Transcription
Quality DepartmentChronic KidneyDisease GuidelineTeamTeam LeaderJennifer Reilly Lukela, MDGeneral MedicineTeam MembersR. Van Harrison, PhDMedical EducationMasahito Jimbo, MDFamily MedicineAhmad Mahallati, MDNephrologyRajiv Saran, MBBSNephrologyAnnie Z. Sy, PharmDQuality ManagementProgramInitial Release:November, 2013Interim/Minor Revision:March 2014June 2016July 2019Ambulatory ClinicalGuidelines OversightKarl T. Rew, MDR. Van Harrison, PhDLiterature search serviceTaubman Health SciencesLibraryFor more information:734-936-9771 Regents of theUniversity of MichiganThese guidelines should notbe construed as including allproper methods of care orexcluding other acceptablemethods of care reasonablydirected to obtaining the sameresults. The ultimate judgmentregarding any specific clinicalprocedure or treatment mustbe made by the physician inlight of the circumstancespresented by the patient.Guidelines for Clinical CareAmbulatoryManagement of Chronic Kidney DiseasePatient population: Adults with chronic kidney disease (CKD).Objectives: (1) Identify populations that may benefit from more systematic screening for CKD andprovide an overview of methods for screening and diagnosis. (2) Outline treatment options for patientswith CKD to decrease progression of renal deterioration and potentially decrease morbidity andmortality. (3) Highlight common co-morbid conditions such as cardiovascular disease and diabetes,emphasizing the importance of aggressive management of these conditions to potentially decreasemorbidity and mortality among patients with CKD.Key pointsBackground Despite increasing prevalence of CKD, it is often under-recognized and under-treated. [A]* Evidence for screening and management of early stage CKD is limited due to absence of largerandomized controlled trials.Definition and Staging (Tables 1 and 2) Kidney damage for 3 months, defined by structural or functional abnormalities of the kidney, withor without decreased glomerular filtration rate (GFR).Diagnosis For patients with diabetes, screen annually for microalbuminuria if not on an ACE inhibitor or ARBand for creatinine and estimated GFR [IA]. Consider screening for CKD among patients at increasedrisk, especially those with hypertension [IA] or age 55 years. [IID] Laboratory studies needed to diagnose and stage CKD include eGFR (usually calculated using theCKD-EPI equation) and urine studies for the presence or absence of albuminuria. [IC] Ultrasound imaging for structural kidney disease may be helpful in certain populations. [IID]Treatment Lifestyle modifications (dietary management, weight management, physical activity) are the initialcomponents of treatment and secondary prevention. [IA] Blockade of the renin angiotensin aldosterone system with either an angiotensin converting enzymeinhibitor (ACEI) or an angiotensin receptor blocker (ARB) is the cornerstone of treatment to preventor decrease the rate of progression to end-stage renal disease. [IA] Blood pressure control reduces renal disease progression and cardiovascular morbidity/ mortality.- Target BP 130/80 mm Hg if without hypotension risk (eg, without: orthostatic hypotension, heartfailure, older age). (SBP of 130 mm Hg ([IA] for ASCVD); DBP 80 mm Hg [IA].)- Consider a target BP of 140/90 mm Hg if risk for hypotension. Optimally manage comorbid diabetes and address cardiovascular risk factors to decrease risk forcardiovascular disease, which is the leading cause of mortality for patients with CKD. [IA] Statin orstatin/ezetimibe therapy is recommended in all CKD patients age 50 years to decrease the risk ofcardiovascular or atherosclerotic events. [IA] Monitor for other common complications of CKD including: anemia, electrolyte abnormalities,abnormal fluid balance, mineral bone disease, and malnutrition. [ID] Avoid nephrotoxic medications to prevent worsening renal function. [ID]Monitoring and Follow Up The timing and frequency of CKD monitoring and follow up depends on disease severity and risk forprogression; assess GFR and albuminuria a minimum of once per year. [ID] (table 16) For CKD stages G3b-G5, monitor labs more frequently due to increased risk for hyperkalemia. Refer CKD stage G4 or G5 (see Table 2) to nephrology for co-management and preparation for renalreplacement therapy. Consider referral at earlier stage to assist with diagnosis of underlying causeand/or treatment of common complications of CKD. [IC]* Strength of recommendation:I generally should be performed; II may be reasonable to perform; III generally should not be performed.Levels of evidence for the most significant recommendationsA randomized controlled trials; B controlled trials, no randomization; C observational studies; D opinion of expert panel1UMHS Chronic Kidney Disease Guideline, July 2019
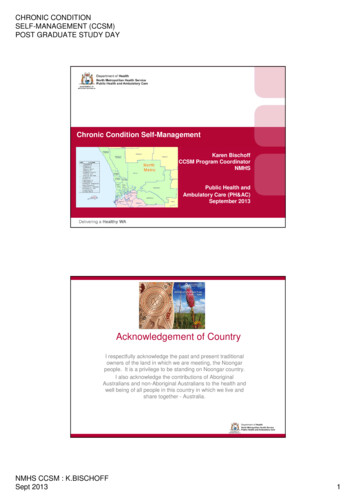
Table 1. Definition of CKDAbnormalities of kidney structure or function (definedby markers of kidney injury or decreased GFR) presentfor 3 months with implications for health. (Eithercriterion is sufficient for diagnosis.)1. Markers of kidney damage (one or more): Albuminuria (AER 30 mg/24 hrs; ACR 30mg/g) Urine sediment abnormalities Electrolyte and other abnormalities due totubular disorders Abnormalities detected by histology Structural abnormalities detected by imaging History of prior kidney transplantation2. GFR 60 mL/min/1.73 m2* GFR glomerular filtration rate; AER albumin excretionrate; ACR albumin-to-creatinine ratioModified from KDOQI Clinical Practice Guidelines for theEvaluation and Management of Chronic Kidney Disease:(2013)Table 2. Staging of CKDCKD is classified by the CGA system:Cause, GFR category, Albuminuria categoryGFRCategoryG1G2G3aGFR(mL/min/1.73 m2) 9060-8945-59G3b30-44G415-29G5 15AlbuminuriaAERCategory(mg/24hrs)A1 30A230-300A3 300TermsNormal or highMildly decreasedMildly to moderatelydecreasedModerately to severelydecreasedSeverely decreasedKidney failureACRTerms(mg/g) 30Normal tomildly increased30-300Moderatelyincreased 300SeverelyincreasedAER albumin excretion rateACR albumin-to-creatinine ratioTable 3. Common Risk Factors for theDevelopment of CKDDiabetesHypertensionAge 55 yearsFamily history of kidney diseaseObesity or metabolic syndromeTable 4. Common Causes of Acute or Acuteon Chronic Kidney InjuryVolume depletionAcute urinary obstructionUse of diuretics, ACE or ARBUse of NSAIDs, iodinated contrast agents, or othernephrotoxic agentsHeart failureAcute glomerulonephritis or acute intestinal nephritisLiver failureMalignancy (eg, myeloma)Table 5. Key Aspects of the Medical Historyin Evaluating Patients with CKDTable 6. Commonly Used Equationsto Estimate Glomerular Filtration Rate (eGFR)Prior kidney disease or dialysisIncidental albuminuria or hematuria (microscopic orgross) in the pastUrinary symptoms such as nocturia, frequency, polyuria,urgency, hesitancy; a history of foamy or frothy urinemay indicate prior heavy proteinuriaHistory of nephrolithiasisFamily history of kidney diseaseDiseases that share risk factors with CKD: DM, HTN,CAD, PAD, heart failureSystemic diseases that might affect kidney (eg,rheumatologic diseases, especially SLE; Sjogren’s;Progressive Systemic Sclerosis)History of use of medications that might affect renalfunction: OTC (especially NSAIDs and herbalmedications) or prescription (eg, lithium, calcineurininhibitors)MDRD (Modification in Diet and Renal Disease Study) 4variable equationGFR (mL/min/1.73 m2) 186 x (SCr) -1.154 x (Age) -0.203 x (0.742 iffemale) x (1.210 if African-American)CKD-EPI (Epidemiology Collaboration) equationGFR 141 x min(SCr/κ,1)α x max(SCr/κ,1)-1.209 x 0.993Age x 1.018[if female] x 1.159 [if black]Patient weight is not required for eGFR using either equation. Results arenormalized to 1.73 m2 body surface area - BSA (accepted average adultsurface area). Equations tend to underestimate GFR if large body surfacearea (eg, obese or large, muscular) patients and overestimate GFR in smallbody surface area patients. Both equations should be used with cautionwhen assessing GFR in those with extremes of body habitus or musclemass, during pregnancy, and in the elderly.Online CKD EPI & MDRD GFR Calculator (with SI fr calculator.cfm2UMHS Chronic Kidney Disease Guideline, July 2019
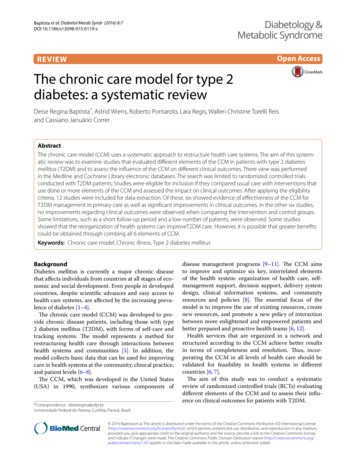
Table 7. Common Agents for Renin Angiotensin Aldosterone BlockadeGeneric(Brand) NameDosage Rangefor NormalKidneyFunctionDose Adjustments Based onGFR (mL/min/1.73 m2)Cost 30 days(Percentage of Usual Dosage)GenericBrand30-5910-29 10Angiotensin Converting Enzyme Inhibitors isinopril(Prinivil, ipril(Univasc)Perindopril(Aceon)10 - 40 mg/day(divided q12-24h)5 - 40 mg/day(divided q12-24h)25 - 50 mg 5%--75-100%50-75%50%25-50%10 - 80 mg/day(divided q12-24h)1 - 4 mg/day(divided q12-24h)7.5 - 30 mg/day(divided q12-24h)4 - 16 mg icar)Valsartan(Diovan)Telmisartan(Micardis)50 - 100 mg q24h---150 - 300 mg q24h---16 - 32 mg/day(divided q12-24h)20 - 40 mg q24h-----80 - 320 mg q24h---40 - 80 mg q24h---Eplerenone(Inspira)25 – 100 mg/day(divided 12-24h)50%Spironolactone(Aldactone)25 - 200 mg/day(divided q12-24h)-2.5 - 20 mg/day(divided q12-24h)10 - 40 mg/day(divided q12-24h)10 - 40 mg q24h50%Max dose of Max dose of2 mg q48h 2 mg q48h 5-7 28 all 14 all 50-150 73-109 150-235 7-10 193-475 9 all 33 all 6 all 48-430 9-13 156-314 11-15 33 all 28-58 38-79 20-73 62-151Can cause acute increase in SCrand/or potassium; continuemedication if increase is 30%;monitor renal function andpotassium levels with initiationand with each dosage change,every 1-2 weeks until valuesreturn to baseline (usually within4-6 weeks) 6 all 120-164 10-13 194-234 60 all 224-294n/a 238-330 13-19 254-330 18-21 233 allCan cause acute increase in SCr and/orpotassium; continue medication ifincrease is 30%; monitor renalfunction and potassium levels withinitiation and with each dosagechange, every 1-2 weeks untilvalues return to baseline (usuallywithin 4-6 weeks)Contraindicated in patients with SCr 2 mg/dL (males) or 1.8 (females)due to increased risk ofhyperkalemia; monitor potassiumlevels with initiation and with eachdosage change; extend dosinginterval or decrease dose by 50% ifnecessaryMonitor potassium levels withinitiation and with each dosagechange; extend dosing interval ordecrease dose by 50% if necessaryAngiotensin Receptor Blockers (ARBs)50%Aldosterone AntagonistsCommentsAvoidAvoid 60-107 369-73850%Avoid 6-23 82-484Cost Average Wholesale Price minus 10%. AWP from Lexicomp Online 7/19. For generic drugs, Maximum Allowable Cost plus 3 from BCBS ofMichigan MAC List, 7/19.3UMHS Chronic Kidney Disease Guideline, July 2019
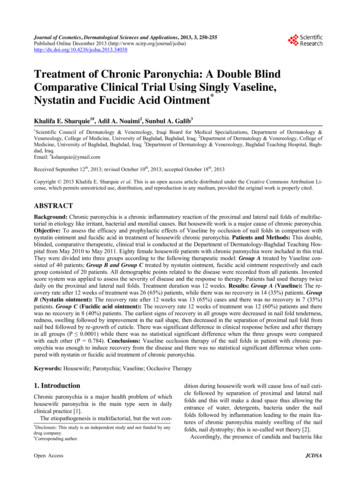
Table 8. Other Drugs Commonly Used to Treat HypertensionGeneric (Brand)NameDosage Rangefor NormalKidneyFunctionHydrochlorothiazide12.5 - 50 mg e Adjustments Based on GFR(mL/min/1.73 m2)(Percentage of Usual Dosage)30-5910-29 10Thiazide DiureticsCost 30 daysGenericBrand--Avoid2.5 - 20 mg q24h---0.5 - 1 g(divided q12-24h)--AvoidChlorthalidone15 - 50 mg q24h--Avoid 28Amiloride(Midamor)5 mg q24hAvoid 22 35Furosemide(Lasix)Torsemide(Demadex)20 - 600 mg q24h---5 - 200 mg q24h--- 5 25-36 10-26 17-164Amlodipine(Norvasc)Verapamil (Calan,Covera-HS, IsoptinSR, Verelan)5 – 10 mg q24h---80 – 120 mg q8h---Felodipine(Plendil)Diltiazem(Cardizem)5 – 10 mg q24h---IR: 30 – 90 mg q6h---CD: 180 – 360 mgq24hLA: 180 – 540 mgq24hIR: 10 mg q8h--- 12-18IR: 267XL: 500-1300CC: 61-102 7 412 6 160 5-20 81-149 35-44 2000 11-20 62-188 20-36 61-122 11-44 43-204 43 164-225Nifedipine(Procardia, Adalat)Potassium-sparing Diuretics50-100%50%Other DiureticsCalcium Channel BlockersXL: 30-120 mg q6hCC: 30-60 l tartrate(Lopressor)Propranolol(Inderal LA)Labetalol (Trandate)50 - 100 mg q24hBisoprolol (Zebeta)5 - 20 mg q24hMetoprolol succinate(Toprol XL)Nadolol (Corgard)25 - 400 mg q24h50-100%Beta Blockers50%3.125 - 25 mg q12h--Max dose 25mgq24h-100 - 450 mg/day(divided q12-24h)80 - 160 mg q24h------100 - 400 mg q12h---75%50-75%50%---40 - 80 mg q24h 6n/a 35-44 98-101 35-67n/aCommentsConsider avoidingthiazide diureticsif GFR 30 mL/min/1.73 m2;potassium-sparingdiuretics andaldosteroneblockers canincrease risk ofhyperkalemia inCKD patients 5 50-65 12-37 443 10 43-100 92IR: 78-155CD: 1000LA: 130-344Atenolol is generallynot recommendedfor BP control inCKD patientsAtenolol, andnadolol are eliminated renally;others aremetabolizedhepatically and donot need any doseadjustments due toCKD (eg,metoprolol , propranolol, labetalol)Extended dosing Extended dosingExtended dosinginterval to q36hinterval to q48hinterval to q48-60hCost Average Wholesale Price minus 10%. AWP from Lexicomp Online 7/19. For generic drugs, Maximum Allowable Cost plus 3 from BCBS ofMichigan MAC List, 7/19.4UMHS Chronic Kidney Disease Guideline, July 2019
Table 9. Drugs Commonly Used to Treat DiabetesGeneric(Brand) piride(Amaryl)Glyburide(Micronase)Dosage Rangefor NormalKidneyFunction500-1000 mg bid50%Dose Adjustments Based on GFR(mL/min/1.73 m2)(Percentage of Usual Dosage)30-5910-29 10BiguanideAvoidSulfonylureas (Second Generation)2.5-15 mg q24h50-100%50%50%1-2 mg q24h---1.25-20 mg q24h0-50%AvoidAvoid15-45 mg liptin(Nesina)--Contraindicated inpatients witheGFR 30mL/min/1.73 m2due to increasedrisk of lacticacidosis. Startingmetformin inpatients witheGFR between30-45mL/min/1.73 m2is notrecommended.Assess risk vs.benefit ofcontinuingmetformin ifeGFR dropsbelow 45mL/min/1.73 m2 11-13Active metabolitecan accumulateand causeprolongedhypoglycemia inpatients withCKD 27-150 7 43-70 6-26n/aCan cause doserelated edema.Contraindicatedin patients withNYHA Class IIIand IV heartfailure.-Dipeptidyl Peptidase-4 (DPP-4) Inhibitors100 mg q24h2.5-5 mg q24h5 mg q24h25 mg q24h50 mg q24h(CrCl 30 to 50)2.5mg q24h(GFR 50)-12.5 mg q24h25 mg q24h25 mg q24h2.5mg q24h2.5mg q24h--6.25 mg q24h56.25 mg q24hComments 5-7 tin(Januvia)AvoidCost 30 daysGenericBrandn/a 487n/a 454 alln/a 471 180 211May increase riskfor heart failure.Use with cautionin patients withknown risk factorsfor heart failure,including renalimpairment.May increase riskfor heart failure.Use with caution inpatients withknown risk factorsfor heart failure,including renalimpairment.UMHS Chronic Kidney Disease Guideline, July 2019
Generic(Brand) NameExenatide(Byetta)ExenatideExtended rulicity)Albiglutide(Tanzeum)Dosage Rangefor NormalKidneyFunction5 - 10 mcg bidDose Adjustments Based on GFR(mL/min/1.73 m2)(Percentage of Usual Dosage)30-5910-29 10Incretin mimetics, injectable-AvoidAvoid2 mcg once weekly-AvoidAvoid0.6-1.8 mg q24h---0.75-1.5 mg onceweekly30-50 mg onceweekly------Cost 30 daysGenericBrandn/a 330-660n/a 25n/a 110n/a 27n/a 20CommentsPost-marketingreports of acuterenal failure andworsening ofchronic renalfailure. Usecaution wheninitiating orescalating dosesin patients withrenal impairment.Monitor renalfunction closely inpatients reportingadverse GIeffects.Cost Average Wholesale Price minus 10%. AWP from Lexicomp Online 6/19. For generic drugs, Maximum Allowable Cost plus 3 from BCBS ofMichigan MAC List, 6/19.Table 10. Statin/Lipid Treatment in Patients with CKDCKD Patient PopulationTreatmentAge 50 years with eGFR 60 mL/min/1.73 m2 and no previous kidney transplant (G3a-G5)Statin or statin ezetimibe 1Age 50 years with eGFR 60 mL/min/1.73 m2 (G1-G2)StatinAge 18-49 with eGFR 60 mL/min/1.73 m (G1-G2) and either: known coronary disease(myocardial infarction or coronary revascularization), diabetes mellitus, prior ischemicstroke, or estimated 10-year incidence of coronary death or non-fatal myocardial infarction 10% 2StatinTransplant recipient (adult any age)StatinHypertriglyceridemiaTherapeutic lifestyle changes2Note: Adapted from the KDIGO Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease, 2013.1Option to add ezetemibe is based on the SHARP (Study of Heart and Renal Protection) trial.2Calculators to estimate 10-year incidence of coronary death or non-fatal myocardial infarction include: Framingham risk score,Reynold’s, SCORE, PROCAM, ASSIGN, or QRISK2.6UMHS Chronic Kidney Disease Guideline, July 2019
Table 11. Drugs Commonly Used to Treat DyslipidemiaGeneric(Brand) NameDosage Rangefor NormalKidney FunctionDose Adjustments Based on GFR(mL/min/1.73 m2)(Percentage of Usual Dosage)30-5910-29 10Cost a 30daysGenericBrandCommentsStatins bAtorvastatin(Lipitor)10 - 80 mg q 24hRosuvastatin(Crestor)5 - 40 mg q24hSimvastatin(Zocor)---Start at 5mgq24h;Max dose of10mg q24h5 - 80 mg q24h c--Pitavastatin(Livalo)2 mg q24h(1 – 4 mg q24h)Start at 1mgq24hMax dose of2mg q24hLovastatin(Mevacor)20 - 80 mg q24hPravastatin(Pravachol)10 - 80 mg q 24hFluvastatin(Lescol)Nicotinic Acid(Niaspan)- 6-8 340-484 10-11 282Use with caution in Asianpatients as drug levelscan be two fold higherthan usual.Start at 5mgq24h 6 112-261Myopathy risk highestwith simvastatin 80mg.If need more thansimvastatin 40 mg daily,switch to atorvastatin orrosuvastatin.Start at 1mgq24hMax dose of2mg q24hStart at 1mgq24hMax dose of2mg q24hn/a 251Contraindicated withcyclosporine.-50%50% 5-8 36-219Use doses over 20 mgwith caution in CKDstages G4 and G5.-Start at 10mgq24h20 - 80 mg q24h-50%50%500 - 2000 mg daily-50%25-50% 11 71-129 122 135-270Use doses over 40 mgwith caution in CKDstages G4 and G5. 20-73 167-592Absorption InhibitorsBile Acid ResinsEzetimibe(Zetia)10 mg daily--- 14 373May be used with otherantihyperlipidemic drugsGemfibrozil(Lopid)600 mg bid-75-100%50-100% 11 436May increase SCr;consider alternatetherapy if SCr 2mg/dL; more likely tocause rhabdomyolysiswhen used inconjunction with statins40 - 160 q24h25%25%Avoid 11-53 64-282Avoid use with statinsdue to increased risk aCost Average Wholesale Price minus 10%. AWP from Lexicomp Online 7/19. For generic drugs, Maximum Allowable Cost plus 3 from BCBS ofMichigan MAC List, 7/19.bThe risk of myopathy is increased when statins are coadministered with medications that inhibit their metabolism (eg, cytochrome P450enzyme inhibitors) or with other medications that have been associated with myopathy (eg, cyclosporine, danazol, niacin, fibrates).Adjust doses as needed, use statins cautiously with fibrates, and avoid coadministration with gemfibrozil if possible.cOnly patients who have been on simvastatin 80 mg for at least 12 months without evidence of myopathy should continue to be treated atthis dosage.7UMHS Chronic Kidney Disease Guideline, July 2019
Table 12. KDIGO Recommended Statin Dosing in Adults with y dose approved for general populationAny dose approved for general populationAny dose approved for general populationAny dose approved for general populationDose (mg/d) for eGFR CategoryG3a-G5 (including patientsreceiving dialysis or who have hada kidney transplant)20 a80 bnot /ezetimibeAny dose approved for general populationAny dose approved for general population cAny dose approved for general populationAny dose approved for general population4010 d4010/10 eStatinDose (mg/d) for eGFR Category G1-G2Adapted from the KDIGO Clinical Practice Guideline for Lipid Management in Chronic Kidney Disease (2013).All doses are mg/d. All statins may not be available in all countries. Lower doses than those used in major trials of statins inchronic kidney disease populations may be appropriate in Asian countries. Cyclosporine inhi
may benefit from more systematic screening for CKD and provide an overview of methods for screening and diagnosis. (2) Outline treatment options for patients with CKD to decreaseprogression of renal deterioration potentially decrease morbidity and and .