Transcription
Lecture Notes on Information Theory Vol. 1, No. 1, March 2013Readiness Analysis of the Implementation ofIndonesian EHMS based on COBIT 5 EnablersAngelina P. Kurniati, Dawam D. Jatmiko, and Bayu MunajatTelkom Institute of Technology/ Informatics Faculty, Bandung, IndonesiaEmail: apk@ittelkom.ac.id, panggilakudawam@gmail.com, bayu1887@gmail.com Abstract—Implementation of EHMS in Indonesia is not asimple task. The parties related to the implementation,which are Health Ministry and healthcare organizations,should consider many factors related to the issue. Someindependent parties have tried to implement it, but none ofthem are really successful. It is important to analyse thereadiness of parties related, before the real implementationcan take place. One method which can be used to analysethis readiness is by reference to COBIT 5 enablers concept.This paper presents analysis of 7 (seven) enablers on COBIT5 as factors to be considered when Indonesian HealthMinistry wants to implement EHMS in Indonesia. Thisanalysis can be continued by implementing enablingprocesses as stated by COBIT 5.In this paper, the concept of enablers is used to assessreadiness of EHMS implementation in Indonesia. Dataand information presented in this paper were collectedthrough a review of literature, interviews and fieldsurveys, as well as data collected through questionnaires.Some theories and methods are used to support theanalysis of each of the enablers.II.A. COBIT 5 PrinciplesCOBIT 5 provides a comprehensive framework thatassists enterprises in achieving their objectives for thegovernance and management of enterprise IT. Simplystated, it helps enterprises create optimal value from ITby maintaining a balance between realising benefits andoptimising risk levels and resource use.Principles of COBIT 5 are:1) Meeting stakeholder needs. Enterprises exist tocreate value for their stakeholders by maintaining abalance between the realisation of benefits and theoptimisation of risk and use of resources.2) Covering the enterprise end-to-end. It covers allfunctions and processes within the enterprise. ItconsidersallIT-relatedgovernanceandmanagement enablers to be enterprisewide and endto-end.3) Applying a single, integrated framework. COBIT 5aligns with other relevant standards and frameworksat a high level, and thus can serve as the overarchingframework for governance and management ofenterprise IT.4) Enabling a hollistic approach. COBIT 5 defines aset of enablers to support the implementation of acomprehensive governance and management systemfor enterprise IT.5) Separating governance from management. Thesetwo disciplines encompass different types ofactivities, require different organisational structuresand serve different purposes.Index Terms— COBIT 5, enablers, principles, enabledimensions, EHMS, IndonesiaI.INTRODUCTIONThere are many initiatives separately to implement ehealth management system (EHMS) in Indonesia. Someinstitutions try to implement a fully automated system,some others automates the system partially. Theimplementation of EHMS in Indonesia involves severalstakeholders related to the system. Various factors needto be studied to assess the readiness of the various partiesimplementing EHMS.COBIT (Control Objectives for Information & RelatedTechnology) 5, as outlined below, introduces sevenenablers (they are explained below), which are factorsthat individually or collectively affect the success of thegovernance and management of IT in the enterprise. Theconcept of enablers is consistent with one of theprinciples of the COBIT 5, which apply a holisticapproach in solving governance and management withinthe organization. These seven interconnected enablersshould work properly to create a conducive environmentin implementing a good practice of EHMS.This paper is the documentation of the preliminary stepof research into the development of Indonesian EHMS.By doing analysis on enablers based on COBIT 5, it ispossible to provide a good understanding of the needs tobe fulfilled on the next steps of developing EHMSprototype.B. COBIT 5 EnablersPrinciple 4 of COBIT5 (enabling a hollistic approach)states that Efficient and effective governance andmanagement of enterprise IT require a holistic approach,taking into account several interacting components.Manuscript received Nov 30, 2012; revised Feb 1, 2013. 2013 Engineering and Technology Publishingdoi: 10.12720/lnit.1.1.11-16THEORY11
Lecture Notes on Information Theory Vol. 1, No. 1, March 20135 provides examples of good practices for someenablers provided by COBIT 5 (e.g., processes).For other enablers, guidance from other standards,frameworks, etc., can be used.COBIT 5 defines a set of enablers to support theimplementation of a comprehensive governance andmanagement system for enterprise IT.Enablers are broadly defined as anything that can helpachieving the objectives of enterprise. The COBIT 5framework defines seven categories of enablers:1) Principles, policies and frameworks are the vehicleto translate the desired behaviour into practicalguidance for day-to-day management.2) Processes describe an organised set of practices andactivities to achieve certain objectives and produce aset of outputs in support of achieving overall ITrelated goals.3) Organizational structures are the key decisionmaking entities in an enterprise.4) Culture, ethics and behavior of individuals and ofthe enterprise are very often underestimated as asuccess factor in governance and management.5) Informationispervasivethroughoutanyorganisation and includes all information producedand used by the enterprise. Information is requiredfor keeping the organisation running and wellgoverned, but at the operational level, information isvery often the key product of the enterprise itself6) Services, infrastructure and applications include theinfrastructure, technology and applications thatprovide the enterprise with information technologyprocessing and services.7) People, skills and competencies are linked to peopleand are required for successful completion of allactivities and for making correct decisions andtaking corrective actions.III.Analysis of the readiness of EHMS implementation inIndonesia is done based on the seven enablers in COBIT 5outlined above.A. Principles, Policies and FrameworksPrinciples and policies refer to the communicationmechanisms put in place to convey the governing body‟sand management‟s direction and anKesehatan Republik Indonesia (Ministry of Health,Republic of Indonesia) had defined some policies relatedto the implementation of EHMS, including the following: UU no 29/ 2004 about medical practices. It is statedthat medical record is a must for doctors andparamedics in caring patients. Kemenkes RI no 844/Menkes/SK/X/2006 about thedefinition of data code standards on health field. Thisdefines data code standards as reference of statisticsbureau, Health Ministry and Financial Ministry. Kemenkes RI no 129/Menkes/SK/II/2008 aboutMinimum Service Standard of Hospital. It statesmetrics for minimum service quality of a hospital. Kemenkes RI no 267/Menkes/SK/III/2008 aboutTechnical Guidance of Organizing Dinas KesehatanDaerah. Permenkes RI no 269/Menkes/PER/III/2008 aboutMedical Records. It consists of redefinition ofmedical records, the ownership, utility andresponsibility, organization and monitoring ofmedical records. Kemenkes RI no 828/Menkes/SK/IX/2008 aboutTechnical Guidance of Minimum Service Standardon Healthcare in District/ City. This policy guidesdistrict/ city in planning, implementing andmonitoring of Minimum Service Standard onHealthcare. UU no 36/2009 about health. It is stated thathealthcare institutions should give full access forresearch and development purposes. They shouldalso provide reports to the Health Ministry. Permenkes RI no 1144/Menkes/PER/VIII/ 2010 aboutorganization and workflow of Health Ministry. Kemenkes RI no 1625/Menkes/SK/VIII/2011 aboutOfficers of Information and Documentation in HealthMinistry.On implementation level, each healthcare organizationcan have its own procedures and rules to be appliedlocally in the organization.C. COBIT 5 Enabler DimensionsAll enablers have four common dimensions, which are:1) Stakeholders – Each enablers has stakeholders(parties who play an active role and/or have aninterest in the enabler). For example, processeshave different parties who execute processactivities and/or who have an interest in the olders, each with his/her own roles andinterests, that are part of the structures.Stakeholders can be internal or external to theenterprise, all having their own, interests and needs.Stakeholders‟ needs translate to enterprise goals,which in turn translate to IT-related goals for theenterprise.2) Goals - Each enabler has a number of goals, andprovides value by the achievement of these goals.3) Life cycle - Each enabler has a life cycle, frominception through an operational/useful life untildisposal. This applies to information, structures,processes, policies, etc.4) Good practices - For each of the enablers, goodpractices can be defined. Good practices supportthe achievement of the enabler goals. Goodpractices provide examples or suggestions on howbest to implement the enabler, and what workproducts or inputs and outputs are required. COBIT 2013 Engineering and Technology PublishingANALYSISB. ProcessesA process is defined as „a collection of practicesinfluenced by the enterprise‟s policies and proceduresthat takes inputs from a number of sources (includingother processes), manipulates the inputs and producesoutputs (e.g., products, services)‟ [2].12
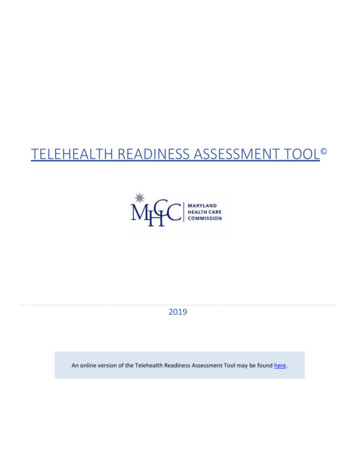
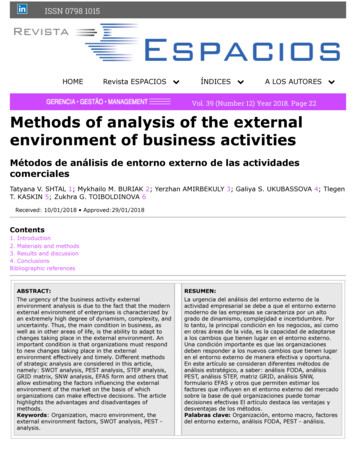
Lecture Notes on Information Theory Vol. 1, No. 1, March 2013The processes of e-health management system [1]can be categorized as:1) Administrative processes, consist of patientidentification and assessment.2) Laboratory processes, consist of order records,results from laboratory instruments, scheduling andbilling.3) Radiology processes, include patient tracking,scheduling, results reporting, and image tracking.4) Pharmacy processes, consist of filling prescriptionsand payer formularies and medicine administration.5) Clinical documentation processes, for example:physician, nurse and other clinician notes; flowsheets; transcription document management,discharge summaries, medical records abstracts,chart tracking, utilization management, etc.6) Reporting processes, consist of summarizing dataand creating reports to be sent to the HealthMinistry.The categorization of processes is not strictly appliedin all healthcare organizations. The organization candefine their own categorization according to theirorganizational structures.and evaluation in the field of health coaching efforts.Organizational structure of BUK shown in Figure 4 [5].Balitbangkes functions in doing and monitoringresearch and development in health subjects. To do this,Balitbangkes establishes some technical policy, planningand research dan development in health subjects. It isresponsible for formulating, implementing, monitoring,evaluating and reporting technical policies, plans andprograms of health research and development.Pusdatin is a supporting unit of Health Ministry inhealth data and information, to manage health statistics,information analysis dan dissemination, and informationsystem and bank data development. Pusdatin, especiallysubfield of information systems development, under thedevelopment of information systems and data banks, isthe most responsible division because it is responsible fordeveloping and maintaining all systems.These three units are responsible for governance rolesof healthcare management system. They are responsiblefor evaluating, directing and monitoring the managementroles of e-health. Management roles are done bymanagement levels in hospitals. Management level willbe executing the policies, plans and programs of HealthMinistry and planning, building, running and monitoringthe processes includes in the system.C. Organizational StructuresOrganizational structure shows the responsibilitysetting, separation of duties and chains of commandwithin an organization. Fig. 1 shows the organizationalstructure of Ministry of Health, Indonesia [3].D. Culture, Ethics and BehaviorCulture, ethics and behaviour refer to the set ofindividual and collective behaviours within an enterprise.Indonesian‟s culture as defined by Hofstede can befigured as on Fig. 2 [8].Figure 1. Organizational structure of Ministry of Health, Indonesia[3]Three most important parts of the Ministry of Healthorganizational structure related to e-health research areDirjen Bina Upaya Kesehatan (BUK), Badan Penelitiandan Pengembangan Kesehatan (Balitbangkes), and PusatData dan Informati (Pusdatin).BUK has a task to formulate and implement policiesand technical standardization in the field of healthdevelopment efforts. In doing this task, BUK formulatingpolicies in development of health efforts, giving technicalcoach and evaluation of health development efforts, andadminister the health development efforts. BUK isresponsible for setting policy, norms, standards,procedures and criteria and to provide technical guidance 2013 Engineering and Technology PublishingFigure 2. Indonesian cultureAs shown ini Fig. 3, Indonesia has a high score (78) ofPDI (Power Distance Index), which means that theIndonesian style is being dependent on hierarchy, unequalrights between power holders and non power holders,superiors in-accessible, leaders are directive, managementcontrols and delegates. Power is centralized andmanagers count on the obedience of their teammembers. Employees expect to be told what to do andwhen. Control is expected and managers are respected fortheir position.13
Lecture Notes on Information Theory Vol. 1, No. 1, March 2013Pasien/ keluargaSurat pengantarRawat JalanSurat pengantarPerinatologiSurat pengantarUGDSurat pengantarPasien/ keluargaSurat pendaftaranrawat inapSurat tandapendaftaranrawat inapMencatat data pasienrawat inapSurat PengantarDokterSurat pengantarHotel Service/Laporan PerbaikanCRM RanapLaporanpemakaianDDB Rekam MedikPermintaan barangdan alat medikBBukuperbaikanalat medikMelakukanpemeliharaanalat medisMenyediakan barangsesuai permintaanMelaksanakanpengkajian dantindakan keperawatanFormpemakaianalat medisMaterial ControlBuku permintaanbarang, alat medisAPassosmedHasilATujuan tercapai?TidakYaSurat keterangan dokter,Surat permintaanmenguburMenerima informasidari dokterpasien boleh pulangKamar JenasahRekam MedikSurat pernyataanserah terimajenazahPerinatologiRekam MedikICU/ NICU/PICU/ SU-ICLaporanpemakaianPerlu homecare?BTidakKamar OperasiRekam MedikSerahterimadengan pasienatau keluargaHemodialisaRekam MedikYaSuratpengantardari dokterFarmasiResep, obatRS LainSurat pengantarRekammedikSurat permohonanlayanan home careRekam MedikRekam medikMelakukan persiapanalat dan fasilitasyang diperlukanMenerima informasipenempatan pasien barudan pemesanan tempatCDMemberikaninformasi pasienbatal pindahSuratpermohonan sewaalat kesehatanKeluarga setuju?YaAAlat tersedia?Melakukan kunjungan danevaluasi tindakanTidakArsipTidakDaftar tarifsewa alat, suratperjanjianPerlu dilanjutkan?Bukusewa alatYa penerimaan pasien baruTidakMenerima pembayaransewa alat, menyerahkanalatMelakukan transaksipembayaranbersama keluargaFC kwitansi,rekam medik pelayanan keperawatan administrasi keperawatanDFCkwitansi,buku sewaalat pengelolaan tempat Home CareFigure 3. IPMap of a HospitalIn IDV (individualism), Indonesia has a low score (14).This means there is a high preference for a stronglydefined social framework in which individuals areexpected to conform to the ideals of the society and thein-groups to which they belong. Indonesia has a lowscore (46) of MAS (masculinity). Indonesia is lessMasculine than some other Asian countries like Japan,China and India. In Indonesia status and visible symbols 2013 Engineering and Technology Publishingof success are important but it is not always material gainthat brings motivation. The UAI (uncertainty avoidanceindex) score for Indonesia is medium low (48). Thismeans that there is a strong preference in Indonesiatoward the Javanese culture of separation of internal selffrom external self. When a person is upset, it is habitualfor the Indonesian not to show negative emotion or angerexternally. They will keep smiling and be polite, no14
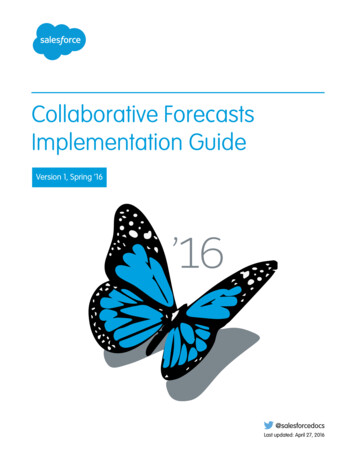
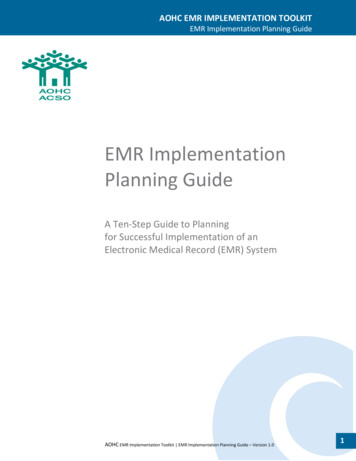
Lecture Notes on Information Theory Vol. 1, No. 1, March 20131.Patients should be able to access and view theirmedical records through the system2. Information in the system should be up-to-date3. Medical information should be presented in acognitively accessible way4. Patients should be able to edit their medical records,annotate them or in the least request the responsiblemedical professionals to make correctionis for them5. The system should be technically accessible6. Each individual should control access to their data7. A possibility for an emergency access should existAn individual should know who accessed their accountand what actions were performedmatter how angry they are inside. This also means thatmaintaining work place and relationship harmony is veryimportant in Indonesia, and no one wishes to be thetransmitter of bad or negative news or feedback.E. InformationThe information enabler deals with all informationrelevant for enterprises. Information can be structured orunstructured, formalised or informalised.Information flow in a healthcare organization can beillustrated using IPMap notation. It shows data andinformation elements in an organization and therelationships through processes. The medical record dataflow from admission process of a patient and are saveduntil some years to keep a historical record of thatpatient‟s health. An example of information flow of ahospital in IPMap notation is shown at Fig. 3.The start of administrative processes is registrationprocess (Mencatat data pasien). The patient data is savedin medical record database (DB rekam medik). Thepatient is then observed by the paramedic, who decidesthe next treatment to be done. Patient can get involved inlaboratory processes (laboratorium), radiology processes(radiologi), and/or pharmacy processes (farmasi), basedon the diagnostic of paramedic. Any treatment receivedby patients will be recorded in the medical record, basedon clinical documentation processes done by paramedics.In addition, the supporting processes are also appliedin the healthcare system in hospitals. The use of drugsand medical devices (Menyediakan obat dan alat medis)is analyzed for any health care service provided topatients. The usage of inpatient rooms is also recorded tomeasure the occupancy and hospital capacity.The sample of hospital also provides home careservices that can be used by patients. When a patientobtain this service, patients can receive health careservices in patients' homes. Health workers will visitaccording to a predetermined schedule, providing healthcare, and noted the visit in the patient's medical record.All data generated during the health care will be storedin a database of medical records. The e-healthmanagement system is designed to generate subsequentreports of such activity automatically in accordance withthe provisions of the health.G. Services, Infrastructure and ApplicationsThe type of minimal hospital services are as stated inKemenkes RI no 129/Menkes/SK/II/2008 about MinimumService Standard of Hospital. The e-Health ManagementSystem is expected to has the following maincharacteristics [9]:1. Patients should be able to access and view theirmedical records through the system2. Information in the system should be up-to-date3. Medical information should be presented in acognitively accessible way4. Patients should be able to edit their medical records,annotate them or in the least request the responsiblemedical professionals to make correctionis for them5. The system should be technically accessible6. Each individual should control access to their data7. A possibility for an emergency access should exist8. An individual should know who accessed theiraccount and what actions were performedFigure 4. System ArchitectureF. Services, Infrastructure and ApplicationsThe type of minimal hospital services, as stated inKemenkes RI no 129/Menkes/SK/II/2008 about MinimumService Standard of Hospital, are: Emergency services,Outpatient and inpatient services, Surgical services,Service delivery and perinatology, Intensive care,Radiology services, Clinical pathology laboratoryservices, Medical rehabilitation services, Pharmacy andnutrition services, Blood transfusion services, Poorservice, Medical record service, Waste esambulance/ hearse, Services undertakers, Laundryservices, Maintenance of hospital services, andPrevention of Infection Control.The e-Health Management System is expected to hasthe following main characteristics [9]: 2013 Engineering and Technology PublishingService capabilities refer to resources such asapplications and infrastructures that are leveraged in thedelivery of IT-related services. It should be able tointegrate the need of healthcare organization to managehealth records of their patient, the interconnectionbetween healthcare organizations, and the reportingfunctions from each organization to the Health Ministry.Architecture of services and application proposed in thisresearch is shown at Fig. 4.H. People, Skills and CompetenciesThe last enabler to take care is people, skills andcompetencies. Data of paramedics in Indonesia can besummarized as in Table 1 [7].Health Ministry through its personnel bureau, based onPermenkes 1144/ 2010, is doing human resource15
Lecture Notes on Information Theory Vol. 1, No. 1, March 2013The authors wish to thank Rendy Radofara, WisnuArimurti, and Aditya Ananda Uttama as the supportingteam in doing this reseach. This work was supported inpart by a grant called Hibah Bersaing from Dirjen DIKTI,Indonesia.management processes, including the preparation offormation and human resource recruitment, civilassignment, non-permanent employee assignment, rankassignment, transfer and discharge, assesment and careerdevelopment, functional degree administration, awardsand employee welfare. This bureau also conductsplanning, monitoring, evaluation and reporting, and theimplementation of administrative affairs of the bureau.IV.REFERENCES[1]CONCLUSION[2]This preliminary analysis of readiness on EHMSimplementation in Indonesia can be helpful in creatingconducive environments in implementing IT in healthfield. It can be concluded that:1. Principle, policies and framework of health systemis complete and allows the implementation of anEHMS.2. Processes within the healthcare service might bechanged due to the implementaion of EHMS.3. Organizational structure of health ministry andbelow is not ready to implement EHMS becausethey have not enough IT employees who canoperate EHMS.4. Culture, ethics ad behavior of individuals in theenterprise should be taken care of to support theimplementation of EHMS smoothly.5. Information and the data related to the EMS havebeen collected separately and need to be integratedso that the system can run optimally.6. Services, infrastructure and application of EHMSshould be prepared based on processes and otherenablers setting.7. People, skills and competencies should be managedcarefully because this is the most crucial enabler ofsuccessful implementation of e-health managementsystem. Competence and expertise of the peopleinvolved in it must also be increased in accordancewith the needs of the system.[3][4][5][6][7][8][9]Angelina P. Kurniati was born in Kudus, Indonesia, on July 4, 1983.She completed a graduate degree at Informatics Engineering, TelkomInstitute of Technology, Bandung – Indonesia; and a post-graduatedegree at Magister of Informatics Engineering, Bandung Institut ofTechnology, Bandung – Indonesia.She is now working as a lecturer at Informatics Faculty, TelkomInstitute of Technology, and hold the position as Head of InformaticsLaboratories and Workshop. Previous publications related to this paperare: [1] “Perancangan e-Health Management System” (Designing eHealth Management System), presented on National Conference ofInformation system, Indonesia, 2012; [2] “Information QualityManagement for Telehomecare”, presented on International Conferenceof Information and Communication Technology and Systems, Indonesia,2010; [3] “Designing IQMM as a Maturity Model for InformationQuality Management”, presented on Informing science and ITEducation Conference, Italy, 2010.ACKNOWLEDGMENT 2013 Engineering and Technology PublishingElectronic Health Records Overview. National Institutes of HealthNational Center for Research Resources. 2006.COBIT 5: A Business Framework for the Governance andManagement of Enterprise IT. ISACA, Los Angeles. 2012.Official Website of Indonesia Health Ministry. [Online]. Available:http://www.depkes.go.idOfficial Website of Badan Penelitian Dan PengembanganKesehatan. Indonesia Health Ministry. [Online]. al Website of Bina Upaya Kesehatan. Indonesia HealthMinistry. [Online]. Available: http://buk.depkes.go.idOfficial Website of Pusat Data dan Informasi. Indonesia HealthMinistry. [Online]. Available: http://www.depkes.go.id/datinHealth Ministry Data and Information. July 2011.Hofstede, Geert. Drivers of Indonesian Culture.S. Ali, D. Chornyi, C. Mauro, and H. Kremar, “Evaluationframework for personal health records: Microsoft healt valut vs.google health,” in Proc 43rd Hawaii International Conference onSystem Sciences, 2010.16
COBIT 5 provides examples of good practices for some enablers provided by COBIT 5 (e.g., processes). For other enablers, guidance from other standards, frameworks, etc., can be used. III. ANALYSIS Analysis of the readiness of EHMS implementation in Indonesia is done based on the s