Transcription
SPLINTING GUIDE FOR EMS/HOSPITAL PROVIDERSINTRODUCTION (LOUIS SPINA M.D., 9/2016)Splints can be applied to most pediatric fractures, dislocations and sprains. Splints mayalso aid in the immobilization of soft tissue injuries such as fingertip amputations andlacerations over joints where it is important to minimize tension or damage to thehealing injury.Immobilization can decrease pain and bleeding as well as prevent further vascular,nerve and soft tissue damage. Unlike casts, which are circumferential, splints allow forswelling in the immediate post injury phase and can reduce the possibility ofcompartment syndrome. They can be used the primary modality for immobilizationduring the healing phase of an injury and can be used temporarily until swellingresolved and a cast can be placed definitively.Many recent studies in the pediatrics have demonstrated that removable splints forminor injuries such as torus fractures provide a faster return to baseline function whencompared to traditional casting.Temporary splints from transport can be used by emergency medical services. Splintscan be made from a variety of materials. The most common form is plaster of Paris(powdered for gypsum impregnated in gauze. This has the benefit of being inexpensiveand customized to the patient. Plaster typically sets in 2-8 minutes but does not reachmaximum strength until 24 hours. Malleable aluminum, air and synthetic splintingmaterials may also be used (e.g. Fiber glass, Orthoglass). Synthetic splinting materialsare more difficult to mold and more expensive. However, they are lighter, set morequickly and are water resistant.Preformed splints for common uses are more readily available (e.g. thumb spica). Therepreformed splints come in a variety of sizes but the appropriate size may not beavailable for smaller children. Preformed splints do not provide the same degree ofimmobilization as custom splints. Custom splits should be utilized when precise andcontinuous immobilization is required.EQUIPMENT1. Stockinet (optional)2. Plaster or fiberglass splinting/casting material3. Webril (splint padding)4. Warm water (room temperature)5. Elastic wrap, Tape, SlingCOMPLICATIONSCutaneous: pressure sores/necrosis, infection, thermal burnsNeurovascular compromise
PROCEDURE: SPLINTINGPREPARE Clean, repair and dress any skin lesions prior to splintingConsider removing clothing that will not be able to be removed afterEvaluate neurovascular statusSELECTAppropriate splint type (See table below)LENGTHUse unaffected extremity to measure the materialsIn general, the plaster is used to immobilize the joint above and jointbelow the injured area, if this is anatomically possibleThe stockinet should be longer than the splining material so that it can berolled over the ends of the splints.Cut dry plaster or fiberglass to fit area to be splinted. Plaster of Parisshould be slightly longer than needed as it retracts during settingWIDTHThe size of the plaster used in measured to cover approximately 50% ofthe circumference of the injured extremity. In an adult, this generallymeans 2 inch for the fingers, 3-4 inches for the upper extremity and 5-6inches for the lower extremityLAYERSIn an average sized adult, upper extremities should be splinted with 8-10layers of plaster. Lower extremities generally require 12-14 layers.PADDING Roll Webril around stockinet. This should be about 2-3 layers thick & eachturn should overlap the previous turn’s with by 25-50% of its thickness.Alternatively, layers of Webril (approximately ½ the number of layers asthe plaster & the same diameter as the plaster) may be usedOne additional layer of Webril is placed on the outside of the plaster (nonskin side) to avoid sticking of the elastic wrap to the plaster.Place additional padding (Webril) over boney prominences (such as theankle malleoli) to avoid pressure injuries.POSITION In general, splints are prepared to immobilize the effective limp in aposition of function. See individual splints to follow. There are exceptionsto this rule. 5th metacarpal neck fractures are position with the 5th MCP at70-90 degrees. Distal finger extensor tendon avulsion leading to Malletdeformity are splinted in extensionWETWet plaster/fiberglass material (not the padding)Plaster of Paris and water create an exothermic reaction. The watershould be at room temperature (ideally at 24 C) The plaster drying rate isdirectly related to water temperature. The colder the water, the longer thedrying time. As the water temperature approaches 40 C, the potential forserious burns from the splint doubles.Squeeze out excess water. Lie the plaster on a flat surface and smoothout any lumps or wrinklesAPPLYThe Webril-lined splint is then positioned over the area to be immobilizedPerform initial splint shaping at large joints. secured with an ACE wrap.Shape splint contours to final form.Maintain splint positioning until it has completely hardened.FINISHRe-evaluate and document neurovascular statusProvide a sling for comfort (upper extremity) or crutches (lower extremity)
SPLINT AFTERCAREThe patient or parent should be advised to avoid wetting the splint and to not to placeany objects between the skin and the splint. The lower end of the splint should beelevated to avoid further swelling. For example, a sling on the upper extremity should beposition so that the hand is above the level of the elbow. For lower extremity splints thefoot should be elevated on a chair if sitting or a pillow if lying. Ice can be applied to theoutside of the splint for pain but no longer than 15-20 minutes.They should return urgently for worsening pain under or distal to the splint. Numbnessor paresthesias. Follow up should be arranged within a week with an orthopedistSPLINT SELECTIONUpper VolarDistal forearmAlternative to sugar tong(not for young children)Wrist, forearmMetacarpalProximal phalanxElbowProximal humerusDistal1st metacarpalProximal phalanxScaphoidDistal femurProximaltibia/fibulaRadial for 2nd/3rd digitsUlnar for 4th/5th digitsPosterior (short)legDistal tibia/fibulaFootAnkleCrutches for children over6 yearsStirrupAnkle (includingAllows for weight bearingsoft tissue injuries) Fits in shoeLong armGutterSugar tongThumb spicaLong legLower ExtremitySplintsUseful for most upperextremity fracturesMust use slingCrutches for children over6 years
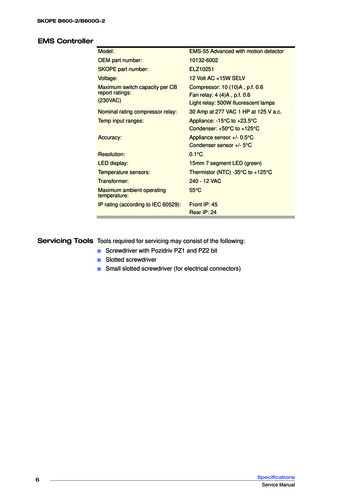
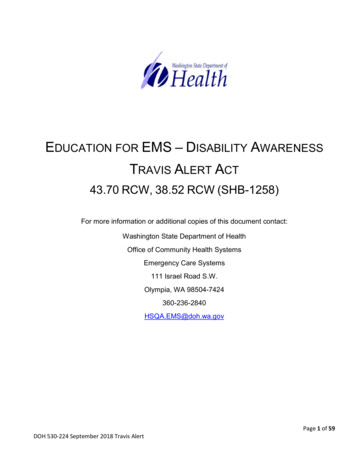
RADIAL/ ULNAR GUTTERINDICATIONSMetacarpal and/or proximal phalangealfractures.Ulnar gutter splint immobilizes the plain of4th and 5th digits.Radial gutter splint immobilizes plain of2nd and 3rd digits.DIMENSIONSWidth to wrap to midline of the hand ondorsal & volar surfaces.Length to extend from the nail base to theproximal forearm.POSITIONINGPosition patient with forearm verticallyerect.Shape the splint as follows:Wrist in neutral positionM-P joints in 70 flexion.P-I-P joints in 20-30 flexion.COMMENTSA thin layer of padding should be placedbetween the fingers to prevent irritation.Using a sling is optional to keep armelevated (not feasible in toddlers & infants
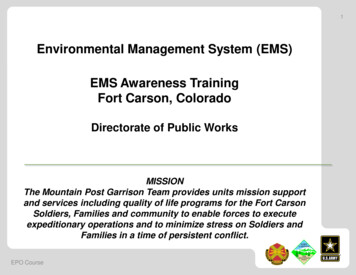
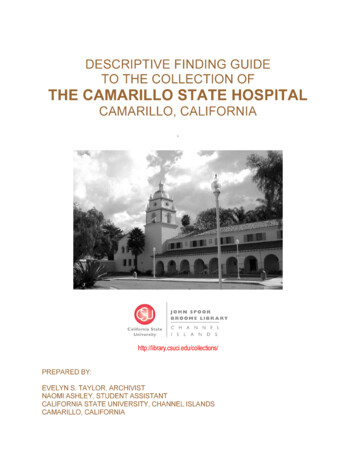
THUMB SPICAINDICATIONSA thumb spica splint is essentially a radialgutter splint adapted for immobilization ofthe thumb.Indicated for:Nondisplaced fractures of the firstmetacarpal bone.Nondisplaced fractures of the proximalphalynx of the thumb.Scaphoid fractures.Sprain of the ulna collateral ligamentDIMENSIONSDimensions are the same as for aradial/ulnar gutter splint.POSITIONINGWrist in neutral position.Thumb abducted & in slight flexion at theM-P and I-P joints.COMMENTSMay also make small cuts inplaster/fiberglass on both sides at the baseof the thumb to make it easier to wraparound thumb
VOLAR /COLLESINDICATIONSDistal forearm and wrist fractures.Also immobilizes the plane of the 2nd and3rd digits.DIMENSIONSWidth to fully cover volar aspect of theforearm.Length to extend from proximal fingers toproximal forearm along volar side offorearm.POSITIONINGPosition wrist in neutral position and digitsslightly flexed at all joints.COMMENTSUsing a sling is optional to keep armelevated (not feasible in toddlers & infants)May be extended to distal fingertips fordistal finger fractures or metacarpalfractures of the fingers/metacarpals 2-4.
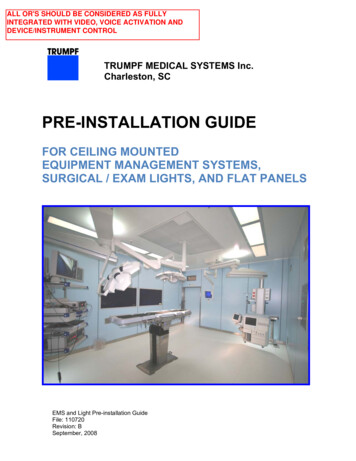
LONG ARM POSTERIORINDICATIONUsed for stable injuries in the elbowregion. For example, the patient withelbow pain in which no obvious fracture isseen but a joint effusion is present asevidence by an enlarged posterior fat pad.(Orthopedic consults are needed forsupracondylar fractures)DIMENSIONSWidth to cover ½ the arm circumference.Length to extend from the dorsal aspect ofthe mid-upper arm, over the olecranon,and down the ulnar aspect of the arm tothe distal palmar flexion crease.POSITIONINGPosition the child on his/her stomach withinjured arm hanging off stretcher withelbow at 90 angleAfter plaster/fiberglass is applied, shapethe splint with elbow flexed at 90 andforearm in neutral position.COMMENTSTo ensure comfort, provide extra paddingto any bony prominence.A sling must be worn to support the armbecause many casting materials cannotmaintain the 90 angle needed at theelbow.
SUGAR TONG (ARM)INDICATIONSBroad range of uses.Proximally, it can be used for stablehumerus fractures.Distally, frequently used for stableforearm and wrist fractures – provides themost effective immobilization in theseareas.A double sugar tong (both proximal anddistal at a 90 degree angle at the elbow)can be used to immobilize elbow injuries.DIMENSIONSWidth of the distal splint should slightlyoverlap the radial and ulnar edges of thearm.Length should extend from the dorsalaspect of the knuckles, around the elbow,to the volar palmar flexion crease.POSITIONINGPosition the child on his/her stomach withinjured arm hanging off stretcher withelbow at 90 angleAfter plaster/fiberglass & overwrap isapplied, shape splint and keep elbowflexed at 90 with the wrist in neutralposition.COMMENTSA sling is necessary to support the sugartong at the elbow.Analogous to a ankle stirrup splint
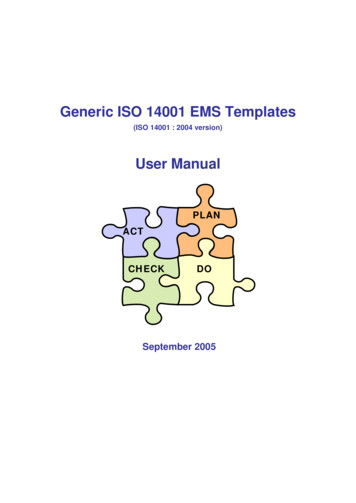
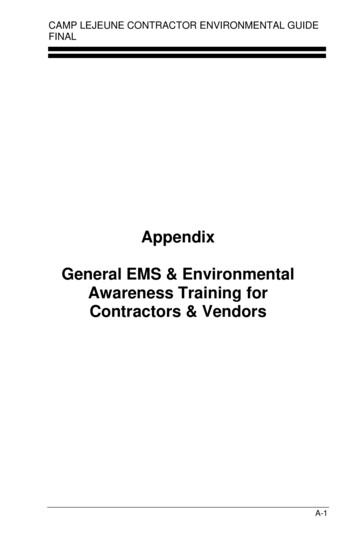
POSTERIOR / SHORT LEGINDICATIONSProvides support for injuries in:Distal tibia/fibulaAnkleFootDIMENSIONSWidth should cover at least ½ the legcircumference.Length should extend posteriorly fromlevel of the fibular neck over the heel ofthe foot to the base of the toes.POSITIONINGTo apply, position child prone on astretcher with knee flexed at 90 degrees.The foot should be placed in neutralposition at 90 to the leg.COMMENTSProvide extra padding at bonyprominences before addingplaster/fiberglass layer.Avoid pressure at fibular neck to preventcompression of peroneal nerve.Crutches are indicated for ambulationexcept for children under 6 years of age.
STIRRUP (LEG)INDICATIONSProvide lateral support for ankle fracturesor soft tissue injuries, preventinginversion and eversion.Often used in addition to posterior splintsto stabilize ankle fractures.DIMENSIONSWidth to cover at least ½ the legcircumference.Length to extend medio-laterally fromjust below the fibular head, around theheel and ending just below the medialaspect of the knee.POSITIONINGTo apply, position child prone on astretcher with knee flexed at 90 degrees.The foot should be placed in neutralposition at 90 to the leg.COMMENTSThese splints conveniently fit into a looseshoe.They allow weight bearing to be initiated.Crutches should be provided if fullweight-bearing is contraindicated.
also aid in the immobilization of soft tissue injuries such as fingertip amputations and . Many recent studies in the pediatrics have demonstrated that removable splints for . Nondisplaced fractures of the fi