Transcription
2013/14 – 2015/16 Business PlanHealth InformaticsVersion number: 0.7Lead author: Donna-Marie Jarrett Health Informatics Team1
Business Planning 2013/14 – 2015/16Contents PageChapter1Introduction2Service Strategy3Strategic Objectives:- Action plans4Integrated Planning2
1. IntroductionThe business plan was developed through a series of workshops and meetings with staff. Thedepartment’s heads of service met with their teams to identify and discuss the components of theSWOT analysis below. This fed into the discussions of the department’s senior management teamto identify our plans for the next three years.Consultation with the Trust’s 7 Divisions is planned to ensure that this business plan supports theirneeds.Strengths Excellent working and meeting environmentFlexible workforce – OoH training and supportavailable and staff are willing to go the extra mileStaff commitment to the provision of a good serviceGood working relationships with colleaguesResponsive to requests for assistanceStaff are well thought ofExperienced staff with years of combined TrustknowledgeConstantly building on strengths (e.g. procurementskills)Wide array of skillsHigh level of staff moraleSupportive Department Management always lookingfor positive solutions for the staffWeaknesses Opportunities To procure modern application development softwaretools to improve and accelerate bespoke applicationdelivery To achieve paper-light working practices within 3 years To fully exploit existing modern applications To identify more “quick wins” (i.e. low cost, minimalresource) To identify applications that can work on mobiletechnology To build on relationships with GPs (e.g. marketing ITTraining Services) To improve PM profile through celebrating oursuccesses To use project management skills to manageexpectations To use the PMO to support change management To modernise infrastructure with increased investmentin virtualisation and supporting network technologies(e.g. VDI) To promote the use of video-conferencing To exploit mobile working technologies To cross-skill existing staff To Channel pressure to deliver CIPS into innovationLack of an Informatics Programme BoardNot using technology effectively ourselves (e.g. no PM tool)Conflicting priorities impacting resources (e.g. broad scope of HIStrategy)Engagement with other staff groupsNo training/ development opportunities for existing staffSome services are reactive rather than proactiveNo contingency for specialist staffLack of administrative support – manageable but does have animpactExternal decisions leads to disjointed sequence of steps inachieving strategyLack of in-depth technical skills in some areasLimited resource for “quick turnaround” projectsAgeing infrastructure (including applications, software,hardware)Time wasted on process for Recruitment Agency and Bank usecan create over spendFunding not in place for Additional Clinics so creates over spendon budgetContinual lack of space is an on-going challenge for MedicalRecordsThreats Pressure to meet timescale expectations Lack of clinical engagement Although improved, too few senior clinicians and managers toparticipate in project governance HI viewed as a cost centre rather than as an investment HI not viewed as a priority by the Trust Increasing complexity and interdependency of systems EDM for staff who resist change and don’t embrace electronictechnology Fragmented Department No retention schedules in place for current offsite storage3
2. Service Strategy for 2013/14 – 2015/16IntroductionThe Trust is committed to providing excellence in patient safety, experience and outcomes. HealthInformatics strives to support the delivery of this commitment through the creation, shaping, sharing andapplication of patient, business intelligence and the deployment of appropriate technologies.In the 2011 Health Informatics Strategy, the Trust confirmed its aspirations to achieve an electronic patientrecord over the following 5 years as it recognised the benefits it would bring. The Trust is in Year 2 of thisstrategy and although there has been good progress, there is still a long journey ahead.2013-2016 Service StrategyOur Service Strategy is to:1. Empower our patients to better manage their own care2. Enable our clinicians to easily see the clinical context of what is happening to a patient3. Give the Trust confidence and the evidence to demonstrate that we are delivering the best possiblecare4. Improve shared decision making across care settings5. Develop divisional capabilities to interpret and understand what our Information reports are saying andwhere to target resources to address emerging issues6. Transform the Information Services team into an Business Intelligence team and creating a culture ofsensible analytics and standards for report production, eg validating and sense checking beforepublishing a report, ensuring that data sources and methodologies are referenced and how they havebeen applied7. Upskilling the Information Services through training, reinforce the alignment of Analysts with divisionsthrough attendance at performance meetings and increased visibility in providing day to day support8. Enable the Trust to take advantage of technologies that create opportunities to streamline inefficientprocesses and redirect resources to front line careDelivery of the above will focus on three clear objectives:1. Achieve a hospital-wide electronic patient record (EPR)2. Build Information Capability in the Trust3. Reviewing and establishing the right governance arrangements for Health Informatics programmes andprojectsThese objectives are expanded below.1. Achieving an EPRCurrent PositionPatient care pathways are supported by a mixed economy of paper and electronic data; a summarydescription is shown below:EmergencyA&E staff create handwritten CAS cards. For admitted patients all CAS cards are photocopied andsent with the patient to the ward for integration into the medical record. Diagnostic requests are4
processed either by Patient Centre/PAS or via handwritten forms. The record of treatmentprovided is handwritten. Results are printed out and inserted into the CAS cards even though mostresults are available by Patient Centre/PAS/Ice Desktop or Ward Enquiry. Discharge summaries areautomatically produced either electronically or populated via IPL if more information is required tobe conveyed to the GP. Documents are sent to the GP surgery using Docman where the GP has itimplemented.OutpatientsAppointments are booked either by Choose and Book or via phone/fax/letter into theAppointments Centre. Letters are sent to patients confirming their appointment details. Chronosautomated telephone service is used to remind patients of their appointments as well as a followup call from the Appointments team.Clinic lists are created on PAS/Patient Centre. Medical Records print out clinic lists for the nursingstaff. Diagnostic requests are currently done on paper, as are clinical findings of the Doctor whorecords these in the patient’s notes. Specialist charts, eg paeds growth, are completed by hand. Allclinical outcome administration is processed using forms – handwritten or typed. DNA, interconsultant referrals and discharge letters are dictated digitally in clinic and transcribed outside ofthe hospital. These letters are stored electronically and a copy sent to the GP using Docman but apaper copy is also placed in the patient’s medical record.InpatientsInpatients are recorded using PAS/Patient Centre. Admission letters are generated via PAS/PatientCentre. Discharge summaries completed in IPL and sent to GPs via Docman where implemented.All nursing and doctors notes are currently handwritten into the temporary patient notes file at theend of each bed. Nursing observations are currently handwritten. When discharged, all paperworkis filed into the medical record.External to the HospitalGP’s are able to use the Trust’s GP Browser module in PAS to lookup what is happening to theirpatients, including inpatients, outpatients and AE attendances. Not all GPs use this service.The Trust is currently submitting its A&E attendance data to Surrey PCT/NW Surrey CCG to enablean understanding of how GPs and patients are using the service. There is no health economy viewof a patient as none of the systems in primary, community and acute are joined up.Desired OutcomesAddressing the mixed economy of paper and clinical systems to achieve a hospital-wide EPR will: Empower our patients to better manage their own care because they will be able to see theirmedical history in one place Enable our clinicians to easily see the clinical context of what is happening to a patient Give the Trust confidence and the evidence to demonstrate that we are delivering the best possiblecare Improve shared decision making across care settingsMaking IT HappenWe will:5
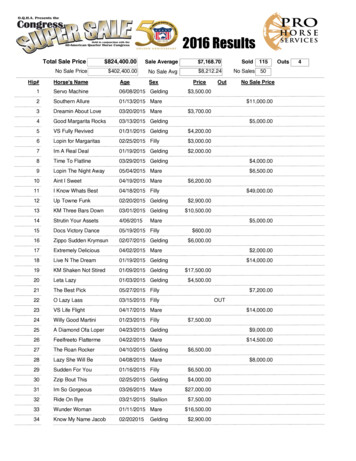
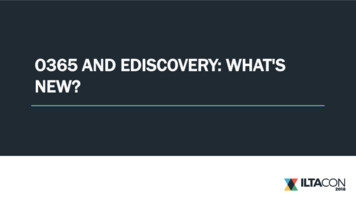
Reducing the burden of paper/manual processes on clinicians and their support staff by automatingclinical administrative processes, eg using workflow, eForms, eSignature technologies Transitioning away from paper to digital records Enabling the ‘easy’ capture of clinical activity at the point of care so it becomes second nature Procure and implement the right solutions to enable us to achieve:o the Clinical 5 necessary for a basic electronic patient recordo decision support product(s) to support our clinicianso electronic medical record solution via the Southern Collaboration for Electronic DocumentManagemento the support of the clinical workflowo the right technical infrastructure to enable clinicians to view patient information in contextacross all our clinical systems Enabling the easy and secure sharing of patient information across care settings by participating inthe South Integration Programme Apply the principal of ‘usability’ (relevant, natural, supportive, consistent, flexible) to everything wedo to “Working smarter” – exploring and exploiting opportunities for greater efficiency throughappropriate use of technology Continue the journey away from retrospective analysis of data to pro-active, predictive modellingand real-time intelligence “Sweat” our current clinical and corporate applications and infrastructure to achieve maximumreturn on investment Improve supplier management so as to achieve better value from existing contracts and to fullyexploit emerging opportunities with their products and services Ensure that the Health Informatics department has the right skills and competencies to deliver thestrategy over the next 5 years Deliver ‘business as usual’ services whilst implementing this business plan. Appendix ? contains adescription of these servicesThe diagram on the following page shows how this fits together.6
Achieving an EPR7
2. Building Information Capability in the TrustCurrent PositionInformation services currently provide a variety of statutory, regular and adhoc reporting to a variety ofcustomers both internal and external: The Trust Board (Board Report)Department of Health (Unify 2)Hospital Divisions (IPR)Contracting teamSpecialised Services (vascular, cardio, cancer)The scope of the service is currently only providing data reporting and not meaningful businessintelligence for decision making. The team is struggling with demand and has not been very good atmeeting deadlines.Desired OutcomesThe focus will be to transform the Information Service to one that is proactive, providing as near toreal-time intelligence as possible. As the demands on information services grow ever greater the needto work smarter and more efficiently has become essential. To meet this demand the InformationTeam has already put in place work streams that will automate and join together system processesenabling the speeding up of the production of statutory and regular reporting.QlikView has been implemented as the Trust’s main reporting tool providing full drill down capabilitiesincluding trust, divisional, speciality, consultant and patient levels. By continuing with the deploymentof QlikView, it is intended that reports generated will directly support operational management andany issues of performance. The key areas for the development are: Emergency Care pathwaysPlanned Care pathwaysLong Term Conditions18 weeks from referral to treatment (admitted non admitted pathways)DNA ratesMortalityEmergency Readmission ratesHospital acquired infectionsData QualityIt is imperative that QlikView becomes an integral performance tool that is used for the day to dayoperational management of the Trust. All relevant staff within the Trust will have access to QlikViewmetrics and activity – additionally with the ability to drill down to patient level and undertake their ownanalysis from their own desktop.This alone will allow the Trust to operate with a greater understanding of performance, activity anddemand. The most important benefits are: the development of divisional capabilities to interpret and understand what the reports are sayingand where to focus any remedial action(s)8
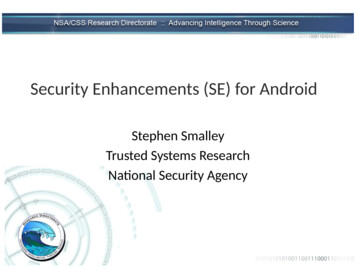
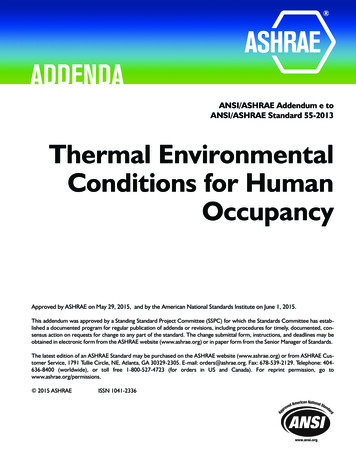
transforming the Information Services team into a Business Intelligence team through training andcreating a culture of sensible analytics and standards for report production, eg validating and sensechecking before publishing a report, ensuring that data sources and methodologies are referencedand how they have been appliedEssential in this development will be greater alignment of the Information Team with their divisions sothey fully understand the services provided and develop their specialty and pathway knowledge.Retention of staff will also be key to building up historical knowledge across the Trust.Making IT HappenWe will: Accelerate the implementation and embed the use of QlikView in the Trust so that it becomes anintegral performance tool that is used for the day to day operational management of the Trust. Provide appropriate access to QlikView metrics and activity so divisions can drill down to patientlevel data and undertake their own analysis from the desktop. Provide full training to all Trust Management staff, clinicians and the Information Services team.This will provide individuals with the knowledge, skills and ability to access relevant information, tosupport them to work effectively Minimise time spent on producing routine reports through the implementation of QlikView;enabling teams to develop their own reports. Information analysts will work with Divisions todevelop meaningful reports that inform rather than raise more questions than answers Reinforce the alignment of our Information Analyst to divisions to develop an understanding of thedivision specialties, pathways and operational issues and be visible in supporting the divisions attheir Performance Meetings; periodic rotation of Information Analysts into other divisions toensure well-rounded experience Provide the Information Services team will receive a structured training program so that theybecome information specialists. This will allow them to :o Understands data structureso Be experts in analysis and presentation of informationo Have in depth understanding of clinical processes, pathways and clinical informationsystemso Considers internal and external data sources – triangulate and benchmarko Be a bridge between information services and clinical areas – an important member of bothteamso Takes ownership of, and strive to improve the information recordedo Uses information to facilitate the understanding of service challenges and help focus onquality and productivity improvements Establish a Trust-wide Data Quality Group to ensure that we are capturing the right data, at theright time and that it is coded appropriately. There should be senior representation fromInformation Services, Finance and a Clinical specialist. This Data Quality Group will establish anaction log to enable it to be prioritised and performance managed by Operations supported byHealth Informatics.The diagram on the following page shows how this fits together.9
Building Information Capability in the TrustInformation driving decisionsInformation specialistsBuilding Capability Confidence for Clinical Ops staffClinical Systems Data Warehouse- the foundation -10
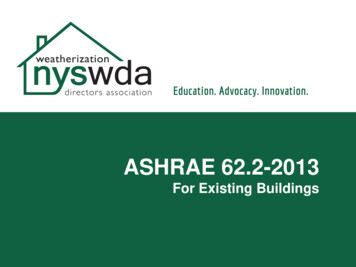
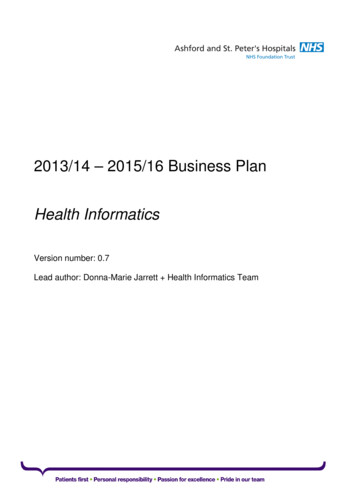
3. Establishing the right governance arrangements for Health Informatics Programmes ProjectsCurrent PositionThe Trust currently has an established Health Informatics Group, although this is not very wellattended. The work of the Health Informatics PMO is not very visible in the Trust. There are mixedperceptions about how effective the Trust PMO and the Health Informatics PMO are engaging withClinicians.Desired OutcomeTo establish the right levels of clinical engagement in Health Informatics projects and programmes,ensuring that clinical safety and clinical content are captured, issues addressed and benefits realised.Making IT HappenWe will: Work with our clinicians and operational colleagues to develop effective long term clinicalengagement that drives the strategic direction of health informatics Develop a plan for achieving the right levels of clinical engagement Propose a management framework for the implementation of health informatics projects andprogrammes that is fully inclusive of clinicians and operational staffThe diagram on the following page demonstrates work in progress and will be the subject ofconsultation with clinicians and operational staff.11
Proposed Governance for Health Informatics Programmes and Projects12
3. 2013/14 – 2015/16 Divisional ObjectivesCorporate Objective 1 – Highest Quality StandardsTo achieve the highest possible quality of care and treatment for our patientsActions to be takenPriorities for the Division in2013/14 – 2015/16 Ensure strong governance structure is inplace for informatics strategyRisks to deliveryYr 1 Review of Processes:oClinical Admin processesoClinical processes o Nursing processesDevelop new Service Model for MedicalRecords Ensure ProgrammeBoard is fully establishedand well attendedUndertake RiskAssessment of proposedclinical processesresulting fromimplementationsDevelop StakeholderPlan and AnalysisReview approach to GPReferrals & TWRReview of Order Comms;Clinical Record; CodingSheet; Ops Notes;Anaesthetic Records; ED;ePrescribingReview of nursingprocesses, in line withdeployment of NursingObs solution aboveCentralise managementof Health Records (adult,paeds, maternity)Prepare Staff TransitionplanStaff ConsultationCull Iron MountainArchiveResolve filing issuesDevelop feasibility studyand options appraisal forscanningDevelop financial modelYr 2Yr 3 DivisionalLead anddates ofcompletionLack of integration with Trust PMOPre Q1Pre Q1Pre Q1 Capacity to undertake the workLack of clinical engagement in thedevelopment and sign-off of processesLEPPre Q1Pre Q1Q1 Resistance to changeFunding for additional resources toenable the change to happenCapacity of Finance/CIP Manager to helpHI model the savings and expenditureCapacity to deliver given programme ofworkMGPre Q1Pre Q1Pre Q1Pre Q1Pre Q1DMJ/MGPre Q1Q1-Q2
Building Information Capability in theTrust Ensure IT infrastructure is resilient to determine approachRetender archive storageAccelerate theimplementation ofQlikViewProvide access to metricsso divisions can drilldown to patient leveldataProvide training to Ops,Clinicians and theInformation ServicesTeamInformation Analysts towork with Divisions todevelop meaningfulreportsReinforce the alignmentof Information Analystswith DivisionsProvide the InformationServices Team with astructured programmeof trainingEstablish a Trust-wideData Quality Group toensure that we arecapturing the right data,at the right time andthat it is codedappropriatelyComplete Core SwitchreplacementInstallation of resilientfibreOngoing development ofreporting and support forunderstanding the root causeof issues Ensure IT equipment is fit-for-purpose,maintained and supported Review Desktop StrategyImprove mobile working capabilities Develop Mobile DeviceBusiness CaseDevelop “Quick win”applications for mobile Move to single vendoredge switch and wifiReview fibre capabilityand replace if requiredIdentify further potentialfor mobile deviceapplicationsRoll out VDI to rest ofqualifying estate14Ongoing development ofreporting and support forunderstanding the root causeof issuesHead ofInformation DowntimeProcurementNetwork Design User acceptabilityAvailability of FundingLegacy software not compatibleProcurement processAvailability fundingSoftware not compatibleUser acceptabilityMFPre Q1MFMF
Improve access to multiple clinicalsystems devicesDeploy mobile devicesSeek approval for VDIrollout across campusInstall 250 user POCSeek approval for SingleSign On Business CaseProcure Single Sign Onsolution with ContextManagementDeploy Single Sign Onwith ContextManagement 15Selecting the right product to fit in withclinical portalStakeholder engagement at senior levelfor project board -conflicting prioritiesClinical engagementInteroperability with South IntegrationProgramme (Surrey-wide Clinical Portal)LEPPre Q1Pre Q1Q1 – Q2
Corporate Objective 2 – High Performing WorkforceTo recruit, retain and develop a high performing workforceActions to be takenPriorities for the Division in2013/14 – 2015/16Risks to deliveryYr 1 Developing the Workforce Clear roles and responsibilities forleadership Planning the Workforce Inspire and support the Workforce Yr 2Yr 3Identify funding for specialisttraining in the followingareas:oSpecialist IT skills(5 staff membersto attend)oSpecialist projectmanagement skills(Prince2 – 3 staffmembers)Continue to maintain highlevel of mandatory trainingcomplianceContinue to encourage ITTraining team to access freeof-charge external trainingfor Blend-IT and Microsoftexpert levelContinue to encourage seniormanagers to attend TeamBrief with cascade briefingsessions at weekly teammeetingsContinue to evaluateresources and retain staffContinue to encouragemorale boosting activitiessuch as bake-offs, crossdepartmental informalcelebrations Length of time required to recruit Budget overspend from using Agency Bank staff to cover posts whilstrecruitment process happens Access to funding for training Access to retention premiaDivisional Leadand dates EP/AM/MGongoingMF/LEP/AMongoingAllOngoing16
Corporate Objective 3 – Clinical StrategyTo deliver the Trust’s clinical strategy of joined up healthcareActions to be takenPriorities for the Division in2013/14 – 2015/16 Procurement and implementation ofnew clinical systems:oNursingRisks to deliveryYr 1 oEDM Yr 2Develop Business Caseand User Requirementsfor Nursing Obs solutionProcurement of NursingObs solutionCommence deploymentof Nursing Obs solution Complete Procurementof EDM solutionPrepare Health Recordsfor scanningCommence deploymentof EDM Complete deployment ofNursing Obs solution andswitch off paper (Q2)Yr 3 Lack of stakeholder engagement atsenior level for project boardAvailability of FundingAvailability of an off-the-shelf fit-forpurpose solution – may have to have abespoke solution developedDivisionalLead anddates ofcompletionLEPPre Q1Q1 – Q2Q3 –Q4Complete deployment ofEDM (Q1)All partners remaining in the collaborativeThis is a collaborative business case with FPHand HWPH, which could impact the directionof travelThe funding is coming from DH, with potentiallimitations/restrictions regarding scope,timingLEPQ1 – Q2Q3Q4 – Q1 2013Potential issues with drawing down capitalfundingoClinical Portal Business case approvalfor Clinical PortalProcure Clinical PortalCommence deploymentof Clinical PortalComplete deployment ofClinical Portal (Q3) Lack of Stakeholder engagement atsenior level for project board conflicting prioritiesClinical engagement – need to beinvolved in selecting the right productAvailability of FundingLEPQ1Q2-Q3Q4
Deployment of key departmentalsolutions Further deployment ofChoose and BookComplete deployment ofPatient Centre for OrderComms, Clinical Recordand Coding SheetFurther exploitation ofBluespier (ops notes,anaesthetic records,endometriosis)Planning andimplementation ofePrescribingComplete deployment ofDatixDeployment of Mobileworking for MidwivesComplete procurementof TranscriptionDeploy TranscriptionComplete deployment ofRealtime ED Capture EEG/ECG asdigital files Conflicting priorities for IT ProjectsTeamStakeholder engagement at senior levelfor project board – conflicting prioritiesClinical staff capacity to undertake thechange and embedLEPPre Q1 – Q2Pre Q1Pre Q1Pre Q1 – Q3Pre Q1Q1Pre Q1Q1Q118
Corporate Objective 4 – Financial sustainabilityTo ensure financial sustainability of the Trust through business growth and efficiency gainsActions to be takenPriorities for the Division in2013/14 – 2015/16 Achieve CIPRisks to deliveryYr 1 Prepare financialmodel forachieving CIPConsultant withdivisions on theimpactYr 2Yr 3DivisionalLead anddates ofcompletionDMJtba
Strategic ObjectiveCorporate Objective 1:Highest Quality StandardsCorporate Objective 2:High Performing WorkforceCorporate Objective 3:Clinical StrategyCorporate Objective 4:Financial SustainabilityDivisional KPI / Measure1.2.3.4.5.1.2.3.4.5.1.2.3.4.5.1.2.3.4.5.
5. Integrated Planning: Capacity Planning, Workforce and Financial planningUse the separate excel workbook for your Division on the T drive T:Capacity Modelling\2013-14 Business Planning to complete your plans for: Activity and capacity plans Transformation Plans Workforce Learning, Education and Development Needs Budget, new service developments and capital plans.Additional guidance notes for completion of each section are included in the Spreadsheet21
Appendix ?Service Delivery PlanService ProvidedDescriptionInformation ServicesInformation Services will be providing Statutory, Routine and Adhoc reporting available across theTrust. This includes the ongoing development and maintenance of the Trust’s central datawarehouse, associated reporting developments, data processing and cleansing services.During 2013-14 work will continue to move the Trust away from a reactive and retrospectivereporting function to a pro-active and predictive modelling, analysis and intelligence service.Information Services will provide an integrated approach to performance reporting and continue withthe development of the Integrated Performance Report, NHS Outcomes Framework, On-lineautomated Dashboards.Information Governance (IG)Providing the Trust with appropriate advice and guidance on compliance with UK and EU legislation,NHS standards and best practice for Information Governance. Achieving and maintaining NHS IGToolkit Level 2 compliance will be paramount as will developing detailed plans to achieve Level 3during 2011-12. A comprehensive IG Risk and Issues Logs will be maintained and used to ensurecompliance across all systems and processes. Day to day management of FOI and SAR requests,ensuring compliance with mandatory response times.Health RecordsDay to day management of the Trust’s medical records library, ensuring that clinical services havecomplete patient records at the time and place they are needed. As the Trust trials weekend clinics,the medical records service will need to respond to ensure continuity and support of those services.The requirement to have robust case note tracking and document management will be addressed inthe new Health Informatics Strategy.Clinical CodingAccurately coded episodes of care are pivotal in assessing clinical outcomes, safety of our workingpractices, quality and ensuring financial viability. It is essential that clinical coding occurs as near toreal time as possible and as close to the point of care as possible. We will therefore continue withour plans to co-locate our Clinical Coders into the Wards and Clinics. This will have the added benefitof assisting in the process of embedding Service Line Reporting across clinical areas. We will alsoconsolidate our expertise and knowledge by supporting our Clinical Coders in passing the nationalaccreditation examination. During 2012-13 we will also explore opportunities to generate incomegiven our excellent reputation and increasing demands from other Trusts for assistance.Clinical Coding will develop stronger links with Quality to further increase the clinical coding quality,income generation and reduce data quality queries.Information Technology (IT)Day-to-day management of a stable IT infrastructure, as well as constantly seeking and deliveringimprovements via upgrades and new technologies.This team consists of four streams:Programme ManagementService Level Management IT Support – includes IT Servicedesk, Desktop Support and Server maintenance Network and Systems (infrastructure) Applications Management (clinical systems) – includes Data Quality Web ServicesManagement and co-ordination of a portfolio of projects, some sourced from capital funding thathave been identified in the Health Informatics Strategy, others sourced from departmental budgets.The team focuses on both large Trust-wide projects as well as ensuring some smaller projects are alsotaken forward, with a view to ensuring on-going service improvement takes place at all levels. Thisteam includes the provision of the following sevices: informatics project management (project leadership and support) change management (process mapping and design) IT training (PAS, other clinical systems, ad hoc requests)Maintain and improve service quality through a constant cycle of agreeing, monitoring and reportingon service achievements and the instigation of actions to eradicate poor service. Ensuring thatHealth Informatics complies with the Scheme of Delegation achieves financial balance andcontributes towards the Trust’s CIPs targets.
Health Informatics strives to support the delivery of this commitment through the creation, shaping, sharing and application of patient, business intelligence and the deployment of appropriate technologies. In the 2011 Health Informatics Strategy, the Trust c