral resolution of the wires.ABFigure 1.4 The effect of using post-processing options. (A) A small haemangioma in the liver merges into thebackground and is difficult to detect. (B) A post-processing option, which allocates the range of grey shades in a nonlinear manner, enhances contrast resolution and improves detection of focal lesions.3
ch01.qxd46/30/045:35 PMPage 4ABDOMINAL ULTRASOUNDABFigure 1.5 The effect of tissue harmonic imaging (THI): (A) a bladder tumour in fundamental imaging mode (left) isshown with greater definition and loss of artifact in THI (right). (B) In an obese patient, cysts near the gallbladder (left)are shown in greater detail using pulse inversion tissue harmonics (right). A small nodule is demonstrated in the lowercyst.to establish the vascularity of masses or lesionsand to identify vascular disturbances, such asstenoses. Flow information is colour-coded (usually red towards and blue away from the transducer) and superimposed on the image. Thisgives the operator an immediate impression of avascular map of the area (Fig. 1.7). This Dopplerinformation is obtained simultaneously, oftenfrom a relatively large area of the image, at theexpense of the grey-scale image quality. The extratime taken to obtain the Doppler information foreach line results in a reduction in frame rate andline density which worsens as the colour Dopplerarea is enlarged. It is advisable, therefore, to use acompact colour ‘box’ in order to maintain imagequality.Power Doppler also superimposes Dopplerinformation on the grey-scale image, but withoutany directional information. It displays only theamount of energy (Fig. 1.8). The advantage ofthis is that the signal is stronger, allowing identification of smaller vessels with lower velocityflow than colour Doppler. As it is less angledependent than colour Doppler it is particularlyuseful for vessels which run perpendicular to thebeam, for example the inferior vena cava (IVC).
ch01.qxd6/30/045:35 PMPage 5OPTIMIZING THE DIAGNOSTIC INFORMATIONABFigure 1.6 The importance of using the equipment properly. (A) Incorrect use of equipment settings makes it difficultto appreciate the structures in the image. (B) By increasing the resonant frequency, decreasing the frame rate andadjusting the focal zone correctly, a small rim of fluid around the gallbladder is seen and the gallbladder wall andvessels posterior to the gallbladder are made clear.Figure 1.7 Colour Doppler of the hepatic veinconfluence. The right hepatic vein appears red, as it isflowing towards the transducer. The left and middlehepatic veins are in blue, flowing away from thetransducer. Note the peripheral middle hepatic vein,which appears to have no flow; this is an artifact due tothe angle of that part of the vessel to the beam.Pulsed Doppler uses pulses of Doppler fromindividual elements or small groups of elementswithin the array. This allows the operator to selecta specific vessel, which has been identified on thegrey-scale or colour Doppler image, from which toobtain a spectrum. This gives further informationregarding the flow envelope, variance, velocityand downstream resistance of the blood flow(Fig. 1.9).Figure 1.8 Power Doppler of the hepatic veinconfluence. We have lost the directional information, butflow is demonstrated in all parts of the vessel—eventhose perpendicular to the beam.Getting the best out of DopplerFamiliarity with the Doppler controls is essential inorder to avoid the pitfalls and increase confidencein the results.It is relatively straighforward to demonstrateflow in major vessels and to assess the relevantspectral waveform; most problems arise whentrying to diagnose the lack of flow in a suspectedthrombosed vessel, and in displaying low-velocity5
ch01.qxd66/30/045:35 PMPage 6ABDOMINAL ULTRASOUNDABFigure 1.9 Flow velocity waveforms of hepatic arteries. (A) High-resistance flow with low end-diastolic flow (EDF)and a dichrotic notch (arrowhead). The clear ‘window’ during systole (arrow) indicates little variance, with the bloodflowing at the same velocity throughout the vessel. During diastole, the area under the envelope is ‘filled in’, indicatinggreater variance in flow. (B) By contrast, this hepatic artery trace indicates low-resistance flow with good EDF and nonotch. Variance is apparent throughout the cycle.CHOOSING A MACHINEFigure 1.10 On the left, the portal vein appears tohave no flow (arrow) when it lies at 90 to the beam—apossible misinterpretation for thrombosis. When scannedintercostally, the vein is almost parallel to the beam andflow is easily demonstrated.flow in difficult-to-access vessels. Doppler isknown to produce false-positive results for vesselocclusion (Fig. 1.10) and the operator must avoidthe pitfalls and should ensure that the confidencelevels are as high as possible (see Box 1.2).The ultrasound practitioner is confronted witha confusing range of equipment and choosingthe right machine for the job can be a dauntingtask.An informed and useful choice is more likelywhen the purchaser has considerable experiencewithin the particular clinical field. Many machines,purchased in the first enthusiastic flush of settingup a new service, for example, turn out to beunsuitable two or three years later.Mistakes are made by insufficient forward planning. A number of machines (usually at thecheaper end of the market), though initially purchased for specific, sometimes narrow, purposes,end up being expected to perform more complexand wider-ranging applications than originallyplanned.Take careful stock of the range of examinationsyou expect your machine to perform. Future developments which may affect the type of machine youbuy include: Increase in numbers of patients calculated fromtrends in previous years.
ch01.qxd6/30/045:35 PMPage 7OPTIMIZING THE DIAGNOSTIC INFORMATIONBox 1.2 Steps to take if you can’t detect flowwith Doppler Ensure the angle of insonation between thevessel and the transducer is 60 . Colour andpulsed Doppler are highly angle-dependent.Ensure the Doppler gain is set at the correctlevel. (Colour and pulsed Doppler gain settingsshould be just below background noise level.)Ensure the Doppler power/output setting issufficient.Ensure the pulse repetition frequency (PRF) isset correctly. A low PRF (‘range’ or ‘scale’ setting) is required to pick up low-velocity flow.Ensure the wall thump filter setting is low. (Ifthe setting is too high, real low-velocity flowis filtered out.)Use power Doppler, which is more sensitiveand is not angle-dependent.Know the limitations of your machine.Machines differ in their ability to detect lowvelocity flow.If in doubt, test it on a reference vessel youknow should contain flow.ultrasound-guided therapies which may berequired in future.The following points are useful to bear in mindwhen purchasing new equipment:Probe number and design (Fig 1.11)Consider the footprint, shape and frequenciesrequired: most modern transducers are broadbandin design, enabling the user to access a wider rangeof frequencies. This is a big advantage as this limits the number of probes required for a generalservice. A curved array probe is suitable for mostgeneral abdominal applications, operating in the3.5–6 MHz region. Additional higher-frequencyprobes are useful for paediatrics and for superficialstructures. A small footprint is essential if neonataland paediatric work is undertaken and a 5–8 MHzfrequency will be required.A biopsy attachment may be needed for invasiveprocedures, and, depending on the range of workto be undertaken, linear probes, endoprobes,intraoperative probes and other designs can beconsidered.Image quality Increase in range of possible applications, animpending peripheral vascular service, forexample, or regional screening initiative. Clinical developments and changes in patientmanagement which may require more, ordifferent, ultrasound techniques, for example,medical therapies which require ultrasoundmonitoring, applications involving the use ofcontrast agents, surgical techniques which mayrequire intraoperative scanning, increases ordecreases in hospital beds, introduction of newservices and enlargement of existing ones. Impending political developments bygovernment or hospital management, resultingin changes in the services provided, thefunding or the catchment area. Other impending ultrasound developments,such as the use of contrast media orThere are very few applications where this is not ofparamount importance and abdominal scanningrequires the very best you can afford. A machinecapable of producing a high-quality image is likelyFigure 1.11 Curved arrays (left and centre) suitable forabdominal scanning. A 5 MHz linear array (right) isuseful for superficial structures, e.g. gallbladder andanterior abdominal wall.7
ch01.qxd6/30/0485:35 PMPage 8ABDOMINAL ULTRASOUNDto remain operational for much longer than onecapable of only poor quality, which will needreplacement much sooner. A poor-quality image isa false economy in abdominal scanning.Other considerations include: System dimensions and steering. Therequirement for the system to be portable, forexample for ward or theatre work, or mobilefor transportation to remote clinics. Machinesused regularly for mobile work should berobust and easy to move. Moveable (swivel and tilt) monitor and controlpanel, including height adjustment for differentoperators and situations. Keyboard design, to facilitate easy use of therequired functions, without stretching ortwisting. Hand-held portable machines are an optionthat may be considered.Machine capabilities and functionsThe availability and ease of use of various functionsdiffer from machine to machine. Some of theimportant issues to consider when buying amachine include: probe selection and switching process, simultaneous connection of several probesdynamic frequency capabilitydynamic focusing control, number and patternof focal zonesfunctions such as beam steering, sector angleadjustment, zoom, frame rate adjustment,trackerball controlstime gain compensation and power outputcontrolscine facility—operation and size of memoryprogrammable presetstissue harmonic and/or contrast harmonicimagingbody marker and labelling functionsmeasurement packages—operation and displaycolour/power and spectral Doppler through allprobesDoppler sensitivityDoppler controls—ease of use, programmablepresetsoutput displaysreport package option.ErgonomicsGood ergonomics contribute considerably to thesuccess of the service provided. The machine mustbe usable by various operators in all the required situations. There is a significant risk of work-relatedmusculoskeletal disorders (WRMSD)2 if carefulconsideration is not given to the scanning environment (see p. 12). When choosing and setting up ascanning service, forethought should be given notonly to the design of the ultrasound machine, butalso to the seating arrangements and examinationcouch. These should all be adjustable in order tofacilitate the best scanning position for the operator.Maintenance issuesIt is useful to consider the reliability record of thechosen equipment, particularly if it is to operate inout-reach clinics, or without available backup inthe case of breakdown. Contacting other users mayprove useful.Various maintenance contract options and costsare available, including options on the replacementof probes, which should be taken into accountwhen purchasing new equipment.UpgradeabilityA machine which is potentially upgradeable has alonger, more cost-effective life and will be supported by the manufacturer over a longer period oftime. Consideration should be given to future software upgrades, possible effects and costs and otheravailable options for the future, such as additionaltransducers or add-on Doppler facilities.Links to image-recording devicesMost ultrasound machines are able to link up tomost types of imaging facility, whether it be a simple black and white printer or a radiology-widephotographic archiving and communications (PAC)system. There may be costs involved, however, inlinking your new machine to your preferred imaging device.
ch01.qxd6/30/045:35 PMPage 9OPTIMIZING THE DIAGNOSTIC INFORMATIONEquipment manufacturers now follow theDICOM standard. Digital Imaging and Communications in Medicine is the industry standard fortransferring medical images and related information between computers. This facilitates compatibility between different pieces of equipment fromdifferent manufacturers and potentially enablesthem to be linked up.RECORDING OF IMAGESThere are no hard and fast rules about the recording of ultrasound scans and departmental practicesvary. It is good practice for departments to haveguidelines for taking and retaining images withinindividual schemes of work, outlining the minimum expected.3The advantages of recording images are: They provide a record of the quality of thescan and how it has been conducted: theorgans examined, the extent of the scan, thetype and standard of equipment, the settingsused and other scanning factors. This can be aninvaluable tool in providing a medicolegaldefence. They provide an invaluable teaching aid. They help to ensure quality control withindepartments: promoting the use of goodtechnique, they can be used to ensure protocolsare followed and provide an excellent audit tool. They can be used to obtain a second opinionon difficult or equivocal cases and provide abasis for discussion with clinical colleagues. Generally speaking the recording of images isencouraged. It reduces the operator’s vulnerabilityto litigation and supports the ultrasound diagnosis.4 It is only possible to record the entire examination by using videotape, which is rarely practicalin larger departments. The operator must take theresponsibility for ensuring the scan has been performed to the required standard; any images produced for subsequent discussion are onlyrepresentative of the examination and have beenchosen by the operator as an appropriate selection.If you have missed a small metastasis in the liverwhile scanning, or a gallstone in the gallbladder,you are unlikely to have included it on an image.Choice of image-recording device depends onmany factors. Considerations include: The disadvantages are: The cost of buying, running and maintainingthe recording device or system. The quality of images in some cases may notaccurately reflect that of the image on theultrasound monitor. The scanning time must be slightly increasedto accommodate the taking of images. Storage and retrieval of images may be timeand space-consuming. Hard copy may be mislaid or lost.If the examination has been badly performed,the hard copy may demonstrate that too!image quality—resolution, grey-scale, storagelifecapital cost of the system—including the installation together with the installation of anyother necessary equipment, such as a processorcost of filmprocessing costs if applicable—this includes thecost of chemicals, the cost of buying and maintaining a processor and possibly a chemicalmixermaintenance costsreliability of the systemstorage of images in terms of available spaceand costlocation and size of the imaging systemother considerations—ease of use—mobility—colour capability—ability to produce slides/teaching aids—shelf life of unused film and stored images.Numerous methods of recording images are availableto suit all situations. Small printers, attached to ultrasound scanners, are easy to use, cheap to buy and runand convenient if the machine is used on wards ordistant satellite units. However, systems which produce hard copy, however good, are inevitably ofinferior image quality to electronic image capture.9
ch01.qxd106/30/045:35 PMPage 10ABDOMINAL ULTRASOUNDMulti-system departments are tending towards networked systems which produce high-quality images,and can be linked to multiple machines and modalities. These are, of course, more expensive to purchaseand install, but are generally reliable and produceconsistent, high-quality image.Ultimately, the goal of the filmless department isbeing realized in PACS (photographic archiving andcommunications systems). Digital imaging networks are convenient, quick and relatively easy touse. The image quality is excellent, suffering little orno degradation in capture and subsequent retrieval,and the system can potentially be linked to a conventional imager should hard copy be required.The number of workstations in the system canbe virtually unlimited, depending on the system,affording the operator the flexibility of transmitting images immediately to remote locations, forexample clinical meetings, outpatient clinics, etc. Itis also possible to download images from scansdone with mobile equipment, remote from themain department, on to the PACS.Digital storage and retr
Ultrasound continues to be one of the most important diagnostic tools at our disposal. It is used by a wide range of healthcare professionals across many applications. This book is intended as a practical, easily accessible guide to sonographers and those learning and developing in