Transcription
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Dialectical Behavior Therapy: Its Role inTreating the Traumatized BrainJaye L. Neal, LCSWMartha Wetter, PhDJuly 22 – 23, 2019Agenda Conceptualization of BPD Validation Neurobiology of Trauma Skills Training Linehan’s BiosocialTheory DBT Techniques forAddiction DBT Modes and Functions Individual therapy Stages of Treatment Phone Coaching andConsult Group DialecticsDialectical Behavior Therapy (DBT) DBT is an empirically based treatment and has beenidentified as the treatment of choice for BPD by theAmerican Psychiatric Association It consists of four components Skills training Individual therapy Phone coaching Consult groupJaye Neal, LCSWMartha Wetter, PhD1
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Conceptualization of BPD in DBT Affective Dysregulation Emotional lability Problems with anger Interpersonal Dysregulation Chaotic relationships Fears of abandonment Self Dysregulation Identity disturbance/ lack of sense of self Sense of emptinessConceptualization of BPD in DBT, cont. Behavioral dysregulation Suicidal behavior, threats, self-harm Impulsive behaviors Cognitive dysregulation Dissociative responses Paranoid ideation (extreme interpersonal sensitivity)** drop the “m” word from your vocabulary **BPD and Childhood Trauma Many conceptualizations of BPD do not address thechronic childhood trauma that individuals with BPDoften experience (but cf. Linehan’s discussion in herbook on pg. 26) Many researchers (Schore,Van der Kolk,, Zanarini,) viewpsychological trauma as an antecedent to BPD Traumatic victimization by primary caregivers ishypothesized to be one of the key etiological factors inBPD (with genetics and constitutional factors as well)(Ball & Links, 2009; Laporte, Paris, Guttman, &Russell, 2011; Zanarini, 2000)Jaye Neal, LCSWMartha Wetter, PhD2
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19BPD, Trauma, and Complex-PTSD Prevalence of chronic relational trauma in BPD is wellestablished Early, severe, and chronic maltreatment and neglect OR Chronic invalidation of the child’s behaviors, thoughts andfeelings Many symptoms of Complex-PTSD (C-PTSD) overlap withBPD criteria One strong demonstration of this overlap is the frequentoccurrence of early abuse, trauma, and the presence ofdissociative symptoms in individuals with BPDComplex PTSDSix clusters of symptoms have been suggested for adiagnosis of C-PTSD:(1) Alterations in regulation of affect and impulses, includingproblems regulating emotions, persistent sadness, suicidalthoughts, explosive anger or covert anger(2) Alterations in attention or consciousness, including forgettingtraumatic events, reliving traumatic events or havingepisodes of dissociation(3) Alterations in self-perception, such as a sense of helplessness,shame, guilt, stigma, and a sense of completely differentfrom other human beings (cf. earlier client self-description)Complex PTSD(4) Alterations in relations with others, includingisolation, distrust, or a repeated search for arescuer(5) Somatization, including a focus on physicalsymptoms and a search for medical treatmentof bodily distress(6) Alterations in systems of meaning, which mayinclude a loss of sustaining faith or a sense ofhopelessness and despairJaye Neal, LCSWMartha Wetter, PhD3
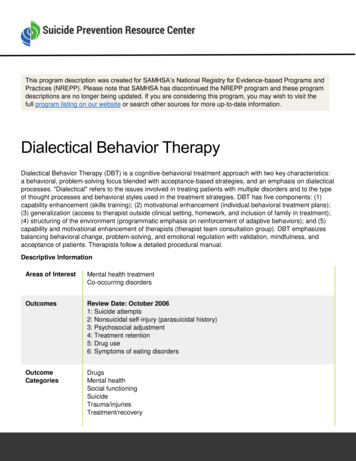
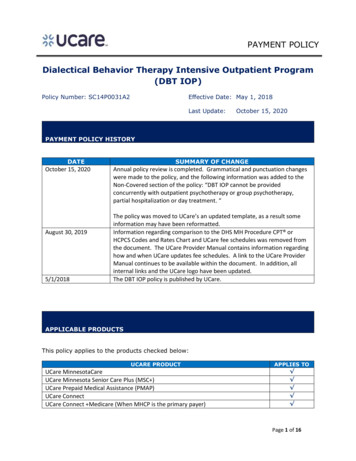
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Complex PTSD and BPD Even a cursory examination of these symptoms reveals aremarkable resemblance to the symptoms of BPD,indicating that BPD may well be best conceptualized asa form of PTSD due to chronic relational trauma startingin childhood. Since DSM-IV, a massive body of neurobiologicalresearch has accumulated revealing how chronicchildhood abuse and neglect can cause pervasive,devastating, and lasting biological and psychologicalharm.Importance of InterpersonalExperiences (i.e., Attachment Theory) Human connections build neural connections Incredible growth of synaptic connections occur aschild ages Wiring of the brain is governed by early experienceevery interaction counts! Thus, trauma in childhood changes braindevelopmentNeural circuitrynewborn3 month old15 month old2 year oldJaye Neal, LCSWMartha Wetter, PhD4
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Secure Attachment When parents are attuned to child’s inner states andrespond appropriately, a secure attachment is built Parent and child “resonate” with each other, so eachfeels “felt” The child actively needs and seeks attunement andattachment Prof. Ed Tronick’s Still Face Experiment shows whathappens when attunement does not occurStill FaceThe Other End of the AttachmentSpectrum: Neglect and Abuse Neurobiological impact oftrauma in childhood Before the connectionsbetween the amygdala andorbitofrontal cortex are built,the right amygdala becomeshypersensitive to stressfulconditions, holds mental modelsof expected danger, harborsterror and anguish, and lacksconnection with other circuitsfor regulationJaye Neal, LCSWMartha Wetter, PhD5
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Neglect and Abuse: Structural andFunctional Abnormalities Childhood maltreatment and neglect areassociated with structural and functionalabnormalities in different brain areas, including: the pre-frontal cortex (logic and reasoning) the corpus callosum (integrating the right and lefthemisphere) the amygdala (fear and facial recognition) the temporal lobe (hearing, verbal memory,language function) the hippocampus (memory)Neglect and Abuse: Effects onNeurotransmitters Norepinephrine is increased, producing anxiety,arousal and irritability Dopamine is increased, producing hypervigilance,paranoia, and perceptual distortions Serotonin is decreased, leading to irritability,depression, or aggression Endogenous opioids are not produced, leading to apredisposition to opiate-based substance abuseNeglect and Abuse: Effects on Health Repeated, hyperarousal of the neuroendocrine system,especially in early childhood, often leads to long-lastingphysical problems Fibromyalgia, irritable bowel syndrome, chronic pelvic pain(females), migraine headaches, psychogenic-seizures, "acid"stomach, back pain, and autoimmune illnesses such as MS orlupus or RA As a result, individuals with BPD often have a diagnosis ofsomatoform disorder and often are regarded by doctorsas difficult patients, because they don’t improve withtreatment (cf. Dr. Burke-Harris’ findings, coming up)Jaye Neal, LCSWMartha Wetter, PhD6
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Frequency of Childhood Trauma:Adverse Childhood Events Studies(ACEs)V. J. Felitti, MD & R. F. Anda, MDSurvey of over 17,421 adults in the KaiserPermanente HMO in California http://www.acestudy.org/ Nadine Burke-Harris, MDWhat are Adverse Childhood Events? Abuse: Neglect Emotional Emotional Physical Physical Sexual Household Dysfunction: Substance abuse Mental illness Mother treated violently Incarceration of householdmember Parental separation or divorceJaye Neal, LCSWMartha Wetter, PhD7
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Relation of ACEs to mental & physicalproblems(Am J Prev Med 1998;14: 245-258) Dose/ response relationship Almost two-thirds of study participants reported at least 1ACE, and more than 1 in 5 reported 3 or more ACEs For people who reported 1 ACE, the probability of exposureto any additional ACE was 65%-93% Persons with 4 ACEs had: 4-12x risk for alcoholism, drug abuse, depression, suicideattempt 2-4x risk smoking, poor self-rated health, 50 lifetimesexual partners and STDs Neuroplasticity Brain’s capacity to change neural connectivity in response tonew experiences Synaptogenesis formation of new synaptic connections Neurogenesis birth of new neurons These occur throughout the lifespan!Jaye Neal, LCSWMartha Wetter, PhD8
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Good news Findings from three areas of research psychotherapy, attachment, and neurobiologyshow that:Psychotherapy which works is based on arelationship in which the therapist uses attuned(validating) responses to encourage and shapebehavioral change (change strategies) whichwork because the brain is neuroplasticGood news In DBT, the combination of validation and changestrategies ultimately rebuilds neural networks in theclient’s brain that were harmed by adverse childhoodevents What makes DBT dialectical is the balance of validationstrategies with change strategies Thus, DBT is an extremely helpful approach to addressthe neuro-biological effects of traumaStudy: DBT Alters Emotion Regulationand Amygdala Activity Study conducted by Goodman, Carpenter, Tang et al, in2014 Previous findings: Deficient amygdala habituation hasemerged as a biological correlate of affective instability inBPD Hypothesis: BPD patients would exhibit decreased amygdalaactivation and improved habituation, as well as improvedemotion regulation, with standard 12-month DBT Results: Hypothesis was CONFIRMED decreased amygdalaactivation with DBT treatmentJaye Neal, LCSWMartha Wetter, PhD9
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Linehan’s Biosocial Theory of BPD BPD is a dysfunction in emotion regulation Genes and intra-uterine factors interactreciprocally with an invalidating environment toproduce vulnerability to pervasive emotiondysregulation The invalidating environment reflects aninsecure attachment in the caregiver-infantrelationshipBiosocial Theory of BPDBiologicaldysfunction in theemotion regulationsystemPervasive ve Emotion Dysregulation High Sensitivity Immediate reactions Low threshold for these reactions High Reactivity Extreme reactions High arousal which dysregulates cognitive processing Slow Return to Baseline Long lasting reactions High sensitivity to next emotional stimulusJaye Neal, LCSWMartha Wetter, PhD10
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Invalidating Environments In attachment-disordered, invalidating interactions, theinfant/child’s communications about her inner world: Are not accepted as accurate Are not seen as valid response to events Are dismissed, trivialized or disregarded Are directly criticized or punished Are attributed to socially unacceptable characteristics(e.g., laziness, over-reactivity, lack of motivation,manipulation, lack of discipline) Are pathologized even when normalConsequences of InvalidatingEnvironments The invalidating environment does not teach theinfant/child to: Trust her emotions and thoughts as valid responses toevents Identify and label emotions and thoughts in a normativeway Regulate emotions when they become intense oroverwhelmingConsequences of InvalidatingEnvironments The invalidating care-giver makes problem solving seemOVERLY SIMPLE By over-simplifying problem solving the invalidatingenvironment does not model for the child how to: Tolerate distress Form realistic goals and expectations Understand the (often slow) process of achieving goalsand expectationsJaye Neal, LCSWMartha Wetter, PhD11
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Consequences of InvalidatingEnvironments The child who experiences invalidation or mistreatment islikely to conclude that she must be unacceptable or bad todeserve such punishment or neglect The abused or neglected child also comes to view caretakersas dangerous, rejecting, or unavailable, and the world as adangerous place Current threats that resemble the early invalidatingrelationships trigger painful childhood memories. This canleads to behavior that, although intended to keep peopleattached, appears so child-like and demanding that it doesthe oppositeConsequencesof Invalidating Environments As stated by a trauma survivor, “if badrelationships messed me up, then it followsthat I need good relationships to help meheal.” For our purposes, good relationships intherapy represent relationships that arebased on an attached, attuned,validating therapist We will return to the topic of validationlater in this trainingWhat does DBT Consist of? Group skills training (different from group therapy) DBT-informed individual psychotherapy Telephone skills coaching calls with client in betweensessions Therapist consultation meetings with other DBT therapists Ancillary treatments other treatments not directlyconnected to DBT (pharmacotherapy, inpatienttreatment, AA, NA)Jaye Neal, LCSWMartha Wetter, PhD12
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19DBT Functions And Modes Of TherapyFunctionModeEnhance CapabilitiesSkills training; medicationImprove motivation*Individual therapyAssure generalization ofskillsPhone/email consultationKeep therapistdialectical/balancedConsultation meetingStructure the environmentConsult to environment(parents, partners, children,other treating professionals)*focusing on obstacles, distortedcognitions, and reinforcementcontingenciesDBT Assumptions for Clinicians Clients are doing the best they can Clients want to improve Clients need to do better, try harder, and be more motivatedto change Clients may not have caused all their own problems, but theyhave to solve them anyway New behavior has to be learned in all relevant contexts All behaviors (actions, thoughts, emotions) are caused Figuring out and changing the causes of behavior is a moreeffective way to create change than judging and blamingthe client (which may well happen with BPD; e.g., “she justdoesn’t want to change.”)DBT is a STRUCTURED Treatment withStages and Targets Pretreatment Targets Orientation and CommitmentOrientation Explain neurobiology of trauma to client Orient client to program Review Patient and Therapist Agreements* with client Agree on goals (Stage I behavioral targets)*Jaye Neal, LCSWMartha Wetter, PhD13
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19DBT is a STRUCTURED Treatment withStages and TargetsCommitment Pros and cons of commitment to change Devil’s advocate approach Foot-in-the-door approach; door-in-the-face approach Review of prior commitments Shaping; CheerleadingFoot in the DoorJaye Neal, LCSWMartha Wetter, PhD14
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Treatment Stages in DBT (FollowingCommitment) Stage I: “get out of hell;” focus on behavioral control, safety, and skillacquisition Stage II: Trauma work; narrating traumatic events; reduce PTSDsymptoms Stage III: Define life goals, build self-respect, achieve dialectical view ofoneself and the world (these may begin in Stages I and II)Stage I Treatment Target Hierarchy Three kinds of target behaviors toorder of importance)decrease(listed in Life-threatening behaviors Suicide attempts and life threatening behaviors (e.g., selfharm, dangerous drug use) Therapy-interfering behaviors Any behaviors that interfere with the client receivingeffective treatment (e.g., non-attending behaviors, noncollaborative behaviors, non-compliant behaviors)Stage I Treatment Target Hierarchy Quality-of-life-interfering behaviors Substance abuse Extreme financial difficulties Criminal behavior that may lead to jail High risk sexual behavior Other very dysfunctional behaviors: Interpersonal (biting someone during a fight) Employment-Related (telling your boss to “f—k off”) School-Related (e.g., getting suspended/expelled) Illness-Related (e.g., refusal to treat physical illness or constant treatmentseeking) Mental Health-Related (e.g., going into hospitals, psychiatrist-hopping,not taking meds as prescribed)Jaye Neal, LCSWMartha Wetter, PhD15
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Stage I Treatment Targets Behavioral skills to increase: Attending skills training group Meets once a week, usually for 2-2.5 hours, for 14 months Organized like a class and has 4 skills modules Core mindfulness Distress Tolerance Emotion Regulation Interpersonal EffectivenessThe Four Skills Modules of Stage IMindfulness, attentional awareness and control Learn to observe and describe sensory experiences, from bothinternal and external sources Learn to increase awareness of the present moment Learn to participate fully in the present moment Engage the world in a nonjudgmental wayInterpersonal effectiveness Learn to ask for what you need effectively Learn to say no to unwanted requests effectively Learn to do both in a manner that maintains self-respect and/orthe relationshipThe Four Skills Modules of Stage IEmotion Regulation Learn the model for describing emotions Learn to decrease vulnerability to negative emotions Learn to increase occurrence of pleasant emotions Learn techniques to manage extreme emotionsDistress Tolerance Learn to tolerate distress and accept reality instead ofusing impulsive behaviors to relieve miseryJaye Neal, LCSWMartha Wetter, PhD16
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Targets in Stage II and Stage III Stage II Targets Emotionally process the past (i.e. trauma work) Decrease post-traumatic stress This requires the client to be able to experience intenseemotion without avoidance, learned through skills training Stage III Targets Manage normal problems in living Increase self-validation Move toward individual goalsWhat Exactly Does Dialectical Mean? A dialectic is a method of examining and discussing opposingideas in order to find a balanced and accurate view Looking for a synthesis of the thesis and antithesis Example: Thesis: All people are capable of evil Antithesis: All people are capable of good Dialectical Synthesis: (1) Some people are capable of good,and some are capable of evil; (2) Most people are capable ofboth good and evil at times, depending on circumstances, etc. A dialectical view leads to a balancing of extremesA quick way to view a dialecticJaye Neal, LCSWMartha Wetter, PhD17
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Dialectical Conflicts ClientsExperience Clients frequently vacillate between sympatheticarousal and parasympathetic numbing (which is whythey are so often diagnosed with Bipolar I Disorder) This pattern reflects what may be called the PTSD rollercoasterDialectical Conflicts ClientsExperience Clients frequently vacillate between rigidly held butcontradictory points of view It’s all my fault – It’s all their fault Clients tend to see reality in polarized categories of“either-or” rather than “both-and” which produces ablack/white view of their world and its possibilities Such categorical thinking is often accompanied by thebelief that things once defined never change, so oncea person has failed, she will be a failure foreverJaye Neal, LCSWMartha Wetter, PhD18
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19DIALECTICS: How Does This Help? This perspective helps pave the way toward finding themiddle path by allowing the client to: Expand thoughts and ways of considering life situations "Unstick" standoffs and conflicts Be more flexible and approachable Avoid assumptions and blaming self and others The middle path requires acceptance of reality as it is.This requires the balancing (synthesis) of opposites: Accepting self and others, AND also acknowledging theneed for change Balancing self-blame with blaming othersDialectical Issues That Must BeBalanced By Client And Therapist Skill Enhancement vs. Self-Acceptance Problem-Solving vs. Problem Acceptance Affect Regulation vs. Affect Tolerance Self-Efficacy vs. Help-Seeking Trust vs. Suspicion Contemplation/meditation vs. ActionDialectics in DBT The dialectic of acceptance vs. change runsthroughout DBT in terms of treatment, appearing asthe tension between validation strategies andchange strategies Example of dialectics in DBT: You are doing the best you can, and you need to dobetter, try harder, and be more motivated to change. You are responsible for your own actions and you arenot in control of everything.Jaye Neal, LCSWMartha Wetter, PhD19
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Validation Is acknowledgement and acceptance of client as she is Communicates to the client that you realize she is doingthe best she can in the moment Balances the message she needs to change, to workharder, to act “better” Helps client feel safe Builds a solid therapeutic relationshipValidation checklists provided in your materialsTargets for Validation: Things to watchfor in the therapy room Emotional experiences,pain, suffering Cognitive experiences,thoughts, beliefs,assumptions Behaviors Inner strength, potentialto succeedLevels of validation1.2.Stay awakeMake accurate reflections Repeat what client said Rephrase using synonyms3.Identify un-verbalized emotions, thoughts, behavioral urges Paraphrase using inferred meaning Reflect the emotion behind the content4.Validate in terms of past learning or biological dysfunction “It makes sense you feel that way because in the past . . .”5.Validate in terms of present context or normative functioning “Of course you feel that way given what just happened ”6.Be radically genuineJaye Neal, LCSWMartha Wetter, PhD20
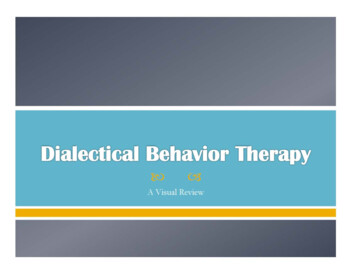
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Validating vs. Invalidating Responses: Impact onPsycho-physiological Arousal and alidationValidation1615141312012Time Period34Shenk & Fruzzetti, 2007Validation – Or Not Therapists may fail to validate an emotion, thought, oraction ( a missed opportunity), which is different fromacting invalidating toward the client Or, they may block inaccurate or distorted expressionsof a feeling or thought (e.g. “I’m worthless” or “Things willNEVER change”) and then redirect to a more accurateexpression (e.g. “Of course you think that AND it is notso”)Validation Rules Believe and reflect that the client is capable and thather perspective is understood and important and valid inher own context Rule: Do at least one level 5 validation each session (i.e.,communicate to the client that you can see there is noother way she could have felt, or thought, or acted giventhe current circumstances)Jaye Neal, LCSWMartha Wetter, PhD21
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Validation Rules: You Cannot Do theFollowing Too Much Communicate Interest: “Tell me more about that ” “How did that happen?” Body language – lean toward the client, make eye contact, nod Hear and see correctly: “It sounds like you were really upset ” “You look like you might be scared.” Communicate understanding “It makes sense that you did that or felt that or thought that.”Validation Rules: You Cannot Do theFollowing Too Much Give causes “Of course you feel this way, you have a sensitive nervoussystem.” “Naturally you believe that, you’ve been hurt in the past.” Be nonjudgmental Have an accepting facial expression, that means nofrowns, no pursed lips, no tsking. This means no disapprovaleven though you may be disappointed or dismayed bywhat the client is telling youValidation Rules: You Cannot Do theFollowing Too Much Accentuate the correct or effective i.e., find the thing you can be positive about “Even though it didn’t work out for you the way youwanted, you tried really hard.” “Although you were really angry and you shouted, youdidn’t hit anybody.” Give functional validation (through behavioral response) The statement “I’m thirsty” is met with a drinkJaye Neal, LCSWMartha Wetter, PhD22
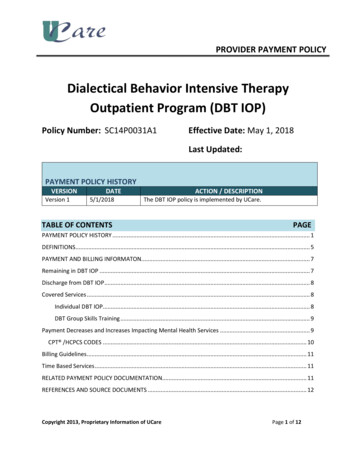
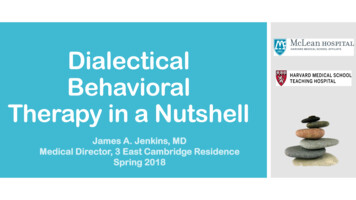
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Validation Rules: You Cannot Do theFollowing Too Much Treat the client as though she can be strong Don’t walk on egg shells because actually that is patronizing,and communicates you believe she is weak, dangerous, crazy,or all three Cheerlead Encourage and support your client Be genuine Treat the client as a person you are collaborating with to solveproblems they naturally are having given their past experiencesand current situationValidation & HopeToxic Positivity This is hard. You've done hard thingsbefore and I believe in you. You'll get over it! I know there's a lot that could gowrong. What could go right? Just be positive! All vibes are welcome here. Good vibes only! It's pretty normal to have somenegativity in this situation. Stop being so negative! It's probably pretty hard to be positiveright now. I'm putting out good energyinto the world for you. Think happy thoughts! Sometimes giving up is ok. What is yourideal outcome? Never give up! It's never fun to feel like that. Is theresomething we can do today thatyou'd enjoy? Just be happy! It's probably really hard to see anygood in this situation. We'll make senseof it all later See the good in everything.It’s Not about the NailJaye Neal, LCSWMartha Wetter, PhD23
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19When in doubt, validate!!Balancing Communication: As Always,a Dialectic Exists There are two primary communication styles in DBT They not only balance each other, but they must bothbe used often. The therapist must learn to move backand forth between the two quickly and easily Reciprocal communication: Responsive, warm, genuine,and appropriately self-disclosing Irreverent Communication: Off-beat, unexpected, and/ortongue-in-cheekCommunication Strategieschecklists providedIrreverent Communication Irreverent communication is used to: Get the client’s attention Shift the client’s affective response Get the client to see a completely different point of view It is used whenever the client, or both therapist andclient, are “stuck” in an ineffective emotional, thought,or behavior pattern.Jaye Neal, LCSWMartha Wetter, PhD24
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Change Strategies: Skills Training Validation is one side of the dialectic in DBT We will now turn to the other side of the dialectic:Problem solving/ change techniques used in DBT These techniques are taught in the DBT skills traininggroups Core mindfulness Distress Tolerance Emotion Regulation Interpersonal EffectivenessCore Mindfulness Mindfulness skills are central to DBT; these skills underpinand support all other DBT skills Core Mindfulness skills are the only skills that arehighlighted the entire year They are both taught in a 7-week unit and reviewedfor two sessions at the beginning of each of the otherthree skills units The focus of Core Mindfulness skills is learning to be incontrol of one’s attentionJaye Neal, LCSWMartha Wetter, PhD25
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Core Mindfulness It is the act of consciously focusing the mind in thepresent moment without judging the moment as goodor bad When mindful, we are aware in and of the presentmoment. We are alert and awake, like a security guardat a school But we are NOT rigidly clinging to the present moment(as if we could keep a present moment from changing ifwe cling hard enough)Mindfulness practice can literallychange your brain!Jaye Neal, LCSWMartha Wetter, PhD26
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Mindfulness Research Holzel, Carmody, Vangel et al. (2011) conducted acontrolled longitudinal study to investigate pre–postchanges in brain gray matter attributable toparticipation in a mindfulness program The results indicated that participation in mindfulness isassociated with an increase in the amount of graymatter in brain regions involved in learning and memory,emotion regulation, self-reflective processing, andperspective-takingCore MindfulnessThe Mindfulness Skills include: What skills (what you do) Observe Describe Participate in the present moment How skills (how you do the What skills) Nonjudgmentally One-mindfully (with focus) Effectively (that is, willingly and as skillfully as possible)Core Mindfulness DBT teaches there are three states of mind that humans maybe in: Emotion Mind Reasonable Mind Wise Mind Wise Mind is the state of mind in which both the right brainand the left brain work together; it is seeing the value of bothreason and emotion; it is finding the middle path betweenthese two states of mind Wise mind is needed to make skillful, balanced decisions and isdeveloped through mindfulness practiceJaye Neal, LCSWMartha Wetter, PhD27
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Core Mindfulness: The Takeaway Intentionally focusing on the present moment, without judgingit or denying it or holding onto it, and bringing your focusback when it wanders, again and again and again, is all thatis needed to practice mindfulness and reap its benefits. MINDFULNESS CAN BE PRACTICED ANYTIME, ANYWHERE, ANDWHILE DOING ANYTHING if you are focused in the presentJaye Neal, LCSWMartha Wetter, PhD28
Dialectical Behavior Therapy:Its Role in Treating the TraumatizedBrain07/22/19 – 07/23/19Interpersonal Effectiveness Interpersonal Effectiveness is the next module in skills training,running approximately eight weeks It is designed to teach clients how to ha
Dialectical Behavior Therapy: Its Role in Treating the Traumatized Brain 07/22/19 –07/23/19 Jaye Neal, LCSW Martha Wetter, PhD 1 Dialectical Behavior Therapy: Its Role in Treating the Traumatized Brain Jaye L. Neal, LCSW Martha Wetter, PhD July 22 – 23, 2019 Agenda Conceptualization