Transcription
Miss.kamlah1
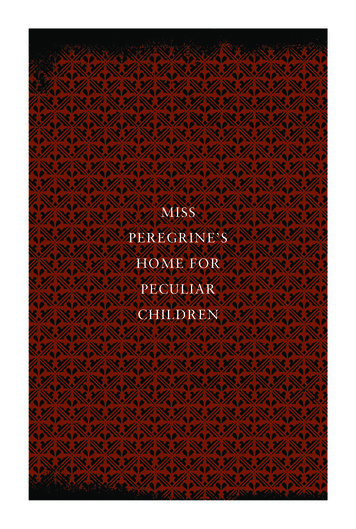
Trachoesophageal fistulaEsophageal atresia Esophageal atresia: Is a malformation that resultsfrom failure of the esophagus to develop as acontentious tube during the forth to fifth weeksof gestation.In this case the esophagus fails to lengthen andbecome separated. Instead it fused into thetrachea by fistula or may end in a blind pouch.It is associated with maternal history ofpolyhydrominous.Associated anomalies may occur including: heartdefects, urinary tract anomalies, &musculoskeletal anomalies.Miss.kamlah2
Miss.kamlah3
Symptoms in newborn includes: excessivesalivation & drooling, often accompanied withcyanosis, choking, & sneezing.During feeding, the infant returns fluid throughthe nose & mouth.Abdomen may become distended due to trappedair.Diagnosis is made by attempting to pass a 5 or 8French nasogastric tube into the stomach, thetube meets resistance.X-ray may show the associated defects.Echocardiogram & abdominal ultrasound may bedone to confirm the diagnosis.Miss.kamlah4
Management Intravenous fluid & antibiotic is started.Suction of the upper pouch of esophagus.Surgery is performed as soon as possible.By ligation of the fistula & connecting the two sidesof the esophagus.Complication may includes: gastroesophegeal reflux,aspiration.Miss.kamlah5
Nursing interventions 1.2.3.4.5.6.7.Esophageal atresia is a surgical emergency .Post operatively interventions includesmarinating airway by:Keeping suction ready to use, when needed.Place the head of the bed slightly lowered toprevent aspiration from secretion.Withhold oral fluidProvide IVF.Measure gastrostomy drainage.Administer antibiotic as ordered.Total parenteral nutrition may be needed untilfeeding is tolerated.Miss.kamlah6
The parents require emotional support.Teach the parents about the operation.Educated the parent about the function of theconnecting tubes after the surgery.Encourage the parents to participate in care.The infant may be discharged at home withgastrostomy tube.Educate parents about its care, feeding, signs ofinfections, & how to prevent complications.Miss.kamlah7
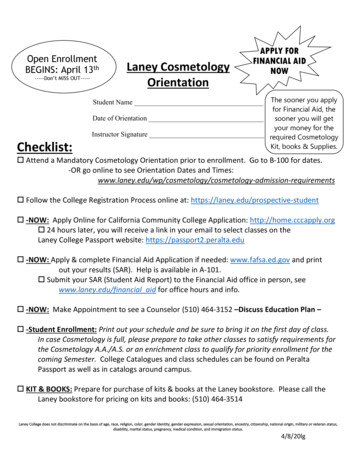
Inflammatory bowel diseases IBDCrohn’s Disease & Ulcerative Colitis IBD encompasses two distinct chronic disorders,Crohn’s Disease & Ulcerative Colitis, that have similarsymptoms & treatment.Genetics & environmental factors are involved in thedevelopment of IBD.Crohn’s disease is a chronic, inflammatory process. Itcan occur randomly throughout the GI tract, with theileum, colon, & rectum the most common sites.A distinct features of Crohn’s disease is thedevelopment of enteric fistulas between loops ofbowel or nearby organs.Miss.kamlah8
Miss.kamlah9
Mucosal ulcers began in small locations, & then grow insize & depth into the mucosal wall.The onset of Crohn’s disease is obvious crampyabdominal pain, followed by diarrhea. Other symptomsincludes fever, anorexia, growth failure of weightloss, general malaise, & joint pain.In serum analysis: anemia is common finding; inaddition to elevated ESR, hypoalbuminemia.Ulcerative colitis is chronic recurrent disease of thecolon & rectal mucosa of unknown etiology.Miss.kamlah10
The inflammation is limited to the mucosa along theentire length of the bowel with varying degree ofinflammation, ulceration, hemorrhage, & edema.The first symptoms is diarrhea. Lower abdominal pain,& cramping are present before & during a bowelmovement & are relived by the passage of stool &flatus.The stool is often mixed with blood & mucus. Wightloss or delayed growth, nutritional deficiencies, &arthralgia often occur as effects of the disease.Miss.kamlah11
Clinical Therapy Crohn’s disease & ulcerative colitis have periods ofremission & exacerbation.Treatment for both disease includes pharmacologicalinterventions (antibiotic, anti-inflammatory,immunosuppressive, & antidiarrheal medications). Andin sever cases, surgery.Nutritional therapy includes high protein, highcarbohydrate, low fiber diet with normal amount offat.Temporary colostomy may be performed to allow thebowel to rest.In ulcerative colitis, the removal of the diseasedbowel provides a permanent cure.Miss.kamlah12
Nursing Intervention Provide adequate stress reduction.Provide emotional support & counseling.Include body image in the plan of care.Teach the child the relaxation technique such as deepbreathing & verbalizing a favorite places.Teach parents about medication & diet.Several small meals better than three big meals.Limiting fiber intake to decrease motility.Offer high caloric meals if the child do not eat well.Watch for foods that cause intestinal problems &avoid them in the future.Miss.kamlah13
Constipation Decreased of the frequency of passage of the stool;the formation of hard, dry stool.Constipation is characterized by firm stool 2 timesper week for at least 2 weeks with no structural,endocrine or metabolic diseases.Babies with bottle feeding are more prone to hardstool than breast feed babies.Because stool patterns vary among children,identification of abnormal pattern is some timesdifficult. For young child, one bowel movement a daymay be normal. As the child grows, three to fourbowel movement in a week ,may be normal.Miss.kamlah14
Etiology & Pathophysiology Constipation may be caused by an underlying disease,diet, or psychological factors.It may be result from defects of filling or emptyingthe rectum.Pathological causes of defective filing includes:ineffective colonic propulsive activity, caused byhypothyroidism or use of medication obstructioncaused by structural anomaly.If rectum fails to fill, stasis leads to excessivedryness of the stool.The child may complain of vomiting, growth failureabdominal pain. An abdominal mass may be felt.Miss.kamlah15
Clinical Therapy Treat the underlying cause.Dietary management is the treatment of choice forconstipation with no underlying cause.Increasing fluid intake for infant & young childrenmay be effective.Removing foods that increase constipation such asbananas, rice, cheese from the child’s diet.Increasing the intake of high fiber foods such aswhole grain breads, raw fruits & vegetables.a single glycerin suppository or enema may be givento relieve hard stool & then dietary & fluidmanagements.Miss.kamlah16
Pharmacological managements of sever constipationusually occur over two stages:1- softening the hard stool by giving the childlactoulose.2- evacuation of stool by giving the child laxatives.## educate the family not to use these medicationfrequently, since overdose can cause boweldependency Behavior management:By changing the young child behavior in regarding totoileting by offering rewards.Placing the child on the toilet for 30 minutes after ameal Miss.kamlah17
Feeding disorders: Colic Is feeding disorder characterized by convulsiveabdominal pain of intestinal origin & sever crying.Episodes of colic usually occur between 2-6 weeks ofage & subsided by 3 months of age.It has unknown etiology, but predisposing factorscould lead to it, such as feeding too rapidly, &swallowing large amount of air.The infant cries loudly & continuously, often forseveral hours. The abdomen is distended & tense.Crying may stops when the child completelyexhausted or after passage of stool or flatus.Miss.kamlah18
Managements Management is supportive.Assess the child’s feeding pattern as well asfrequency of burping.Observe the family interaction with the child’s colicepisode.Assure the parents that they are not responsible forthe child condition, because they may blamethemselves.Positioning the child frequently, preventing suddenloud noises, avoiding smoking, offering pacifier,massaging the abdomen, providing warm bath, feedingsmaller amount with frequent burping would help indecreasing episodes of crying & colic.Miss.kamlah19
Celiac disease Is a chronic malabsorption syndrome, it isimmunological disorder that characterized by anintolerance for gluten (protein found in wheat, oats &barley).Inability to digest gluten result in accumulation ofthe amino acid glutamine, which is toxic to themucosal cells in the intestine.Leading to damage of the villi ultimately impairs theabsorption process in the small intestine.In early stages, celiac disease affect the absorptionof fat, leading to execration large amounts of fat instool (steatorrhea). Stool are greasy, foul smelling,frothy, & excessive.Miss.kamlah20
As the changes in the villi continues, the absorptionof protein, carbohydrate calcium, iron, folate, &vitamin A,D,E. K & B12 become impaired.Symptoms occur after taking solid food containinggluten. The child exhibit chronic diarrhea, vomiting,irritability, malabsorption, abdominal pain, & failure tothrive.Symptoms improved after dietary interventions, &the villi retain to normal within 6 months. Vitaminsupplement may be needed until the child gain normalabsorption function.Miss.kamlah21
Nursing managementsSupport the parents in maintain diet free from glutenfor the child. Educate the parents that celiac disease needslifelong dietary restriction & should not bediscontinues when the child is symptoms free. Avoidance of food rich in gluten is important such as:Bread, cake, doughnuts, cookies, crackers, chocolatecandy, ice cream. Miss.kamlah22
1- Which of the following measures would be themost effective in helping the infant with cleft lip& palate to retain to oral feeding?A.B.C.D.Bubble the infant at frequent intervals.Feed the infant small amounts at one time.Place the end of the nipple far to the back of theinfant’s tongue.Maintain the infant in a lying position while feeding.Miss.kamlah23
2- When teaching the mother of an infant who hasundergone surgical repair of cleft lip how to carefor the stutre line, the nurse demonstrates howto remove formula & drainage, which of thesolutions would the nurse use?A.B.C.D.Mouth wash.Povedone-iodine solution.A mild antiseptic solution.Half strength hydrogen peroxide.Miss.kamlah24
3- On the second postoperative day after repair ofa cleft palate, which of the following would thenurse expect as most appropriate to use with atoddler?A.B.C.D.Cup.Straw.Rubber-tipped syringe.Large holed nipple.Miss.kamlah25
4- immediately of return to the nursing unit aftersurgical repair of a cleft palate, in which of thefollowing position would the nurse place the child?A.B.C.D.On the back with the head in a position of comfort.In low fowler’s position with the head turned to theside.Lying on the abdomen with the head turned to theside.In reverse trendelenburg with the head tiltedforward.Miss.kamlah26
5- which of the following nursing diagnosis would thenurse identify as a priority for the infant withtrachoesophegial fistula?A.B.C.D.Impaired parenting related to newborn’s illness.Risk for injury related to increased potential foraspiration.Ineffective breathing patterns related to a weakdiaphragm.Imbalanced nutrition: less than body requirements,related to poor sucking ability.Miss.kamlah27
6- which of the following would indicate that theinfant with trachoesophegial fistula needssuctioning?A.B.C.D.Brassy cough.Substernal retractions.Decreased activity level.Increased respiratory rate.Miss.kamlah28
7- When obtaining the nursing history from motherof an infant with suspected intussusception,which of the following questions would be mosthelpful?A.B.C.D.“ what do the stools lock like”.“ when was the last time your child urinate”“ is your child eating normally”“ has your child has any episodes of vomiting”Miss.kamlah29
8- which of the following assessments would be thepriority for an infant who has had surgery tocorrect an intussusception & is now at risk fordevelopment of a paralytic ileus postoperatively?A.B.C.D.Measurement of urine specific gravity.Auscultation of bowel sounds.Inspection of the first stool passed.Measurement of gastric output.Miss.kamlah30
9- during physical assessment of a 4 month oldinfant with Hirschsprung’s disease, the nursewould most likely note which of the following?A.B.C.D.Scaphiod-shaped abdomen.Weight less than expected for height & age.Cyanosis of the fingers & toes.Hyperactive deep tendon reflexes.Miss.kamlah31
10- when teaching the parents of an infant withHirschsprung’s disease who received temporarycolostomy about the types of foods that infantwill be able to eat. Which of the following wouldthe nurse recommends?A.B.C.D.High fiber diet.Low fat diet.High-residue diet.Regular diet.Miss.kamlah32
Miss.kamlah 4 Symptoms in newborn includes: excessive salivation & drooling, often accompanied with cyanosis, choking, & sneezing. During feeding, the infant returns fluid through the nose & mouth. Abdomen may become distended due to trapped air. Diagnosis is made by attempting to pass a 5 or 8 French nasogastric tube into the stomach, the