Transcription
Standard Operating Procedure forthe Dental Management ofNon-COVID-19 Patients in Wales1Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
All Wales Clinical Dental Leads COVID-19 Group – Reports to CDO WelshGovernmentDr Warren TolleyDeputy Chief Dental Officer and Dental Director Powys Teaching HealthBoardDr Ilona JohnsonReader and Hon Consultant in Dental Public Health Cardiff UniversityDr Vicki JonesClinical Director of Community Dental Services Consultant in SpecialCare Dentistry Aneurin Bevan University Health BoardDr Mick AllenConsultant in Special Care Dentistry Aneurin Bevan University HealthBoard. Clinical Director for Community Dental Services Cardiff and ValeUHBMr Karl BishopDental Director and Consultant in Restorative Dentistry Swansea BayUniversity Health BoardProfessor Ivor ChestnuttProfessor and Honorary Consultant, Dental Public Health, ClinicalDirector University Dental Hospital Cardiff and Vale University HealthBoardDr Catherine NelsonAssociate Medical Director for Dental Hywel Dda Health BoardDr Robert DaviesDental Foundation Training Program Director Health Education andImprovement Wales (HEIW) and Primary dental care COVID lead CwmTaf Morgannwg University Local Health BoardDr Sandra SandhamClinical Director for North Wales Community Dental Service andDirector of Dental Public Health Betsi Cadwaladr University HealthBoardDr Nigel MonaghanConsultant in Dental Public Health Public Health Wales and VisitingProfessor in Public Health, University of South WalesAdvice to the Group is provided when required by Dr Melanie Wilson, Lead and Senior Lecturer in OralMicrobiology, Health & Safety, Cardiff University School of Dentistry.The Group is independent of Welsh Government but provides reports and recommendations directly tothe Chief Dental Officer for Wales.2Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
Executive SummaryThis guidance is applicable to Wales. The document brings together the information from previous StandardOperating Procedures and key changes are highlighted in the text. It is intended for dental care settings thatprovide care involving patients who are COVID-19 (C-19) negative or who are not suspected of being C-19positive. Separate SOPs are available at centres for people with suspected/ confirmed C-19. Furtherdocuments have been developed in conjunction with National Groups/ Managed Clinical Networks forspecific areas of service provision e.g. paediatrics, orthodontics, and domiciliary care. Primary care providersin other UK nations should refer to guidance produced by their own administrative bodies and regulators.BackgroundThe onset of symptoms after exposure (incubation time) to C-19 is currently estimated at between oneand fourteen days.1 Patients may be infectious for one to two days before the onset of symptoms, theymay be most infectious when they are symptomatic and it is estimated that they may be infectious for upto two weeks.Cases can deteriorate rapidly, often during the second week of disease, and this can lead to death.1 Asthis is a novel virus there is no immunity in the population and current estimates indicate that C-19 hascaused infection for between 5 and 10% of the UK population with the rest remaining susceptible toinfection. For most patients the symptoms are mild and manymay be asymptomatic.C-19 symptoms can vary in severityRecent reports indicate that C-19 transmission is primarilybetween people through respiratory droplets and contactroutes, this includes fomites on surfaces.2 The amount ofviable virus in aerosol has not yet been confirmed and theamount of virus exposure which can result in infection is alsounclear at this time. At present, the World HealthOrganisation (WHO) recommend airborne precautions forAGPs in conjunction with undertaking risk assessments. TheWHO also recommends frequent hand hygiene, respiratoryetiquette, and environmental cleaning and disinfection.3from no symptoms, to having fever 37.8 C, flu like symptoms,persistent cough (with or withoutsputum), anosmia (loss of the senseof smell), ageusia (the loss of thesense of taste), hoarseness, nasaldischarge or congestion, shortnessof breath, sore throat, wheezing,sneezing, general fatigue, muscularpain and GI symptoms. Severe casescan develop pneumonia, acuterespiratory distress syndrome,sepsis and septic shock.1The Welsh Government strategic approach since March 2020has been to reduce community transmission through socialdistancing, protecting the most vulnerable and pausing allnon-essential services at the peak of the pandemic. Services are being restored in this recovery phase.This has been supported by the introduction of a Test, Trace, Protect strategy for identification, isolationand containment (in Wales) on the 1st of June 2020.4 The aim is to restore the delivery of routine care todental patients whilst taking the necessary measures to ensure patient safety. Patient advice andinformation is provided by NHS Direct Wales (online) and NHS 111 Wales (telephone).European Centre for Disease Prevention and Control: Q and A on COVID-19 nswersModes of transmission of virus causing COVID-19: implications for IPC precaution recommendations (29 March 2Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations: for-ipc-precaution-recommendations4 Test Trace Protect: Our strategy for testing the general public and tracing the spread of coronavirus in Wales. https://gov.wales/test-traceprotect-html33Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
Table of ContentsEXECUTIVE SUMMARY . 3BACKGROUND . 3CHANGES SINCE PREVIOUS RELEASES . 5KEY CHANGES FROM PREVIOUS SOPS. . 5DE-ESCALATION IN WALES . 7RELEVANT GUIDANCE . 8UPDATES AND INFORMATION . 8REMOTE ASSESSMENT RESOURCES . 8CONDITIONS WHICH REQUIRE URGENT MEDICAL/DENTAL ATTENTION TO SAVE LIFE . 9ADVICE ON SELF-CARE . 9REMOTE PRESCRIBING. 9PRIORITISING CARE . 10C-19 AND URGENT DENTAL CONDITIONS WHICH NEED FACE TO FACE ASSESSMENT, DIAGNOSIS OR TREATMENT . 10PROVISION OF CARE DURING THE RECOVERY PHASE . 11SCHEDULING APPOINTMENTS . 12RECORD KEEPING . 13PREPARING STAFF . 13PREPARING THE PRACTICE ENVIRONMENT . 13PROCEDURES FOR PATIENTS REQUIRING NON-AGP . 14NON-AGP TREATMENT PROTOCOLS . 16ADDITIONAL PROCEDURES FOR PATIENTS REQUIRING AGP* . 17AGP TREATMENT PROTOCOLS. 18DOFFING PPE . 19DECONTAMINATION . 20ACTIONS IN THE EVENT OF A PATIENT BEING IDENTIFIED WITH C-19 IN THE SURGERY. 21MEDICAL EMERGENCIES . 22APPENDIX 1: PRESCRIBING REMOTELY. 23APPENDIX 2: ASSESSMENT FOR C-19 AND MEDICAL HISTORY . 24APPENDIX 4: STAFF RISK ASSESSMENT, TRAINING, WELLBEING AND INSTRUCTIONS CHECKLISTS . 29STAFF ILLNESS AND WELLBEING CHECKLIST . 30UNIFORM INSTRUCTIONS FOR STAFF. 30APPENDIX 5: AREAS AND ZONING AND PERSONAL PROTECTIVE EQUIPMENT . 31COUNTERFEIT PPE PRODUCTS AND CHECKS THAT PPE IS FIT FOR PURPOSE BEFORE USE . 31APPENDIX 6: PREPARING WAITING AND COMMUNAL AREAS . 32CHECKLIST TO MINIMISE THE RISK OF TRANSMISSION. 32APPENDIX 7: PREPARING SURGERIES . 33APPENDIX 8: VISIT INFORMATION CHECKLIST . 34APPENDIX 10: HAND HYGIENE. 36APPENDIX 10: C-19 CLINICAL DENTAL RISK ASSESSMENT CONSIDERATIONS . 38RISK REDUCTION AND AEROSOL GENERATION IN DENTISTRY . 40APPENDIX 11: MEDICAL EMERGENCY PROCEDURE FOR WHEN AN AGP HAS COMMENCED . 43APPENDIX 12: CARE PATHWAY . 454Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
Changes since previous releasesThis document should be considered as a live document and will be updated as new information andevidence becomes available.Key changes from previous SOPsThe key changes included in this document have been highlighted within the text. This document bringstogether the information from previous Standard Operating Procedures.Information about providers for AGP care has been updated to reflect current shielding arrangements.The definition of low risk patients, for whom standard infection control measures (and no clearancetimes are needed) has been updated to reflect the latest infection control guidance.5The position in relation to the need for settle time for non–AGP procedures has been clarified followingrecent publications.No settle time is required for most non-AGP procedures. ForTime for settle and clearancenon-AGP procedures that have produced a significant about offollowing AGPs has been updated tosplatter/ droplets (for example a difficult extraction) it isreflect current transmission-basedrecommended that there should be a minimum of 10 minutesprecaution advice6, the recent SBARbetween the end of the procedure (e.g. the tooth beingVentilation, Water andremoved) and the next patient entering the room to allowEnvironmental Cleaning in Dentallarger droplets to settle and enable effective cleaning.Surgeries Relating to COVID-197 andHTM-03-01.8For rooms with known air changes, where mitigating measures are used, this document refers to thetables (examples provided in table 1 and 2 below) that are provided in the SBAR document.7 For AGPs ina room with the recommended number of air changes ( 10ACPH) as outlined in HTM-03-017,8 aminimum of 16 minutes is considered appropriate for short AGP treatments ( 10 min) where highvolume (HV) suction is used, extending to 18 minutes for AGP treatments of 40minutes.Where other mitigating factors are also used e.g. rubber dam, fallow times cannot be below 10 minutes.A minimum of 10 minutes must remain for larger droplets to settle prior to surgery decontamination andbefore the next patient enters the room irrespective of the calculated fallow time and any mitigation.Clarification has been given to indicate that the end of AGP is the completion of the AGP component ansmission-based-precautionstbps/7 2020/08/Ventillation-Final-Copy-1.pdf8 es-parts-a-and-b565Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
Table 1 Post AGP settle and clearance time for surgeries (in minutes) according to the duration ofprocedure when no mitigation is used (i.e. no HV suction) and the number of air changes per hour in theroom (table from SBAR Ventilation, Water and Environmental Cleaning in Dental Surgeries Relating toCOVID-19)Room Air change rate (ACPH)(with post AGP times for procedures times in min below)Duration ofAGP 77604935272240368176112816350362722Table 2 Post AGP settle and clearance time for surgeries (in minutes) according to the duration ofprocedure and the number of air changes per hour in the room with rubber dam and high-volumesuction* mitigation (table from SBAR Ventilation, Water and Environmental Cleaning in Dental SurgeriesRelating to COVID-19)Room Air change rate (ACPH)(with post AGP times for procedures times in min below)Duration ofAGP 527211410*10*4019991563929221510*10**Please note that not all units can provide high volume suctionThis document also provides an update on the use of local recirculating air cleaning devices (with HEPAfiltration and UVC) to improve air quality. Instructions for practices who wish to use this equipment andthe need to verify measurements (flow rates) and ACPH is also included. In addition, the use of optimalmaintenance regimes, calculations from the ventilation SBAR5 and maintenance of records of allinformation relating to decisions about times for possible future reference is included.Fallow times for AGPs may be omitted if the next patient is a member of the same household in closecontact and is not in an at-risk group. A fallow time must be in place following the care of the householdgroup.Advice has now been included on the very brief, gentle use of the 3 in 1. If used in this way, with highvolume suction mitigation, with a low risk patient in a low risk geographic area, this would be a low riskprocedure and no additional fallow time should be needed.Advice to maintain social distancing (2m) and wearing of masks in all communal areas where this is notpossible is also emphasised in the main text.Personal protective guidance has been updated to reflect the latest Infection Control Guidance, whichnow omits shoe covers and hats. These are now optional.6Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
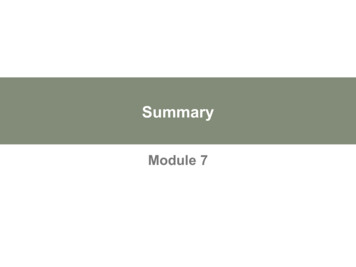
De-escalation in WalesDe-escalation of the C-19 response covers the phase when community transmission is decreasing.9AimThe aim will be to implement a phased, risk-based re-establishment of dental services to meet populationneeds.ObjectivesPrioritise dental care for at-risk groups and people with symptoms/ urgent routine dental problems.Increase practice-based dental care to meet the population’s oral health needs.Maintain emergency/ urgent dental care provision (COVID and non-COVID) to meet requirements.Re introduction of routine dental care and dental prevention activities based on riskThis approach will be based on risk assessment, to minimise the possibility of transmission of C-19 topatients and the dental team within the dental care setting or during dental care procedures.De-escalation principlesCapacity for dental care is limited by measures toreduce transmission risk particularly in the earlystages of de-escalation. However, given the currentlower community transmission in Wales we are nowmoving into low amber. The approach aims todeliver dental services in a way that prioritises carefor those most in need and at risk of seriouscomplications or significant deterioration. Servicesprovided can now increase as C-19 risk reduces.Routine assessment can resume if there is capacityto do so, again by focussing on those who arevulnerable or at risk first. This SOP supports thesafe delivery of AGP care and a stepwise increase incare to meet patient needs based on risk.The Urgent/ Emergency Designated Dental Centreswill continue to provide urgent and emergencydental care for patients with C-19 during the greenphase of de-escalation until the point where this isno longer necessary.9De-Escalation Alert Levels and Dental ServicesRedUrgent/ emergency dentalservices onlyServices to address dentalproblems and symptomsHigh AmberServices to treat dentalconditions with minor/ noLow AmbersymptomsGreenAll routine dental careOfficial communications from the Welsh Government AWDPH pages: -19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
Relevant GuidanceThis document should be considered alongside current advice, guidance and guidelines for dental care: COVID dental de-escalation plans 10COVID-10 infection prevention and control (IPC)11,12COVID-19 personal protective equipment (PPE)13Advice on PPE guidance implementation COVID-19: infection prevention and control (IPC)14Advice on aerosol generating procedures 15should be read alongside guidance for standard andtransmission based precautions.14 The situation is constantly changing and documents are being updatedas new evidence becomes available. As such, it is important to continue to access information regularly,from recognised and reliable sources.Updates and informationDental teams are advised to keep up to date, regularly reviewing information and the latest updates: Information for Health and Social Care Professionals – Wales (including PPE);Coronavirus (COVID-19): latest information and advice;PHW COVID-19 interim guidance for primary care.Remote assessment resourcesPatients should be assessed by a dentist by telephone or video, where appropriate, gathering enoughinformation to identify whether the individual has: A serious condition requiring urgent medical/dental attention to save life;A condition which could be self-managed with appropriate advice and possible prescription;An urgent dental condition which needs face-to-face assessment, diagnosis or treatment.It is recommended that assessments are used in advance of the appointment to reduce appointmenttimes in practice. The video consultation platform Attend Anywhere is currently being made available tosupport practices in this role.16A number of resources have been developed to support the management of dental cases, and dentalcare in the recovery phase of the pandemic. Management of Acute Dental Problems During COVID-19 Pandemic17British Endodontic Society: COVID-1918COVID19 BOS Advice1910 Official communications from the Welsh Government AWDPH pages: https://awfdcp.ac.uk/covid-19/official-comms11 2 ction-prevention-and-control/nipcm/13 rus-covid-19-personal-protective-equipment-ppe14 entation/15 nerating-procedures16 https://digitalhealth.wales/tec-cymru/vc-service17 ental-problems-covid-19/18 https://britishendodonticsociety.org.uk/19 BOS-Advice8Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
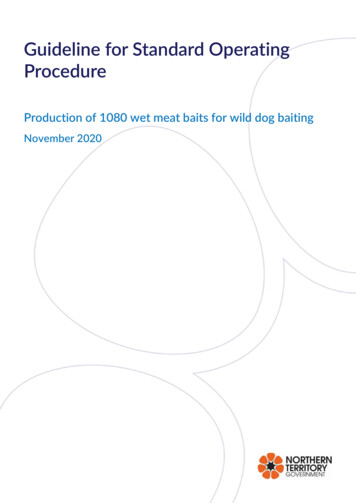
Conditions which require urgent medical/dental attention to save lifePatients with suspected life-threatening conditions should be immediately referred to the appropriateemergency medical services.Advice on self-careSome cases will only require advice to enable the patient to self-care. NHS 111 Wales Encyclopedia20 has31 pages on dental topics. Evidence-based principles of prevention should be used for all patients.21Remote prescribingDentists may prescribe pain relief and/ or antimicrobials in situations where it is clinically appropriate,following an assessment (including medical history and virtual assessment). A face-to-face consultationshould be undertaken where possible. Drugs for the Management of Dental Problems During COVID-19 Pandemic;22Primary Care Dental Services COVID-19 Toolkit: Appendices 2 and 4;23FGDP COVID-19: latest guidance and resources for GDPs;24High level principles for good practice in remote consultations and prescribing.25Advice must be given to the patient so that theyknow what to do if their condition starts todeteriorate and to call Dental Helpline, 111 or999 should airway problems develop. They mustbe reminded of their need to declare their C-19status to the ambulance service/A&E staff.Risk AssessmentA C-19 and medical history should be taken inadvance of care (Appendix 2) and this should beundertaken remotely. Where this is available theoption of testing for C-19 to confirm statusshould be considered. New infection controlguidance now categorises risk.26 Most dentalpatients currently will be in a medium or highrisk category for treatment.Patients who are categorised as low risk for C-19(in accordance with the infection controlclassification)28 may be treated with standardinfection control precautions (SICPS)27 and nofallow time.LOW RISK for C-19Triaged/clinically assessed individuals with:no symptomsORno known recent COVID-19 contact whohave isolated/shieldedANDHave a negative SARS-CoV-2 (COVID-19) testwithin 72 hours of treatment and, for plannedtreatment and have self-isolated from the testdateORHave recovered from COVID-19 and have had atleast 3 consecutive days without fever orrespiratory symptoms and a negative COVID-19testORAre regularly tested (remain negative) e.g. somecare facilities and prisons20 https://111.wales.nhs.uk/encyclopaedia/21 Delivering better oral health: an evidence-based toolkit for k/government/uploads/system/uploads/attachment data/file/605266/Delivering better oral health.pdf22 4/SDCEP-MADP-COVID-19-drug-supplement-080420.pdf23 -dental-services-toolkit/24 20advice25 ions-and-prescribing.pdf26 t/uploads/system/uploads/attachment data/file/910885/COVID19 Infection prevention and control guidance FINAL PDF 20082020.pdf27 icpsall-pathways9Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
Prioritising CareUrgent/ emergency conditions should be prioritised. Those with the most urgent care need should beseen ahead of low risk routine cases. Routine cases should be seen wherever there is capacity to do so.Figure 1: Examples of severe urgent/ emergency dental conditionsSituations where leaving the dental condition without a clinical intervention may endanger the health ofthe patient/ would be likely to result in admission to hospital e.g.:oooDiffuse swelling / lymphadenopathy without a discharging sinusSuspected cancerBleeding that cannot be controlled with local measuresCases that have not responded to local management following local advice, antibiotics and appropriateanalgesia e.g.:oooSevere pain that has not responded to painkillers after 48 hrs of useSevere pain or diffuse swelling that has not responded to antibiotics after 72 hours of useA recent injury in a vital tooth which has resulted in pulpal involvement or trauma that hasresulted in a deranged occlusion.Practices should continue to work to support patients with dental care problems, managing patientexpectations and minimising the burden of dental problems on other health care services (e.g. working toprevent unnecessary patients attending at general medical practices, other NHS teams and helplines).C-19 and urgent dental conditions which need face to face assessment,diagnosis or treatmentPatients should be assessed for signs and symptoms of C-19 at the stage of telephone consultation usingthe latest criteria.28Cases/suspected cases would include one or more of the following in the previous 14 days: Confirmed C-19 (tested positive);Symptoms consistent with C-19 i.e. new continuous dry cough and/ or high temperature 37.8 C, arecent loss of smell or taste (sore throat, shortness of breath, difficulty breathing, nasal dischargeand GI symptoms are also possible symptoms);Contact with a confirmed case (tested positive).Where an individual has been told to self-isolate as part of TTP or travelClinicians should also be aware of the possibility of other symptoms particularly in patients who areimmunocompromised (including severe sore throat, loss of sense of taste).2928 COVID-19: investigation and initial clinical management of possible cases: cases29 -testing/symptoms.html10Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
Provision of care during the recovery phasePatient statusDental conditionDental Care ProviderSuspected or confirmed C19 (high risk C-19)Routine/ non-urgentTreatment should be deferred for 14 days aftersymptoms have stopped/ until confirmednegative.Urgent/ emergencyU/EDDC for C-19non-AGP/ AGPNo history/symptoms ofC-19All carePrimary Care Dental PracticePatients who areshielding4 or who have ahigher risk ofcomplications from C-1930All carePeople with no history/symptoms of C-19 (lowrisk C-19) can be seen in Primary Care DentalPractice. People with suspected or confirmed C19 (high risk C-19) should follow the urgent/non-urgent pathway as required.Patients who requiredomiciliary careAll careProcedures of domiciliary care services shouldfollow Health Board Domiciliary SOPs and it isrecommended that those providing regulardental domiciliary are tested regularly for C-19(e.g. every fortnight)Examples of high-risk individuals include: Older people, People who are shielding or who have health conditions which put them at risk,Pregnant women, People living in institutions e.g. residential care and prisons.3011Non-C-19 Version 1.01 Final 26.8.2020 (this replaces the previous non-AGP and AGP SOPs published by WG)
Scheduling AppointmentsAppointments should be arranged in advance.Patients must be spaced throughout the day to leave time for cleaning and to limit waiting /contacttimes. A recommended scheduling process is described in the table below:PatientRecommendationsShielding/ invulnerable groupsIf appropriate to be seen in primary care with an appointment at the beginning ofthe day. Ensure social distancing and recommended decontamination processes31before and after care to minimise risk.AGPsSpace appointments to ensure social distancing.Book at the end of a sessionSchedule time for procedure and time for decontamination (to include air clearancein an appropriate room)Non-AGPsSpace appointments to ensure social distancing. Schedule appoin
Care Dentistry Aneurin Bevan University Health Board Dr Mick Allen Consultant in Special Care Dentistry Aneurin Bevan University Health Board. Clinical Director for Community Dental Services Cardiff and Vale UHB Mr Karl Bishop Dental Director and Consultant in Restorative