Transcription
Comprehensively updated and significantlyexpanded to include the latest recommendations,findings from leading-edge research, emergentdiagnostic tools, and new therapeutic options,Essential Cardiac Electrophysiology: The SelfAssessment Approach now offers coverage of someof hottest topics in EP, including: HCN channelsCongenital and paroxysmal AV blocksLeft atrial flutterElectrophysiologic assessment of AVNRTand AVRTBystander v/s participating accessory pathwayVT ablationShort QT syndromeGenetics of ARVDEarly repolarization and ventricular fibrillationAortic cusp VTCommotio cordisWeight loss supplements and cardiac arrhythmiasZainul Abedin, MD, FRCP, FHRSProfessor of Clinical MedicinePaul Foster School of MedicineTexas Tech University HealthSciences Center;Adjunct Professor ofElectrical Engineeringand Computer ScienceUniversity of Texas at El PasoEl Paso, TX, USATitles of Related Interest:Bayes de LunaClinical Electrophysiology:A Textbook, Fourth EditionISBN: 978-0-470-65859-8KusumotoECG Interpretation for Everyone:An On-the-Spot GuideISBN: 978-0-470-65556-6Second EditionEssential CardiacElectrophysiologyThe Self-Assessment ApproachSecond EditionFact-based and clinically-focused, Essential CardiacElectrophysiology: The Self-Assessment Approach isan ideal reference for all members of the EP careteam, from cardiac care nurses and techniciansto EP and cardiology fellows to practicingelectrophysiologists. Packed with questionsdesigned to aid readers’ understanding of keyconcepts and retention of essential facts, it is anexcellent study aid for those preparing for boardexamination or other EP certifications.Essential Cardiac ElectrophysiologyThis new edition of Essential CardiacElectrophysiology: The Self-Assessment Approachcontinues the successful formula of the firstedition, providing a concise and thoroughoverview of electrophysiology supplemented bychallenging questions readers can use to test theirknowledge and prepare for examinations.AbedinEssential Cardiac ElectrophysiologyThe Self-Assessment ApproachISBN 978-1-444-33590-39 781444 335903Zainul Abedin
Essential Cardiac Electrophysiology
DedicationTo all the students of cardiac electrophysiologyandTo my mentors: Dr. Fred Morady, Dr. Mark Josephson,Dr. Masood Akhtar, Dr. Warren Jackman, Dr. James Maloney,Dr. Christopher Wyndham, Dr Eric Prystowsky, Dr George Klein andDr Kalyanam ShivkumarandTo my wife Karuna whose patience and understanding madethis project possible.andTo my children Moeen, Sakena and Zameerand my grandchildren Neela and Sameer Yidroose
Essential CardiacElectrophysiologyThe Self-Assessment ApproachSecond EditionZainul Abedin, MD, FRCP, FHRSProfessor of Clinical MedicinePaul Foster School of MedicineTexas Tech University Health Sciences Center;Adjunct professor of Electrical Engineering and Computer ScienceUniversity of Texas at El PasoEl Paso, TX, USAA John Wiley & Sons, Ltd., Publication
This edition first published 2013 2013 by Blackwell Publishing LtdBlackwell Publishing was acquired by John Wiley & Sons in February 2007. Blackwell’s publishingprogram has been merged with Wiley’s global Scientific, Technical and Medical business to formWiley-Blackwell.Registered OfficeJohn Wiley & Sons, Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UKEditorial Offices9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK111 River Street, Hoboken, NJ 07030-5774, USAFor details of our global editorial offices, for customer services and for information about howto apply for permission to reuse the copyright material in this book please see our website atwww.wiley.com/wiley-blackwellThe right of the author to be identified as the author of this work has been asserted in accordancewith the UK Copyright, Designs and Patents Act 1988.All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, ortransmitted, in any form or by any means, electronic, mechanical, photocopying, recording orotherwise, except as permitted by the UK Copyright, Designs and Patents Act 1988, without theprior permission of the publisher.Designations used by companies to distinguish their products are often claimed as trademarks. Allbrand names and product names used in this book are trade names, service marks, trademarks orregistered trademarks of their respective owners. The publisher is not associated with any productor vendor mentioned in this book. This publication is designed to provide accurate and authoritativeinformation in regard to the subject matter covered. It is sold on the understanding that the publisheris not engaged in rendering professional services. If professional advice or other expert assistance isrequired, the services of a competent professional should be sought.The contents of this work are intended to further general scientific research, understanding, anddiscussion only and are not intended and should not be relied upon as recommending or promotinga specific method, diagnosis, or treatment by physicians for any particular patient. The publisher andthe author make no representations or warranties with respect to the accuracy or completeness of thecontents of this work and specifically disclaim all warranties, including without limitation any impliedwarranties of fitness for a particular purpose. In view of ongoing research, equipment modifications,changes in governmental regulations, and the constant flow of information relating to the use ofmedicines, equipment, and devices, the reader is urged to review and evaluate the informationprovided in the package insert or instructions for each medicine, equipment, or device for, amongother things, any changes in the instructions or indication of usage and for added warnings andprecautions. Readers should consult with a specialist where appropriate. The fact that an organizationor Website is referred to in this work as a citation and/or a potential source of further information doesnot mean that the author or the publisher endorses the information the organization or Website mayprovide or recommendations it may make. Further, readers should be aware that Internet Websiteslisted in this work may have changed or disappeared between when this work was written and whenit is read. No warranty may be created or extended by any promotional statements for this work.Neither the publisher nor the author shall be liable for any damages arising herefrom.Library of Congress Cataloging-in-Publication DataAbedin, Zainul, MD.Essential cardiac electrophysiology : the self-assessment approach / Zainul Abedin. – 2nd ed.p. ; cm.Includes bibliographical references and index.ISBN 978-1-4443-3590-3 (pbk. : alk. paper) – ISBN 978-1-118-52199-1 (obook) –ISBN 978-1-118-52200-4 (emobi) – ISBN 978-1-118-52201-1 (epdf) –ISBN 978-1-118-52202-8 (epub)I. Title.[DNLM: 1. Arrhythmias, Cardiac–physiopathology–Handbooks. 2. Arrhythmias,Cardiac–therapy–Handbooks. 3. Cardiac Electrophysiology–methods–Handbooks.4. Electrophysiologic Techniques, Cardiac–Handbooks. WG 39]612.1′71–dc232012043159A catalogue record for this book is available from the British Library.Wiley also publishes its books in a variety of electronic formats. Some content that appears in printmay not be available in electronic books.Cover image: courtesy of the authorCover design by Andy Magee Design LtdSet in 9.5/12pt Meridien by SPi Publisher Services, Pondicherry, India12013
ContentsForeword, viPreface, viiAcknowledgements, viiiAbbreviations, ix1 Ions channels and currents, 12 Electrophysiologic effects of cardiac autonomic activity, 383 Mechanisms of arrhythmias, 504 Sinus node dysfunction and av blocks, 675 Supraventricular tachycardia, 946 Differential diagnosis of wide complex tachycardia, 2197 Ventricular tachycardia and ventricular fibrillation, 2268 Sudden cardiac death and risk stratification, 3699 Cardiac arrhythmias in patients with neuromuscular disorders, 38810 Syncope, 39411 Pharmacologic therapy of arrhythmias, 40712 Electrical therapy for cardiac arrhythmias, 445Index, 494v
ForewordThe second edition of Essentials of Cardiac Electrophysiology continues in the sameformat as the first edition – a concise review in bullet-point fashion of the mostimportant facts dealing with all major topics in clinical cardiac electrophysiologyand with selected basic electrophysiology topics that are the most relevant toclinical electrophysiologists. The second edition has been enhanced both by expanding some of the topics previously covered and by the addition of somenew topics. For example, additional information useful for those wishing toreview cardiac membrane channels has been provided. A notable number ofissues directly related to clinical practice have been expanded upon or added,including post-maze arrhythmias, the genetics of atrial fibrillation, new oralanticoagulants, left ventricular non-compaction, the use of magnetic resonance imaging in patients with a device, and management of high defibrillation thresholds.All in all, this book remains a very useful resource for those seeking a concisereview of the most important information on virtually any topic important toclinical cardiac electrophysiologists.Fred Morady, MDMcKay Professor of cardiovascular DiseaseProfessor of MedicineUniversity of Michigan Health SystemAnn Arbor, MI, USAvi
PrefaceThere are known knowns, there are known unknowns, but there are also unknownunknownsD onald R umsfeldI use this quotation with some trepidation because of its use in justifying the Iraqwar. But I feel it also describes the state of knowledge in many scientific fieldsincluding cardiac electrophysiology.There has been an exponential increase of information in all facets of cardiacelectrophysiology. When the first edition of Essential Cardiac Electrophysiology was published there were seven known types of long QT syndromes; by the time thisedition went into press the list had expanded to 12 different types of long QTsyndromes.The question is invariably raised as to why we need another book on cardiacelectrophysiology when, with the availability of the world wide web and smarthandheld devices, the information can be accessed anytime anywhere withina few seconds. The answer to this question lies in the ability of this text to assimilate, synthesize and present only factual and relevant information.As Albert Einstein has eloquently said, “Everything should be made as simple aspossible, but not one bit simpler.”Learning is best accomplished by testing, reiteration, and concentration onessential information, accomplished in this book by using a self-assessmentapproach, illustrations, tables and an enumeration of factual information inbullet format rather than by verbose description.The first edition has been immensely popular among cardiac electrophysiology and cardiology fellows, residents, and medical students. Keeping thesame format, this edition has been expanded by 50% with new information,multiple-choice questions and illustrations.This has been a long and immensely time-consuming project. The rewardsare not financial. These rewards are realized in the form of compliments from students and encouraging remarks from their mentors.Any project of this magnitude is likely to have errors and or omissions. Anyconstructive criticism, comments, and suggestions are always welcomed.Please send comments, critiques and suggestions to, ‘essentialep@gmail.com’.Zainul Abedinvii
AcknowledgementsI gratefully acknowledge the generous help of Professor Fred Morady, a truescholar and a superb teacher, in reviewing the manuscript and in providingmany valuable suggestions.I am grateful to Ms. Susan Fernandez for secretarial assistance; and toMr. Thomas Hartman, Ms. Kate Newell, Ms. Cathryn Gates and Ms. M ahabunnisaMohamed and other members of Wiley-Blackwell e ditorial, publishing andmarketing team.viii
opyridineAntiarrhythmic drugsAlpha1 acid glycoproteinATP binding cassette proteinAcetylcholineAdenosineAtrial fibrillationAccelerated idioventricular rhythmAutomatic junctional tachycardiaA kinase anchoring proteinsAction potentialAccessory pathwayAction potential durationAtrial refractory periodArrhythmogenic right ventricular dysplasia/cardiomyopathyAtrial tachycardiaAngiotensin IIAdenosine triphosphateAnti tachycardia pacingAndersen–Tawil SyndromeAV dissociationAtrioventricular nodeAVN re-entry tachycardiaAV re-entrant tachycardiaBundle branch blockBundle branch re-entry VTBaroreflex sensitivityCalciumCoronary artery diseaseCyclic adenosine monophosphateCardiac autonomic nervous systemCongestive heart failureComplete heart blockCalcium induced calcium releaseCycle lengthChlorideCatecholaminergic polymorphic ventricular tachycardiaCoronary sinusCerebrospinal fluidCorrected sinus node recovery timeix
x AbbreviationsCXConnexionCYPCytochrome PDADDelayed after-depolarizationDCMDilated cardiomyopathyDFTDefibrillation thresholdEADEarly after depolarizationEAMElectroanatomical mapEFEjection fractionEHLElimination half lifeEREustachian ridgeERPEffective refractory periodHBHis bundleHCMHypertrophic cardiomyopathyHCNHyperpolarization activated cyclic nucleotide gatedHERGHuman ether related a-go-go gene proteinHPSHis Purkinje systemHRVHeart rate variabilityHRTHeart rate turbulenceICa TCa current transient or short actingICaLCa current long actingICEIntracardiac echocardiographyICDImplantable cardioverter-defibrillatorIfHyperpolarizing cation currentIKPotassium currentIK1Inward rectifying potassium currentIKachAcetylcholine mediated potassium currentIK,ATPATP dependent potassium currentIKpTime independent background plateau currentIKrRapidly activating potassium currentIKsSlowly activating potassium currentIKurUltra rapid potassium currentINaSodium currentIP3Inositol triphosphateISTInappropriate sinus tachycardiaItoTransient outward currentIVCInferior vena cavaKPotassiumKvLQT1 Voltage-dependent potassium controlling proteinLAFBLeft anterior fascicular blockLCSDLeft cardiac sympathetic denervationLIPVLeft inferior pulmonary veinLOCLoss of consciousnessLQTSLong QT SyndromeLSPVLeft superior pulmonary veinLVHLeft ventricular hypertrophyLVOTLeft ventricular outflow tract
RCSNDSMVTSNRTSQTSSRSSSMuscarinicMyosin heavy chainMaximum diastolic potentialMyocardial infarctionMinimal potassium current controlling proteinManganese chlorideMaximum tracking rateMonomorphic ium and calcium exchangeNoncoronary cuspNonsustained VTPurinergicPremature atrial contractionsParoxysmal AV blockPulseless cardiac electrical activityProgressive cardiac conduction diseaseProgrammed electrical stimulationP glycoproteinPermanent form of junctional reciprocating tachycardiaProtein kinase APost pacing intervalPostventricular atrial refractory periodPremature ventricular contractionsCorrected QT intervalRight bundleRight coronary cuspRestrictive cardiomyopathyRadiofrequencyRibonucleic acidRight superior pulmonary veinRight ventricular outflow tractRyanodine receptorSino atrial conduction timeSignal average ECGSinoatrial nodeSudden cardiac deathSarcoplasmic Ca release channelSinus node dysfunctionSustained monomorphic VTSinus node recovery timeShort QT syndromeSarcoplasmic reticulumSick sinus syndrome
xii AbbreviationsSURSulfonylurea receptorSVCSuperior vena cavaSVTSupraventricular tachycardiaTATricuspid annulusTCLTachycardia cycle lengthTDPTorsades de PointesTDRTransmural dispersion of repolarizationTEETransesophageal echocardiographyTIATransient ischemic attackTWA T wave alternansULV Upper limit of vulnerabilityVA VentriculoatrialVF Ventricular fibrillationVRP Ventricular refractory periodVT Ventricular tachycardiaWCT Wide complex tachycardiaWPW Wolff–Parkinson–White syndrome
chapter 1Ions channels and currentsSelf-assessment questions1.1 Potassium channels and currents1 In normal Purkinje fibers which one of the following currents is responsiblefor normal automaticity?A If hyperpolarization-activated cyclic nucleotide gated currentB ICaL L-type calcium currentC INa rapid inward sodium currentD IK delayed rectifier potassium currentE Ito transient outward current2 Abnormal potassium channel function is unlikely to causeA Deafness.B Short QT interval.C Long QT interval.D Catecholaminergic polymorphic ventricular tachycardia.3 Osborn waves seen in hypothermia are the result of:A Uneven distribution of Ito in endocardium and epicardium.B Sarcoplasmic calcium overload.C Metabolic acidosis.D Loss of function of the sodium channel.4 Which of the following is the result of outward movement of the potassiumions across the cell membrane?A Repolarizing current.B Depolarizing current.C Prolongation of the QT interval.D Prominent U waves.Essential Cardiac Electrophysiology: The Self-Assessment Approach, Second Edition. Zainul Abedin. 2013 Blackwell Publishing Ltd. Published 2013 by Blackwell Publishing Ltd.1
2 Essential Cardiac Electrophysiology5 I n a diagram of AP shown below, which one of the following currents isactive where arrow is pointing?ABCDItoIK1INaICa6 Which one of the following genes controls the expression of IKr?A KCNQ1 (KvLQT1)B KCNH2 (HERG)C SCN5AD MinK7 Which one of the following actions is likely to activate IKatp current?A Rise in intracellular ATPB Rise in intracellular calciumC Fall of Intracellular ATPD Fall of Intracellular calcium8 How does congestive heart failure affect depolarizing/repolarizing currents?A Outward Repolarizing currents are reducedB Inward depolarizing currents are reducedC Outward repolarizing currents are increasedD APD is decreased9 W hich one of the following is least likely to occur with prolongation of plateau phase of the AP?A Increased strength of contractionB Increase in conduction velocityC Increased duration of contractionD Increased refractoriness10 Which one of the following is likely to increase the activity of IKr?A Increased extracellular potassiumB Exposure to Sotalol
Ions channels and currents 3C Decrease extracellular potassiumD Increase in chloride current11 When does the reverse use dependent block occur?A It occurs with repeated activation of channelB It occurs when sodium channel is blockedC It occurs at slow heart rate but not at fast heart rateD It occurs in the presence of catecholamines12 Which one of the following is least likely attribute of Ito?A It is present in ventricular epicardium but not in endocardiumB It is responsible for spike and dome characteristicC It is blocked by RanolazineD It is also present in human atrium13 Which one of the following is associated with Brugada syndrome?A Defect in SCN5A geneB Loss of IKrC ST segment depression is precordial leadsD Deafness14 Which one of the following agents/actions is likely to block IKs?A AminophyllineB IndapamideC Activation of protein kinase CD ErythromycinE Increase in intracellular calcium1.2 Sodium channels and currents1 Chronic exposure to Na channel blocking antiarrhythmic drugs may result in:A Increase in sodium channel messenger RNA, which counteracts the effectsof channel blockade.B Hyponatremia at cellular level.C Decrease in Na/K ATPase.D Decrease in sodium channel messenger RNA, resulting in steady state-level.2 Which of the following statement about Na/K ATPase is incorrect?A It is an enzyme responsible for the maintenance of Na and K concentrationgradients in the cells.B Its operation produces an inwardly directed current as 1 Na ion is removedfrom the cell in exchange for the influx of 3 K .C The sodium pump performance determines the level of intracellular Na level and, consequently, cardiac inotropic status.D Changes in intracellular Na levels influence the activity of the cardiacNa -Ca2 exchanger.
4 Essential Cardiac Electrophysiology3 S CN5A mutation resulting in loss of function is responsible for which one ofthe following rhythm disorders?A Progressive cardiac conduction disease (PCCD).B Long QT syndrome.C Catecholaminergic polymorphic ventricular tachycardia.D Paroxysmal atrial fibrillation.4 W hich one of the following currents is likely to occur when the Na movesacross the cell membrane and into the cell?A Inward currentB Outward currentC Repolarizing currentD Hyperpolarizing current5 A patient receiving a Na channel blocker develops AF with rapid ventricularresponse. What changes on ECG can be anticipated to occur?A Narrowing of the QRS complex during tachycardiaB Widening of the QRS complex during tachycardiaC Prolongation of the QT intervalD Shortening of the QT interval6 What is likely to happen when a Na channel is blocked?A Increase in intracellular Ca and increased contractilityB Increase in EAD and DADC Decrease in contractilityD Increase in extracellular Na7 Which one of the following is not associated with Brugada syndrome?A Mutation in SCN5A resulting in loss of functionB Increase in Ito currentC Inhibition of ICa during the plateau phaseD Mutation in SCN5A, resulting in gain of function8 W hat type of channel block, by lidocaine, results in effective suppression ofarrhythmias during myocardial ischemia?A Inactivated state blockB Resting state blockC Open state blockD Closed state block9 W hich one of the following agents is likely to be effective in treating flecainideinduced VT?A IV magnesiumB IV lidocaineC IV amiodaroneD IV digoxin
Ions channels and currents 510 W hich one of the following metabolic abnormalities is likely to decrease lidocaine dissociation from the channel sites?A AcidosisB IschemiaC HyperkalemiaD Hyponatremia11 W hat electrophysiologic manifestations can be expected when INab (the slowcomponent of the background Na current) is blocked?A Lengthening of the QT intervalB Positive inotropyC Occurrence of EADD Bradycardia12 W hich one of the following interventions is likely to promote occurrence ofTDP in patients with LQT3?A Beta blocker induced bradycardiaB Permanent pacemakerC MexiletineD Exercise-induced sinus tachycardia1.3 Calcium channels and currents1 I n which one of the following electrical activities there is no contribution fromcalcium current ICaL?A EADB Electrical remodeling of the atrium during AFC DADD Depolarization of the SA and AV nodes2 Which of the following statements is incorrect?A β-Adrenergic agonists increase ICaL channel activityB Beta-blockers act as Ca channel blockersC Parasympathetic stimulation decreases ICaL activityD T-type Ca channel density is increased by growth hormone, endothelin,and pressure overload3 Which of the following agents has no effect on T-type Ca channel?A AmilorideB FlunarizineC MibefradilD Digoxin4 W hich one of the following statements regarding calcium homeostasis incardiac myocyte is incorrect?A Ca2 -ATPase contributes substantially to diastolic Ca2 removal from cardiacmyocyte.
6 Essential Cardiac ElectrophysiologyB Ca2 in SR lumen is bound to the low-affinity calcium-binding proteincalsequestrinC Ca2 signal is generated by Ca2 influx through voltage-dependent L-typecalcium channels.D Sarcoplasmic reticulum is the major reservoir of the calcium.5 Which one of the following agents increases sensitization to RyR2?A TetracaineB RapamycinC CaffeineD Doxorubicin6 Which one of the following statement about ivabradine is incorrect?A It produces bradycardiaB cAMP overload will nullify its effectC It produces visual signs and symptomsD It has negative inotropic effect.
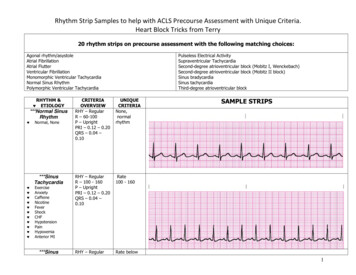
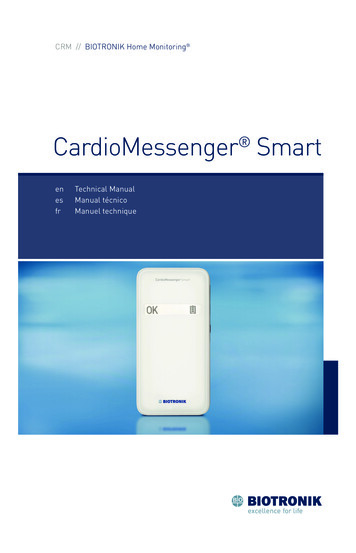
Ions channels and currents 71.1 Potassium channels/currents1,2 There are more than eight types of potassium currents. Plateau phase of the action potential depends on the balance between inward(depolarizing) and outward (repolarizing) currents. Potassium currents (outward movement of the K through the potassiumchannels) are the main contributors to repolarization Activity of potassium channel could be either time-dependent or voltagedependent (KV). Voltage-gated potassium (KV) channels consist of a tetrameric assembly of αsubunits (Figure 1.1). Each α subunit contains six membrane-spanning segments, S1 to S6, with both amino (N) and carboxyl (C) termini located on theintracellular side of the membrane. Segments S1 to S4 confer voltage-sensing properties to these channels,whereas S5 and S6 are critical for forming the channel. KV channels fluctuate between open conducting (activated) state(s) and nonconducting state(s), with the kinetics of the transitions depending criticallyon membrane voltage and channel structure. Nonconducting states can be classified as either closed (deactivated) or inactivated states. During the course of an action potential, closed KV channels activate or openin response to membrane depolarization and subsequently enter the inactivated state in a time-dependent manner. Re-entry into the closed staterequires membrane repolarization. The voltage- and time-dependent transition between these different conformational functional states is called gating. Potassium channels catalyze selective transport of K ions across lipid bilayerswhile remaining impermeable to other biologic cations. AP duration determines amount of calcium influx and tissue refractoriness. Itis inversely related to heart rate. Prolongation of AP plateau increases thestrength and duration of contraction. It also increases refractoriness. In congestive heart failure and in left ventricular hypertrophy repolarizingoutward currents are reduced by 50%. This increases APD and results in EADand arrhythmias. Use of class III drugs in patients with CHF needs reevaluation as intended target (K channels) is down regulated or absent. In atrial fibrillation repolarizing outward currents (IK, Ito) are reduced.Reduction of these currents may exacerbate arrhythmic effect of hypokalemiaand hypomagnesemia. Potassium channel expression is decreased in hypothyroid and hypoadrenalstates.Delayed and inwardly rectifying voltage sensitivepotassium channels2 Rectification is a diode like property of unidirectional current flow which couldbe inward or outwards. It limits outward flow of potassium through IKr and IKsduring plateau. Delayed rectifier potassium channels have slow onset of action.
Figure 1.1 α-Subunits of cardiac ion channels. (a) α-Subunits of Na and Ca2 channels consists of fourserially linked homologous domains (DI–DIV), each containing six transmembrane segments (S1–S6).(b, c) α-Subunits of channels responsible for Ito, IKur, IKr, IKs, IK1, and If consist of one single domain with six(B) or two (C) (IK1) transmembrane segments. Four subunits (domains) co-assemble to form one functionalchannel. (Reproduced with permission.)
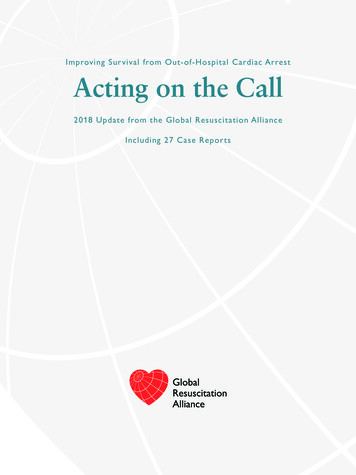
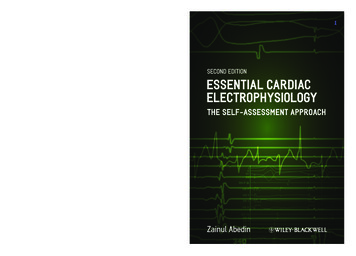
Ions channels and currents 9I toI KsI KrI KurI K1I Katp/achI KpFigure 1.2 Outward currents. Voltage gated potassium channels are activated during upstroke of AP. Rapidly activating and inactivating voltage sensitive transient outward currentIto produces phase 1 of repolarization. Inward rectifier IK1, slowly activating delayed rectifier potassium current,which includes fast inactivating rapid component IKr and slow component IKs,contributes to plateau and phase 3 of AP. K channels carry positive charge which triggers a voltage sensor. Potassium channels are closed at resting potential and open afterdepolarization. Two types of voltage-gated channels play major role in repolarization.1 Transient outward current (Ito) which is characterized by rapid activationand inactivation.2 Delayed rectifier IK which has several components (Figure 1.2)IKr is a rapidly activating current with inward rectification.IKs is a slowly activating currentIKur is an ultra rapid current.Transient outward potassium current (Ito) Ito supports early repolarization during phase 1. The transient nature of Ito issecondary to its fast activation and inactivation upon depolarization. There are two types of Ito currents. Ito1 and Ito2 A calcium-activated chloride current (Ito2) and a classical calcium- independentpotassium current (Ito1) (referred to as Ito). The calcium-independent Ito is of two types: a “rapid” or “fast” Ito,f and a slowerform, Ito,s Ito,s is smaller than Ito,f Ito,f recovers rapidly from inactivation, and its α-subunit (Kv4.3) is encoded byKCND3. Ito,slow recovers slowly from inactivation; its α-subunit (Kv1.4) isencoded by KCNA4.
10 Essential Cardiac Electrophysiology Kv4.3 and Kv1.4 contain one domain with six transmembrane segments Foursubunits co-assemble to form one channel. Kv4.3 is strongly expressed in the epicardium and is responsible for shorter APduration there compared to endocardium, where Kv1.4expression is weak. This creates a transmural voltage gradient between epicardium andendocardium. Ito,f is the primary determinant of the time course of early repolarization (phase1) of atrial and ventricular action potentials and it varies greatly betweenregions of the heart. Early repolarization modulates L-type calcium current magnitude, therebyregulating excitation-contraction coupling and myocardial contractility. Ito,f expression is greater in epicardium, right ventricle and the base of theheart, and less in the septum, left ventricular endocardium, and apex of theheart. Regional variations in Ito,f results in the heterogeneity of action potential,which are responsible for orderly ventricular repolarization. Variation in Ito,f is responsible for the regional modulation of contractility. Electrical heterogeneity associated with the transmural Ito,f gradient contributes to synchronization of repolarization and force generation across the ventricular wall. The effects of Ito,f levels on contractility are related to voltage-dependent modulation of sodium-
electrophysiologists. Packed with questions designed to aid readers’ understanding of key concepts and retention of essential facts, it is an excellent study aid for those preparing for board examination or other EP certifications. EssEntial CardiaC ElECtrophysiology thE sElf-assEssmEnt approaCh Abedin