Transcription
NursingInnovation.UofUHealth.org10creativenursing ideasthat helped transform an entire health systemUniversity of Utah Health Care50 N. Medical DriveSalt Lake City, UT 841322011Nursing Report
1. Run your nursing departmentlike a business. page 52.Nurses should walk in theirpatients’ shoes. page 83.For patients, the little thingsmean a lot. page 1110 creative nursing ideas that helpedtransform an entire health system.4. The nurses you’re searching forare right inside your hospitalwalls. page 155. Transform your float pool into ahighly trained SWAT team.page 176. Open more beds when youneed them. Close them whenyou don’t. page 217. Use more video cameras andfewer patient sitters. page 238. Prevent falls with signedpatient agreements. page 259. Put nurse, physician, andresearcher heads together forbetter patient outcomes. page 2710. Let nurses step outside oftraditional roles. page 30
A message from our ChiefNursing Officerimplemented. We put nurse leaders in non-traditionalroles, set great expectations and then watched themexceed our expectations. We also acknowledgedthat clinical nurses know what their patients need,both physically and emotionally. And with thisnew perspective, my role as a leader became that offacilitator and barrier remover.“Every patient shouldfeel like they’re ourfavorite patient.”Five years ago, the nursing department at Universityof Utah Health Care began a journey to be nationallyknown for the professional practice of nursing. Welooked at our current practice and began imaginingwhere we wanted it to be. We knew that excellencewas not a plaque on the wall, but a feeling thateveryone would notice—a palpable culture thatcombined unsurpassed clinical outcomes with a newlevel of care that made every single patient feel thatthey were, in fact, our favorite patient.Quality and accountability study among academic medical centersranked by the University HealthSystem ConsortiumUniversity of UtahHealth Care2010 / 1st out of 982009 31st out of 9312008 50th out of 88Transformingpatient care.Five years later, the answer is yes. In addition to ranking#1 for most improved patient satisfaction, Universityof Utah Health Care is currently ranked #1 in qualityamong academic medical centers. We did it by thinkingcreatively, working together, and empowering every staffmember from every level of the organization.20282010CentersTo drive transformation, our nursing departmentlooked at everything we did through a single lens: thepatient experience. From our professional practices toeducational opportunities to physical spaces, everythingwas subject to change. And every change we made hadto answer the ultimate question: Will it improve ourpatient care?20CentersFive years ago when we began this journey, Universityof Utah Health Care was an excellent medical center.But something was missing. Although we’d alwaysprovided outstanding care, our quality and patientsatisfaction scores ranked us in the middle of the packfor academic medical centers. We knew we could dobetter—much better.CentersMargaret Pearce, RN, Ph.D.Chief Nursing Officer#1 in Quality in the NationCentersTo build on this strategy, we worked hard to createa culture where anyone in our organization couldcontribute creative ideas that would be valued andI look forward to hearing from you.How do you measure quality? Here at University ofUtah Health Care, it’s not just reflected in our dataand metrics. It’s the smile on a patient’s face. It’s a huggiven freely to a family member in crisis. It’s nursesand physicians and researchers and administratorsall working together to deliver an exceptional patientexperience along with superior clinical outcomes. Andit’s what we do, each and every day.CentersWe also looked at our financial situation anddetermined where we needed to be in the future tocontribute to the healthy, vibrant organization weall envisioned. We started with a strategic plan fornursing, we identified gaps and we put a laser focus onthree areas: patient experience, quality outcomes andfiscal responsibility.As we shifted our focus, things began to change—slowly at first, then more dramatically. This year,we were honored to be named #1 in Quality by theUniversity HealthSystem Consortium for our clinicaloutcomes, as well as Top Improver by Press Ganey forour dramatic rise in patient satisfaction. Now, we’dlike to share some of the ideas that got us to this pointin our journey, and we’d love to hear your great ideasas well. Please take a look at the top 10 creative ideasthat helped transform our organization. Then, takea moment to share your ideas with us atNursingInnovation.UofUHealth.org.Where creativenursing ideasflourish.Developing creativenursing ideas.Some of the changes we made seemed too small tomake an impact—like giving needy families a free meal.Others seemed too monumental to get approved—likebuilding a multi-million dollar ICU. But when theidea was the right thing to do for the patient, we gotit done. And with every change we made, somethingremarkable happened: our satisfaction numbers shot up,our operational costs went down, and our professionalpractice flourished.How, exactly, did we do it? Read on to discover thecreative ideas behind our remarkable transformation.2011 nursing report / 3
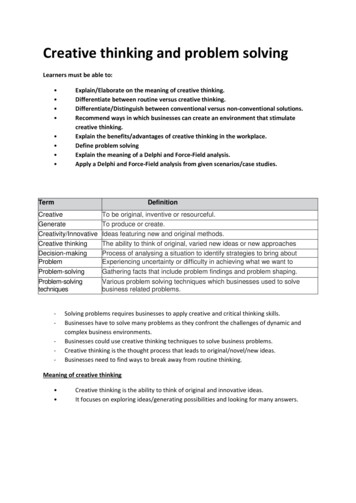
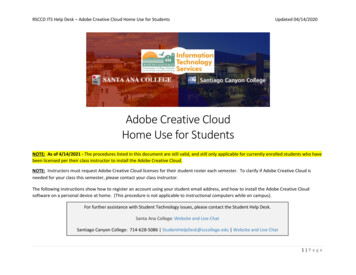
Collaboration is king: Clinical nurse Brooks Lloydand financial analyst Eric Allen work together to solveproblems—and improve quality.01. Runyour nursingdepartment likea business.“Everything we do is for our patients. Butin order to do it, our hospital must stayfinancially viable.”—Eric Allen, Senior Business Financial AnalystHospitals aren’t like typical businesses. Theydon’t sell merchandise. And they don’t slashprices. Instead, they have a clear, singularmission: To care for people.But here’s the conundrum: In order to providethe best patient care, hospitals must think andact like the best-run businesses—and that’s notalways easy for organizations that think and actlike, well, hospitals. “Hospitals need more thanjust a clinical model,” says Margaret Pearce,our CNO. “They also need a business model.”And that’s exactly what we created for ournursing department.Building a 5-yearbusiness plan.Together, we developed a nursing businessplan devoted to making our hospital nationallyknown for the professional practice of nursing.We identified gaps in quality, efficiency, andpatient satisfaction, and we used them to driveour strategy for improvement. We knew that toachieve our ultimate goal of providing excellentcare without compromise, we’d have to add twomore goals: improving our fiscal responsibility andincreasing our quality outcomes.2011 nursing report / 5
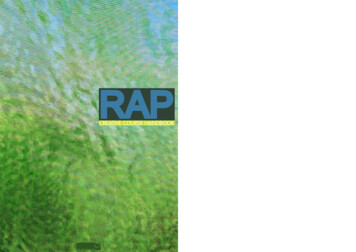
01. Run your nursing department like a business. (cont.)Global staffing changed all that. We put our entirenursing department on a centralized staffing grid andmade hospital-wide staffing decisions based on ourcensus status to ensure an ideal nurse-to-patient ratio.With this one change, we were able to optimize ourstaffing 24 hours a day. 305M ( 38%)1. Analyze the datanueListen to staff concerns, examine financialperformance data, and pinpoint any gaps in qualityor patient safety.reveNet2. Develop a pilotTry out the new idea on one unit and measureresults. Pa3. Expand the program 1.2 Million Saved—By predicting vacanciesand staffing globally,we’ve increased our labormanagement efficiencies,resulting in annual savingsof 1,248,000.96,700Nursinlabor gcosts 73M 70M ( 4%)2011Bring the idea to other units after a pattern ofsuccess has been established with the pilot.With centralized, global staffing and smaller, flexible nursing pods on each unit, University of Utah Health Care has a healthier financialoutlook than ever before, taking care of 11% more patients with 4% less labor—a reduction in nursing labor costs of 100 per patientday.Improve efficiency—and quality—with smaller,more flexible units.To further improve efficiency and staffing, we designedeach of our new units with three smaller pods and threeseparate nursing stations. Now, if our census is low, wecan simply shut down a pod—so we don’t have to staffup on a unit that’s not fully loaded. This strategy can beused in conjunction with the opening and closing of ourFlex Unit (see Idea #6).6 / 2011 nursing report107,000 ( 11%)aystdtien 220M For a hospital to stay financially viable, everydepartment—and every person within that department—must work efficiently. But we couldn’t get there when westaffed nurses unit by unit. We’d bring in agency nursesonly to find that we didn’t need them. We’d staff up tomeet a perceived need only to find that we had too manynurses for the tasks at hand. We’d send nurses home onone unit, while hiring someone new on another. It didn’tmake sense.We’ve developed each of our creative nursing ideas witha structured, systematic approach. Here’s how we do it:2010When it comes to staffing,look at the big picture.Increased revenue, decreased costs2009Our nurses worked closely with the process engineerson our Performance Excellence Team to identifyways to work smarter, leaner, and faster—all whileproviding better patient care than ever before. Weassigned a quality specialist to each unit to ensureconsistent collaboration, ongoing analysis, and continualimprovement. “No one is sitting in an office, evaluatingdata and telling nurses what to do,” says MikeSwanicke, a management engineer on the PerformanceExcellence Team. “We’re working together tosolve problems.”Improvement isa science.2008Bringing nursing expertsand process expertstogether.But that’s just the beginning. Our pods also allow us toco-locate patients based on their clinical needs, so we canassign specialized nurses to very specific areas. What’smore, the smaller pods keep nurses in closer proximityto their patients and create a quieter and less chaoticenvironment. “It’s a great way to give more personalizedcare,” says Margaret. “And it’s incredibly cost effective.”2011 nursing report / 7
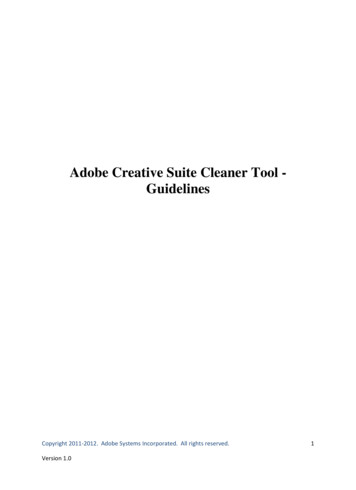
02. Nursesshould walk intheir patients’shoes.Nurses can’t go through the difficult work of treatingpatients if they don’t care about them. And while ournurses have always cared about our patients, it simplywasn’t showing five years ago like it should have.Our patient satisfaction numbers were uncomfortablylow—and to turn them around, we knew we needed tobetter connect with the emotional needs of our patientsand their families. So we created a whole new type ofprofessional development for our nurses, and we called itempathy training.Compassion ascurriculum.Nurses are constantly building their clinical skills, butthat’s only part of what they need to be successful. Withempathy training, we help them understand what it feelslike to be in a hospital and to feel angry or scared orconfused or helpless or alone. In other words, we helpthem understand what it feels like to be a patient.During the training, nurses are given real-world patientscenarios. They’re asked to put themselves in thepatient’s shoes and think about what that person mightbe feeling. Then they identify any barriers that couldkeep them from meeting that patient’s needs—and theydiscuss ways to break them down.8 / 2011 nursing report“ It’s a transformational experience. It’s a chancefor nurses to stop and think about just how hardit is to be a patient.”—Teri Olsen, Director of Project DevelopmentChanging personalattitudes—andprofessional practices.Empathy training shifts nurses’ personal thinking andprofessional actions. At the end of each session, nursesare asked to commit to this new perspective by statingwhat they’ll stop doing as well as what they’ll startImagine that You come to the hospital for the birth ofyour second child, and your wife diesduring labor. You need emergency surgery, but youdon’t have enough insurance or moneyto cover the medical bills. You get in a serious car accident, wakeup in the ER, and learn that you’reparalyzed.These are just a few of the real-world patient scenariosthat we work through during empathy training.Getting to the heart of the matter:Like all of our nurses who’ve beenthrough empathy training, Tammy VanTassel knows that emotional care is justas important as clinical care.doing. Through this practice, we’ve made hundreds ofbig and small changes to our nursing practices—fromavoiding medical jargon, to saying “I’m sorry,” to givinga hug. “With empathy training, our nurses have a chanceto reach inside of themselves and really identify withtheir patients,” says Teri. “And that has made all thedifference.”
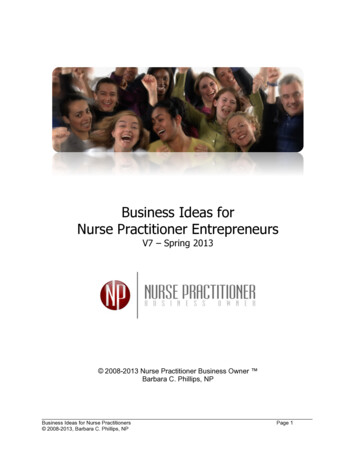
02. Nurses should walk in their patients’ shoes. (cont.)03. For patients,the little thingsmean a lot.Nurses usually know what their patients need. Theproblem is, they haven’t always known exactly howto go about giving them those things—especially whenthose things are related to guest services, not clinicalcare. We decided to change that.As part of our nursing business plan to boost patientsatisfaction scores, we stopped asking consultantsand executives what our patients needed, and westarted asking our bedside nurses. We created a PatientExperience Team comprised of high-performing nurseson each unit, who became our “unit champions,” andwe let them tell us exactly what needed to change.Food, shelter,clothing and a better comb.Championing compassion: Christine Pettit, unit championand clinical nurse coordinator for Women’s & Children’s Services,knows that small gestures of empathy can have a big impact onpatient satisfaction.Patient satisfaction isn’t just measured by numbers on a chart.It’s also measured by the hugs, smiles, and thank yous wereceive each and every day.10 / 2011 nursing reportBy surveying patients and staff throughout the hospital,our Patient Experience Team pinpointed a number ofsmall kindnesses and conveniences that brought bigsmiles—or simply a sigh of relief. We started giving freecafeteria meal coupons, pre-paid phone cards, and evenfree hotel stays to families who seemed to need them.We gave cards to patients who were spending theirbirthdays in the hospital. We provided new clothes fortrauma patients to go home in. We upgraded the flimsycombs in patient rooms.“When a new mom can’t leave the hospital as soon asexpected, we do everything we can to make her stay alittle easier,” says Christine Pettit, unit champion andclinical nurse coordinator for Women’s & Children’s2011 nursing report / 11
Ready to help: When Clinical Nurse Coordinator TrevanBiddulph needs a little something extra for a patient, he knowsexactly where to turn: The Patient Experience Resource Book.03. For patients, the little things mean a lot. (cont.)Services. “Sometimes a seemingly small gesture cangive her the extra comfort and emotional support sheneeds—like providing a conference room or gatheringspace for dad and the kids, so that extended familymembers can be in the room visiting the mother.”Making it easy for nursesto help guests.Giving extra help and services to patients and familiesis a relatively easy way to boost satisfaction. But it onlyworks if every nurse on every unit knows about thesespecial guest services and feels empowered to offer them.That’s where the Patient Experience Resource Bookcomes in. It outlines all of the special services nurses canoffer to patients and families. Even better, it’s stockedwith the tools nurses need to make it happen—like mealcoupons and new birthday cards. So making someonehappy can be as simple as opening a book.“Spending a littledowntime in a patientroom, especially in themiddle of the night,can help someonefeel a little lesshomesick, and a lotmore comfortable.—Christine Pettit, Unit Champion and Clinical NurseCoordinator for Women’s & Children’s ServicesBuilding patient satisfactionUniversity of Utah Health Care National Percentile RankPress 920102011 YTDWhite nursing uniformscreate positive patientperceptions.color. Ultimately, they chose three color options forpants, along with all-white tops; not because theyloved the color white, but because they felt it was theright thing to do for our patients.Patients don’t judge nurses just based on their clinicaltraining or the letters behind their names. Like all ofus, they make judgments based on first impressions.And research shows that they perceive nurses inwhite uniforms as more professional and competentthan nurses in scrubs. Uniforms also help patientsdistinguish their nurses from their nursing assistants—or any other staff that enters the room. 107,000 saved injust two yearsFor those reasons, we decided to eliminate ourhospital’s chaotic rainbow of scrubs and put our nursesin consistent uniforms. But as part of our culture ofcollaboration, we let our nurses have the final say onBefore we moved to uniforms, it seemed likeeveryone in the hospital wore scrubs—fromhousekeepers and call center workers to RNsand physicians. Today, scrubs are used for theirintended purpose: surgery. This simple changehas significantly decreased the amount wespend on scrubs.Also in 2010, University of Utah Hospital was named Top Improver byPress Ganey for our dramatic rise in patient satisfaction.12 / 2011 nursing report2011 nursing report / 13
04. Thenurses you’researching forare right insideyour hospitalwalls.Look around your hospital. Really look. Look at thepeople making beds in patient rooms, drawing blood inthe phlebotomy lab, or wheeling patients to radiology.What if you could take the best and brightest of themand help them become RNs? And what if you couldfurther guarantee that they’d launch their RN careersright in your hospital?It might sound like a crazy idea, but that’s exactly whatwe did. It all started when one of our promising healthcare assistants, Trent Bassett, couldn’t get in to nursingschool. He had great grades and solid work experience,and yet he’d been rejected by multiple programs. Buthe didn’t come to us to complain. He came to us withan idea.Learning together: Trent Basset, a critical care nurse, mentors CarmenCannon, a student in our associate degree program. Carmen, who willearn her RN this year, worked as a food handler in our cafeteria beforebeing accepted into our RN program.A nursing assistantdriving change.We helped Trent create a program in our hospital calledFUUN—Future University of Utah Nurses. The groupmet to discuss nursing application strategies, hear fromadmissions counselors at local schools, and help eachother through the application process. The networkingand collaboration paid off. Within a year, all but oneFUUN participant had been accepted to nursing school.And today, Trent is one of our critical care nurses.A new kind of nursingschool is built.Through FUUN, we learned that there were plenty ofpeople, right within our own hospital walls, who wouldlove to help fill our nursing gaps if they could just getthe clinical training they needed. And so we took Trent’sidea and pushed it to the max: We created our very ownnursing program.2011 nursing report / 15
04. The nurses you’re searching for are right inside your hospital walls. (cont.)We knew that the difficulty for nursing hopefuls wasgetting an RN, and once that was accomplished, theRN-to-BSN program was more readily available. Sowe developed an RN associate’s degree program inpartnership with Salt Lake Community College and theUniversity of Utah College of Nursing.Now in its 4th year, our program is open only to currentUniversity of Utah Health Care employees, so staff withthe right grades and prerequisites have an easier way toget into school, get trained and get to work. We pay foreach student’s tuition and books with a single caveat:They must agree to work with us as an RN for threeyears after they graduate.“Students are elatedwhen they findout they have theopportunity to goto nursing school.We have been ableto help fulfill dreamsas well as fill opennursing positions.”—Tiffany Noss, Staff Development Educator,Clinical Staff Education“It’s a win for our staff and a win for our hospital,too,” says Tiffany Noss, who manages our studentprograms. “The program requires an investment ofabout 12,000 per student, but it pays for itself.” Indeedit does. According to the American Nurses Association,recruitment can range from 22,000 - 64,000 pernurse, depending on factors like turnover, unit specialtyor location. With a guaranteed pipeline of new nurses forour hospital each year, we save hundreds of thousandsin recruiting costs and our new RNs are busy continuingtheir education to BSN and beyond.Student success story:From cafeteria to clinicals.Carmen Cannon knew she wanted to be a nurse atUniversity of Utah Health Care, but there was only oneproblem. She didn’t have an RN, and she had no ideahow long it would take to get into a traditional nursingprogram. She didn’t want to give up, but she was havinga hard time moving forward. “I was working in thecafeteria at the U—I just wanted to get into the hospitalany way I could, and I knew I had to start somewhere.”When she got accepted to our Salt Lake CommunityCollege nursing program, she knew she was finally onher way to fulfilling her dream. “It was shocking andthrilling to get in,” she says. “The opportunity to receivefree tuition and books is pretty unbelievable.” Today,Carmen is finishing her program, confidently making itthrough her clinicals, and preparing for her next move:a doctorate in psychiatric nursing. “The SLCC programopened up more opportunities for me and other peoplelike me who work at the hospital,” she says. “And I’mforever grateful.”05. Transformyour float poolinto a highlytrained SWATteam.Five years ago, we managed our resource nurses inthe same way that most other hospitals in Americado it. We used them to float in, help out, andmove on. We gave them our routine, low-acuitytasks—so they weren’t overwhelmed, but theywere often overlooked for career advancementor special assignments. They were missing out onopportunities to their build clinical skills, and wewere missing our opportunity to get truly valuablecontributions from them.83 new RNs.60 more in the queue. 0 spent to recruit them.University of Utah Health Care currently has 74graduates from our associate’s degree programworking as RNs in our hospital, and 60 morestudents in the queue to become our new RN hires.Because they’ve agreed to work for us for threeyears after graduating, we’ve saved 3 million 9.1 million in recruitment costs.All that changed when we made the decision toturn resource nursing into a career path, not justa fill-in job. “Our resource nurses have alwaysreceived essential education, but they weren’talways offered advanced, specialized training,”says Karen Nye, manager of resource nursing.“Today, they’re some of the most highly trainednurses in our hospital.” And that means we’ve gota team of flexible professionals who are ready totake on any challenge—from critical care ICU casesto highly specialized burn procedures.Training to the max: Resource Nursing Manager Karen Nye, picturedwith nurse Jacob Moon, makes sure that every resource nurse has theopportunity to pursue specialized, advanced education.16 / 2011 nursing report2011 nursing report / 17
05. Transform your float pool into a highly trained SWAT team. (cont.)they’re the perfect candidates for the job. And we’regiving them the education they need to be part ofthat team.“Our resource nursesare the hospital’sSWAT team: highlytrained, autonomous,and ready foranything.”“We’re changing the way people think about resourcenursing,” says Karen. And we’re changing the wayresource nurses work in our health system. Gone are thedays when unit nurses would have to take time out oftheir shifts to show the float staff what to do. Instead,our resource nurses can teach them a new skill or takeon a challenging patient. “They add real value to ourprofessional nursing staff,” says Karen. “They’re anintegral part of our critical care service line.”—Karen Nye, Manager, Resource NursingFrom standing at thebedside to soaring overthe Wasatch mountains.Schedule proactively, notreactively.Our resource nurses can receive specialized certificationsfor our ER, ICU, burn and neurology units. And withour new AirMed track, we’ve taken resource trainingeven higher. “AirMed needs highly specialized nurseswho also possess incredible versatility,” says Karen.“Our resource nurses work all over the hospital and canperform many specialized procedures.” In other words,In order to work more efficiently than ever before, andto provide even more value from our resource nursingstaff, we’ve taken a big-picture approach to resourcescheduling by staffing a full month ahead of time.“There’s no more scrambling,” says Karen. “Our nursescan look at the schedule, choose where they want towork, and help us fill known, active holes instead ofperceived holes.”Overtime hours decrease for five ICU units62% reduction inovertime hoursAverage overtimehours a week454035302520151050Rollout of prescheduling begins.The front lines of critical care: With our new AirMed track forresource nurses, every nurse at our hospital gets the training they needto build a dream career. Pictured here: Amanda Lawrence, Flight Nurse.Before implementing pre-scheduling, our ICU unitsaveraged 42 hours/week of overtime. Now, theyaverage 16 hours/week of overtime. 102,000 saved annuallyProactive scheduling has enabled our hospital tosave 102,000 annually in overtime pay costs—justin our ICU units /11Overtime hours for our five ICU units have decreased significantly since the implementation of proactive scheduling for resource nursing staff. Overtime hoursincreased temporarily in February and March during the transition of an additional unit to the resource pool.18 / 2011 nursing report2011 nursing report / 19
A flexible (and satisfying) solution: Tracey Nolen, nurse managerfor the Flex Unit, helps every patient on the unit know that they’vecome to exactly the right place.06. Open morebeds when youneed them.Close themwhen you don’t.When it comes to patient census, every hospital unithas its sweet spot—the number of patients that ismost productive and efficient. Problem is, it’s all tooeasy to find your units operating in a very sour spot—understaffed and stretching human resources toothin, overstaffed and unnecessarily wasting financialresources, or worse: completely maxed out and turningpatients away.It’s a situation that’s bad for patients, bad for nurses,and bad for business. And it’s the situation that droveUniversity of Utah Health Care to create a brand-newmode of operation: the Flex Unit, a 13-bed unit thatopens and closes based on the daily hospital census.Boosting hospital-wideefficiency.Nolen’s flexible, use-only-what-you-need solution turnedout to be a million-dollar idea. Literally. Staffed by thehospital’s committed, highly trained resource nurses, theFlex Unit has helped the hospital to consistently run atits sweet spot and save over 1,084,000 in staffing costs.At the same time, the unit boasts a patient satisfactionrate of 99%—one of the highest in the hospital.“Our patients aren’ttasks. Our patientsare people.”—Tracey Nolen, nurse manager, Flex Unit“We couldn’t keep thinking the same way and expectingdifferent results,” says Tracey Nolen, Nurse Managerof the Flex Unit. “The critical red census alerts wereunacceptable. Going on divert was unacceptable.”2011 nursing report / 21
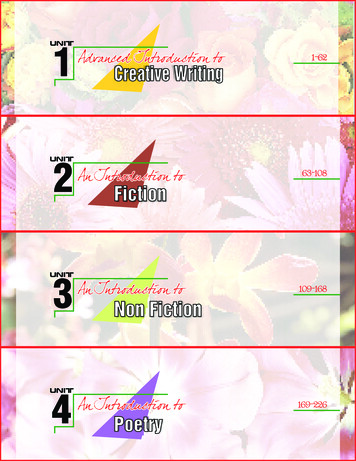
06. Open more beds when you need them. Close them when you don’t. (cont.)Building an overflow unit 1,084,000 savedthat patients actually love. As a 13-bed unit that can be opened or closed basedAt many hospitals, getting “stuck” on an overflow unitleads to low patient satisfaction marks. But that’s notthe case on the Flex Unit. “The patients who come to usare really sick and often unhappy,” says Tracey. “Thehospital is the last place in the world that they wantto be; especially if they feel like they’ve been put in thewrong place due to overcrowding. It’s our job to turnthat around.” Citing excellent clinical care as a basicpatient expectation and right, Tracey talks about howher Flex Unit nurses consistently exceed that expectation.“Our nurses understand the risk of low patientsatisfaction on an overflow unit, and they go the extramile to make sure the emotional needs of patients andfamilies are met,” says Tracey. It could be grabbingsnacks for a tired, hungry family. Or providing newclothes for a trauma patient to go home in. “Ourpatients on the Flex Unit have lost their control,” saysTracey. “We look for ways to give some of it back—andto give them back their dignity. Above all, we alwaysremember that our patients aren’t tasks. Our patientsare people.”on hospital need, the Flex Unit helps every unit inthe hospital to run at its sweet spot—providing moreefficient care, without spending more money.In an overflow unit where patients could easily begrumpy, if not downright angry, the Flex Unit has madeeach patient feel like they are welcome, cared for, andexactly where they should be—which is why patientsatisfaction consistently soars03. For patients,the little thingsmean a lot.A consistent, watchful eye: Elizabeth Armour-Roth (right), nurse manager of the Neuro Acute Care Unit, trains health care assistant Kara Andrews onvideo monitoring protocol. All staff members on the unit follow consistent procedures to ensure patient safety.07. Use morevideo camerasand fewer patientsitters.When we started extolling the virtues of videomonitoring, skepticism was understandably high. Howcould we possibly replace human sitters with impersonalvideo cameras? If we didn’t have someone in the room,could we really keep patients safe? Would we be able torespond quickly enough? And how would our patientsfeel about being on camera 24/7?22 / 2011 nursing reportWe answered these concerns in the same manner thatwe’d answered concerns about other innovative-butcontroversial ideas: We created a pilot program.2011 nursing report / 23
07. Use more video cameras and fewer patient sitters. (cont.)video m
like to share some of the ideas that got us to this point in our journey, and we’d love to hear your great ideas as well. Please take a look at the top 10 creative ideas that helped transform our organization. Then, take a moment to share your ideas with us at NursingInnov