Transcription
Disability and Rehabilitation, 2010; Early Online, 1–8RESEARCH PAPEREffects of progressive exercise during phase I cardiac rehabilitation onthe heart rate variability of patients with acute myocardial infarctionDisabil Rehabil Downloaded from informahealthcare.com by 187.66.81.48 on 09/02/10For personal use only.MICHELE D. B. SANTOS-HISS1,3, RUTH C. MELO2, VICTOR R. NEVES1, FLÁVIO C. HISS3,ROBERTO M. M. VERZOLA4, ESTER SILVA5, AUDREY BORGHI-SILVA1,ALBERTO PORTA6, NICOLA MONTANO7 & APARECIDA MARIA CATAI11Department of Physiotherapy, Federal University of São Carlos, São Carlos, SP, Brazil, 2School of Arts, Science andHumanities, University of São Paulo, São Paulo, Brazil, 3Medical School of Ribeirão Preto, University of São Paulo, RibeirãoPreto, SP, Brazil, 4Department of Physiology, Federal University of São Carlos, São Carlos, SP, Brazil, 5Faculty of HealthScience, Methodist University of Piracicaba, Piracicaba, SP, Brazil, 6Department of Technologies for Health, University ofMilan, Galeazzi Orthopaedic Institute, Milan, Italy, and 7Department of Clinical Sciences, University of Milan, InternalMedicine II, L. Sacco Hospital, Milan, ItalyAccepted August 2010AbstractPurpose. Heart rate variability (HRV) decreases after an acute myocardial infarction (AMI) due to changes in cardiacautonomic balance. The purpose of the present study, therefore, was to evaluate the effects of a progressive exercise protocolused in phase I cardiac rehabilitation on the HRV of patients with post-AMI.Material and methods. Thirty-seven patients who had been admitted to hospital with their first non-complicated AMI werestudied. The treated group (TG, n ¼ 21, age ¼ 52 12 years) performed a 5-day programme of progressive exercise duringphase I cardiac rehabilitation, while the control group (CG, n ¼ 16, age ¼ 54 11 years) performed only respiratoryexercises. Instantaneous heart rate (HR) and RR interval were acquired by a HR monitor (Polar1S810i). HRV was analysedby frequency domain methods. Power spectral density was expressed as normalised units (nu) at low (LF) and high (HF)frequencies, and as LF/HF.Results. After 5 days of progressive exercise, the TG showed an increase in HFnu (35.9 19.5 to 65.19 25.4) and adecrease in LFnu and LF/HF (58.9 21.4 to 32.5 24.1; 3.12 4.0 to 1.0 1.5, respectively) in the resting position(p 5 0.05). No changes were observed in the CG.Conclusions. A progressive physiotherapeutic exercise programme carried out during phase I cardiac rehabilitation, assupplement to clinical treatment increased vagal and decreased sympathetic cardiac modulation in patients with post-AMI.Keywords: Acute myocardial infarction, cardiac rehabilitation, heart rate variabilityIntroductionAnalysis of beat-to-beat heart rate variability (HRV)provides a simple, reproducible, and non-invasivemethod for quantifying the influence of the autonomic nervous system on the heart and, consequently, for identifying the presence of autonomicimbalance [1,2]. In general, HRV is analysed by timeand frequency domain methods [2–5], which allowthe characterisation of some conditions and/ordiseases that affect cardiac autonomic control [3].It is well established that autonomic imbalanceplays an important role in the pathophysiology ofcardiovascular diseases [6]. In patients with myocardial infarction, sympathetic hyperactivity has beenshown to occur soon after the acute event [7].Therefore, these patients have low HRV, which ischaracterised by decreased cardiac vagal modulationand consequent sympathetic predominance [8–10].Because of its prognostic value, HRV has been usedin several clinical trials with coronary artery disease(CAD) patients as an index for clinical outcomeCorrespondence: Dr. Aparecida Maria Catai, Department of Physiotherapy, Federal University of São Carlos (UFSCar), Via Washington Luiz, Km 235, CP:676, São Carlos – SP, 13565-905 Brazil. E-mail: mcatai@ufscar.brISSN 0963-8288 print/ISSN 1464-5165 online ª 2010 Informa UK, Ltd.DOI: 10.3109/09638288.2010.514016
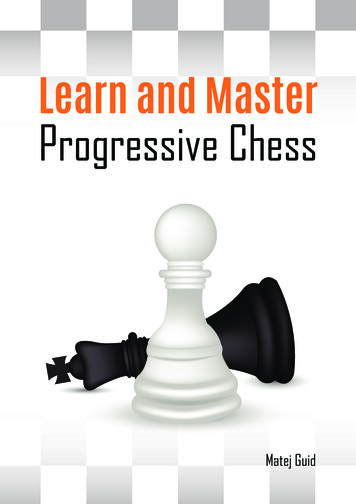
Disabil Rehabil Downloaded from informahealthcare.com by 187.66.81.48 on 09/02/10For personal use only.2M. D. B. Santos-Hiss et al.[11]. The literature has reported that reduced HRVis an important predictor for arrhythmic complications [1,2,8,9], as well as an independent mortalitypredictor associated with other post-acute myocardial infarction (AMI) risk factors (i.e., reduced ejection fraction and increased resting HR) [8–10,12].On the other hand, a recent meta-analysis showedthat HRV increases significantly in response topharmacological interventions, biobehavioural treatments and exercise training in patients with CAD[11]. Although the exercise training in phase IIoutpatient cardiac rehabilitation improves the HRVof patients with CAD [13,14] and myocardialinfarction [14,15], little is known about the effectsof progressive exercise applied during phase I cardiacrehabilitation on the cardiac autonomic modulationof patients with post-AMI. Considering that cardiopulmonary rehabilitation provides significant improvement in health outcomes, reduced hospitaladmissions and length of hospitalisation, maintenance of the patient’s functional level, and improvement in quality of life and overall risk factor controlthrough lifestyle change [16,17], it is possible thatprogressive exercise in the early phase of recoverycould bring additional benefits to patients with postAMI. Therefore, we hypothesised that progressiveexercise during phase I cardiac rehabilitation inaddition to clinical intervention might aid in therecuperation of cardiac autonomic balance in patientswith post-AMI. Thus, the purpose of the presentstudy was to evaluate the effects of phase I cardiacrehabilitation on the HRV of patients with post-AMI.MethodsSubjectsOne hundred and sixty-two patients (both genders)with AMI were admitted to the Coronary Care Unit(CCU) of a local hospital during the periodsNovember 2004 through November 2005 andSeptember 2006 through April 2007. Only fifty-nine(mean age: 53-years old) fulfilled the inclusioncriteria, i.e., having suffered their first non-complicated AMI with ST-segment elevation. The exclusion criteria were as follows: a history of previousAMI, complicated AMI, AMI without ST-segmentelevation, signs and/or symptoms of post-AMI chestpain or re-infarction, presence of diabetes mellitusassociated with cardiac autonomic dysfunction,persistence of altered pressure response (refractoryhypertension with levels greater than 180/100mmHg), atrial fibrillation, malignant ventriculararrhythmias, complex ectopic ventricular beats, supraventricular or sinus tachycardia (greater than 120beats per minute), 28 and 38 AV block; pacemakerimplantation; signs of low output or ventricularfailure, hypotension and heart failure; debility, fever,respiratory insufficiency, chronic obstructive pulmonary disease, illegal drug consumption, sequelaeof stroke, lower limb amputation, severe aorticstenosis, severe left main coronary injury (450%),prior coronary artery bypass graft surgery, inability toprogress to next protocol step and hospital entry atleast 48 h after the AMI event.Initially, 59 patients were evaluated during the firstday of hospitalisation, but only 40 were followeduntil hospital discharge. Because of noise in theelectrocardiogram (ECG) signal, three patients wereexcluded before the data analysis. Thus, a total of 37patients were studied, of which 16 belonged tocontrol group (CG, 54 11 years old) and 21 to thetreatment group (TG, 52 12 years old) (Figure 1).Among this sample, seven (19%) were submitted tothrombolyze with streptokinase (STK), 24 (65%)were submitted to primary percutaneous transluminal coronary angioplasty (PTCA) and six (16%)were treated with neither STK nor PTCA due todelayed admission to hospital (12 h after the beginning of chest pain). During hospitalisation, allpatients were submitted to cardiac catheterisation,and 34 (92%) were successfully treated with PTCA(primary or elective).ProceduresIn accordance with the Helsinki Declaration, allpatients were informed of the experimental procedures and signed an informed consent form approved by the Ethics Committee of the localinstitution (Process no. 023/2004 and no. 232/2006).Clinical evaluations were based on daily clinicaland physical examinations and laboratory tests,including: CK-MB enzyme concentration, totalblood count, clinical biochemical screening (glucose), chest X-ray, and standard ECG, as well ascardiac catheterisation.Experiments were always carried out in the afternoon. The patients were followed over 5 days,starting in the CCU (first two days) and concludingin the ward (remaining four days). The experimentalprotocol was initiated 22 5 h after CCU admissionfor both groups, as recommended by Antman et al.[18]. Both groups were daily submitted to a standardprotocol that included 10 min of rest in supineposition followed by 4 min of respiratory exercises.During the resting period, the patients were alwaysinstructed to quietly relax, breathe spontaneouslyand remain awake. The respiratory exercises weredone in the supine position and included diaphragmatic breathing pattern and deep breathing pattern.These respiratory exercises were only performed to
3Disabil Rehabil Downloaded from informahealthcare.com by 187.66.81.48 on 09/02/10For personal use only.Progressive exercise in acute myocardial infarctionFigure 1. Flow diagram accounting for sample loss.avoid possible pulmonary complication due to bedrest and hospitalisation. In addition, TG performed5 days of phase I cardiac rehabilitation that consistedof a 5-step exercise programme, progressing fromactive assisted movements on the first day after AMIto walking in the final days of hospitalisation. Thisintervention was performed and supervised by a teamof physical therapists.The progression of TG through the exerciseprotocol was based on a daily clinical evaluation ofeach patient. Walking intensity was set at 20 beatsper min above standing rest heart rate [16].Additionally, if any signs and/or symptoms appearedduring the progressive exercise training such asfatigue, chest pain, dyspnea, cyanosis, pallor, tachycardia (4120 beats per min), bradycardia, complexarrhythmias (i.e., those causing electrical and hemodynamic instability) or hypotension, the session wasinterrupted. However, none of these signs orsymptoms occurred.The instantaneous HR and RR interval wererecorded during both standard and progressive exercise protocols with a digital telemetry system consisting of a transmitter placed on the patient’s chestand a HR monitor (Polar1 S810; Polar Electro Oy,Kempele, Finland). The system detects ventricular
4M. D. B. Santos-Hiss et al.depolarisation, corresponding to the R wave on theECG, with a sampling rate of 500 Hz and a temporalresolution of 1 ms [19], and has been previouslyvalidated by Loimaala et al. [20]. After recording, thesignals were transmitted to a receiver and interfaceconnected to a computer for subsequent analysis.Additionally, blood pressure (BP) was measuredeach day by the auscultatory method before, duringand after the standard and progressive exerciseprotocols. The medication dosage was noted dailyand was not changed during the investigation inorder to prevent any influence on the variablesstudied.ResultsIn each group studied, the autonomic heart ratemodulation of patients with post-AMI was similarwhen divided by gender (male and female), ejectionfraction (preserved and reduced), AMI topography(anterior and posterior) and clinical interventionreceived (with STK, without STK and with primaryPTCA). Data were, therefore, pooled according toeach condition (control or treatment). The patients’characteristics are presented in Table I. No differenceswere found between CG and TG for these variables.MedicationsDisabil Rehabil Downloaded from informahealthcare.com by 187.66.81.48 on 09/02/10For personal use only.Heart rate variabilityHR and RR interval data were obtained on the first(T0) and the sixth day of hospitalisation (T5) (i.e.,after five days of progressive exercise training) duringa 10-min period while subjects were in the restingsupine position. Frequency domain analysis of HRVwas performed with an autoregressive algorithm[21,22], which was applied to stable 256 RR intervalseries. The power spectral density was calculated foreach RR series. Three spectral components wereobtained: very low frequency (VLF), from 0 to0.03 Hz; low frequency (LF), from 0.03 to 0.15 Hz;and high (HF), from 0.15 to 0.4 Hz. The spectralcomponents were expressed in absolute (ms2) andnormalised units and as low/high frequency ratio(LF/HF). Normalisation was computed by dividingthe absolute power of a given spectral component(low or high frequency component) by the totalpower minus the power of the component, with afrequency range between 0 and 0.03 Hz (very lowfrequency), and then multiplying this ratio by 100[21,22].Statistical analysisData are reported as mean SE. Subject characteristics, medication dosages, HR, SBP, DBP andresting HRV indices at baseline (T0 ¼ 1st day) werecompared between groups using the t-test forindependent samples. After that, the effect of time(T0 compared with T5 ¼ 6th day), group (controlcompared with treated) and the interaction betweentime and group effects were evaluated by two-wayANOVA for repeated measures. When an interactionbetween time and group effects was found, theStudent–Newman–Keuls Method was performed.Finally, intragroup analysis was performed usingthe paired t-test. These statistical analyses werecarried out using Sigma Stat for Windows, version2.03. The level of significance was set at p 5 0.05.All administered medications were recommended inthe ACC/AHA Guidelines [18] and the dosage ofthose that could affect HRV (b-blockers andangiotensin-converting enzyme-ACE inhibitors)was unchanged from the first (T0) to the sixth dayof hospitalisation (T5) for both groups.Heart rate, blood pressure, respiratory frequency, meanR–R and varianceIn both groups, resting HR and systolic bloodpressure (SBP) were high and mean R–R was lowerTable I. Patient characteristics.CharacteristicsGender (male/female)Age (years)Weight (kg)Height (cm)BMI (kg/m2)Control group(n ¼ 16)13/354 1173 15165 727 5Treatment group(n ¼ 21)17/452 1272 12168 726 3Coronary heart disease risk factorsSmoking11 (69%)Hypertension8 (50%)Family history of CAD9 (56%)Diabetes mellitus1 (6%)Overweight and obesity10 (62%)Hyperlipidaemia13 (81%)Sedentary7 (44%)Stress12 (75%)138531191014Infarction topographyAnteriorInferior14 (67%)7 (33%)MedicationsB-blockersACE grel8 (50%)8 (67%)(95%)(90%)BMI, body mass index; CAD, coronary artery disease; ACE,angiotensin-converting enzyme.
5Progressive exercise in acute myocardial infarctionConsidering that attenuated HRV is an independentrisk marker of premature morbidity and mortalityamong patients with CAD [11], the present findingsindicate that, when applied as a supplement toclinical treatment, progressive exercise contributesa protective effect during early recovery from AMI.The imbalance in autonomic cardiac function thataccompanies an AMI can be observed up to 6months after the event [9]. This fact can beattributed to ventricular remodelling, which isdivided into two phases: early, which occurs withinhours of AMI onset, and late, which occurs 72 hafter onset. Early ventricular remodelling is characterised by infarct expansion, which results inventricular rupture or aneurism. Later remodellinginvolves the entire left ventricle (LV) and isassociated with progressive dilatation, LV architecture alteration and myocyte hypertrophy, causingincreasing wall stress and damage to contractilefunction. Disturbances in circulatory hemodynamicsactivate the sympathetic adrenergic system, whichstimulates catecholamine synthesis and activates therennin–angiotensin–aldosterone system [23]. Anincrease in afferent sympathetic activity would causereflex inhibition of vagal activity, leading to sympathetic modulation predominance on the sinus node[24]. Consequently, the structural alterations observed in post-infarction LV remodelling can causepersistently reduced HRV [23,24].Abe et al. [24], studying patients after reperfusedfirst anterior AMI, verified that an HRV index(SDNN) was independently associated with LVend-systolic volume index. These authors suggestedthat autonomic alteration consequent to post-infarction LV remodelling might result in depressed HRVon the first day than the sixth day (time effect,p 5 0.05). No additional effects (group and interaction) were observed for these variables. Diastolicblood pressure (DBP) was higher in TG than in CG(group effect, p 5 0.05), but remained within thenormal range (580 mmHg). The variance of R–Rintervals and respiratory frequency presented nosignificant effects (time, group or interaction). OnlyTG patients showed a lower SBP at discharge than ontheir first day of hospitalisation (p 5 0.05) (Table II).Disabil Rehabil Downloaded from informahealthcare.com by 187.66.81.48 on 09/02/10For personal use only.Heart rate variabilityAll HRV indices presented a time effect (p 5 0.05),suggesting that these indices changed during hospitalisation. Additionally, LFnu, HFnu and LF/HFwere influenced by an interaction between time (T0vs. T5) and group (control group vs. treated group)(p 5 0.05). Thus, the progressive exercise protocolwas able to decrease the LFnu and LF/HF ratio, aswell as increase the HFnu in TG (p 5 0.05). ForCG, however, the HRV indices remained unchanged(Table II). Intragroup changes were observed only inTG, which presented a higher HFnu and a lowerLFnu and LF/HF at discharge (day 6) than on thefirst day of hospitalisation (p 5 0.05) (Table II).DiscussionThese results demonstrate that five days of progressive exercise improves vagal modulation and decreases sympathovagal balance while in the restingsupine condition in patients with post-AMI.Table II. Cardiovascular and respiratory variables with heart rate variability data during resting supine condition for both groups studied.CG (n ¼ 16)T0TG (n ¼ 21)T5p ValuesT0T5TGICardio-vascular and respiratory variablesHR (bpm)71 2.062 2.0SBP (mmHg)108 3.3100 3.3DBP (mmHg)68 2.367 2.3RF (resp/min)19 3.418 2.869 1.7110 2.9*76 2.019 3.166 1.7103 2.971 2.020 2.5p ¼ 0.006p ¼ 0.029NSNSNSNSp ¼ 0.042NSNSNSNSNSTime domainMean (ms)Variance (ms2)865 0.15120 12.2981 0.14109 8.6898 0.1113 15942 0.260 4.6p ¼ 0.02NSNSNSNSNSFrequency domainLF (nu)HF (nu)LF/HF51.4 21.039.9 19.42.2 1.754.4 22.439.3 23.02.6 2.358.9 21.4*35.9 19.5*3.1 4.0*32.5 24.165.2 25.41.0 1.5p ¼ 0.012p ¼ 0.036p ¼ 0.0034NSp ¼ 0.005p ¼ 0.003p ¼ 0.002p ¼ 0.024p ¼ 0.004CG: control group; TG: treatment group; T0 ¼ control condition (1st day ); T5 ¼ after 5 days of cardiovascular physiotherapy treatment (6thday); HR: heart rate; SBP: systolic blood pressure; DBP diastolic blood pressure; RF: respiratory frequency; LF: low frequency; HF: highfrequency; nu: normalised units; ANOVA two way: T ¼ time effect (T0 vs. T5); G ¼ group effect (control group vs. treated group);I ¼ interaction between group and time effects.*t-test: significant difference T0 vs.T5 for TG.
Disabil Rehabil Downloaded from informahealthcare.com by 187.66.81.48 on 09/02/10For personal use only.6M. D. B. Santos-Hiss et al.[23,24], which can persist for weeks or months afterthe AMI [9,23]. On the other hand, some studieshave demonstrated that exercise training does notaccelerate [25,26] or may even attenuate theprogression of ventricular remodelling after AMI[27]. Although functional and structural changes inthe left ventricle were not evaluated in the presentstudy, it is unlikely that short-term exercise training,i.e., five days of progressive exercise, would be ableto
with post-AMI. Thus, the purpose of the present study was to evaluate the effects of phase I cardiac rehabilitation on the HRV of patients with post-AMI. Methods Subjects One hundred and sixty-two patients (both genders) with AMI were admitted to the Coronary Care Unit (CCU) of a local hospi