Transcription
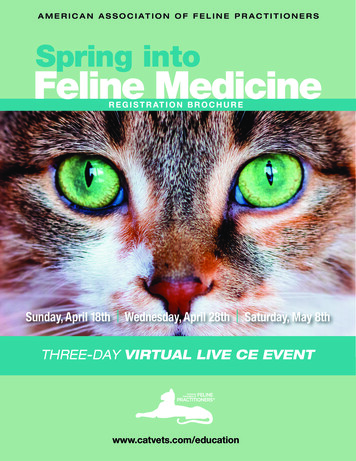
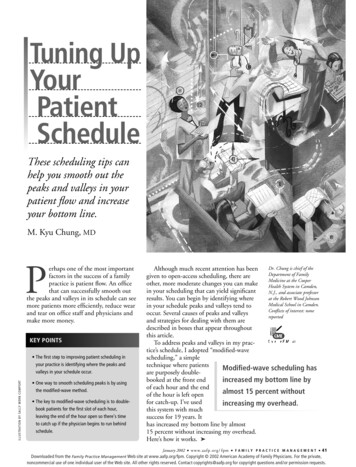
Acute and Chronic ParonychiaDIMITRIS RIGOPOULOS, MD; GEORGE LARIOS, MD, MS; and STAMATIS GREGORIOU, MDUniversity of Athens Medical School, Andreas Sygros Hospital, Athens, GreeceALEVIZOS ALEVIZOS, MD, Health Center of Vyronas, Athens, GreeceParonychia is an inflammation of the folds of tissue surrounding the nail of a toe or finger. Paronychia may be classified as either acute or chronic. The main factor associated with the development of acute paronychia is direct or indirect trauma to the cuticle or nail fold. This enablespathogens to inoculate the nail, resulting in infection. Treatment options for acute paronychiainclude warm compresses; topical antibiotics, with or without corticosteroids; oral antibiotics;or surgical incision and drainage for more severe cases. Chronic paronychia is a multifactorialinflammatory reaction of the proximal nail fold to irritants and allergens. The patient shouldavoid exposure to contact irritants; treatment of underlying inflammation and infection is recommended, using a combination of a broad-spectrum topical antifungal agent and a corticosteroid.Application of emollient lotions may be beneficial. Topical steroid creams are more effective thansystemic antifungals in the treatment of chronic paronychia. In recalcitrant chronic paronychia,en bloc excision of the proximal nail fold is an option. Alternatively, an eponychial marsupialization, with or without nail removal, may be performed. (Am Fam Physician. 2008;77(3):339-346,347-348. Copyright 2008 American Academy of Family Physicians.)This article exemplifiesthe AAFP 2008 AnnualClinical Focus on infectiousdisease: prevention, diagnosis, and management. Patient information: A handout onchronic paronychia, written by the authors of thisarticle, is provided onpage 347.Paronychia (synonymous with perionychia) is an inflammatory reaction involving the folds of tissuesurrounding a fingernail or toenail.The condition is the result of infection andmay be classified as acute or chronic. Thisarticle discusses the etiology, predisposingfactors, clinical manifestation, diagnosis, andtreatment of acute and chronic paronychia.Nail Structure and FunctionThe nail is a complex unit composed offive major modified cutaneous structures:the nail matrix, nail plate, nail bed, cuticle(eponychium), and nail folds1 (Figure 1).The cuticle is an outgrowth of the proximalfold and is situated between the skin of thedigit and the nail plate, fusing these structures together.2 This configuration providesa waterproof seal from external irritants,allergens, and pathogens.Acute ParonychiaETIOLOGY AND PREDISPOSING FACTORSThe most common cause of acute paronychia is direct or indirect trauma to thecuticle or nail fold. Such trauma may berelatively minor, resulting from ordinaryevents, such as dishwashing, an injury froma splinter or thorn, onychophagia (nail biting), biting or picking at a hangnail, fingersucking, an ingrown nail, manicure procedures (trimming or pushing back the cuticles), artificial nail application, or other nailmanipulation.3-5 Such trauma enables bacterial inoculation of the nail and subsequentinfection. The most common causativepathogen is Staphylococcus aureus, althoughStreptococcus pyogenes, Pseudomonas pyocyanea, and Proteus vulgaris can also causeparonychia.3,6,7 In patients with exposure tooral flora, other anaerobic gram-negativebacteria may also be involved. Acute paronychia can also develop as a complicationof chronic paronychia.8 Rarely, acute paronychia occurs as a manifestation of otherdisorders affecting the digits, such as pemphigus vulgaris.9CLINICAL MANIFESTATIONSIn patients with acute paronychia, only onenail is typically involved.10 The condition ischaracterized by rapid onset of erythema,edema, and discomfort or tenderness of theproximal and lateral nail folds,11 usuallytwo to five days after the trauma. Patientswith paronychia may initially present withonly superficial infection and accumulationDownloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright 2008 American Academy of Family Physicians. For the private, noncommercial use of one individual user of the Web site. All other rights reserved. Contact copyrights@aafp.org for copyright questions and/or permission requests.
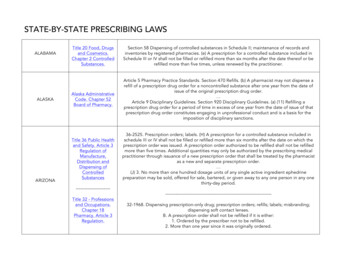
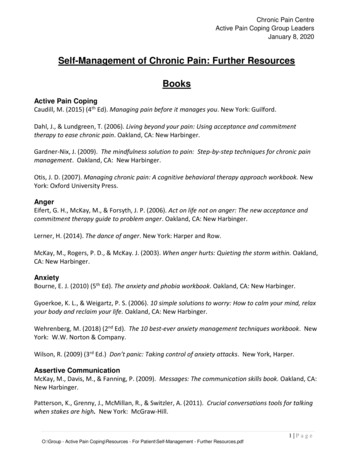
ParonychiaSORT: KEY RECOMMENDATIONS FOR PRACTICEClinical recommendationThe digital pressure test may be helpful in the early stages of paronychialinfection when there is doubt about the presence or extent of an abscess.There is no evidence that treatment with oral antibiotics is any better orworse than incision and drainage for acute paronychia.Topical steroids are more effective than systemic antifungals in thetreatment of chronic paronychia.Patients with simple chronic paronychia should be treated with a broadspectrum topical antifungal agent and should be instructed to avoidcontact irritants.EvidenceratingReferencesC14C23B21C22A consistent, good-quality patient-oriented evidence; B inconsistent or limited-quality patient-oriented evidence;C consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about theSORT evidence rating system, see http://www.aafp.org/afpsort.xml.DIAGNOSISof purulent material under the nail fold,as indicated by drainage of pus when thenail fold is compressed12,13 (Figure 2). Anuntreated infection may evolve into a subungual abscess, with pain and inflammation ofthe nail matrix.11 As a consequence, transientor permanent dystrophy of the nail platemay occur.10 Pus formation can proximallyseparate the nail from its underlying attachment, causing elevation of the nail plate.10,11Recurrent acute paronychia may evolve intochronic paronychia.7,12The diagnosis of acute paronychia is basedon a history of minor trauma and findings on physical examination of nail folds.The digital pressure test may be helpful inthe early stages of infection when there isdoubt about the presence or extent of anabscess.14 The test is performed by havingthe patient oppose the thumb and affectedfinger, thereby applying light pressure tothe distal volar aspect of the affected digit.The increase in pressure within the nail foldCross-sectionDorsal viewLateral nail grooveDistal edge ofnail plateLateral nail foldLateral nail foldsDistal phalanxLunulaNail plateCuticle(eponychium)EpidermisProximalnail foldSagittal viewNail matrixCuticle (eponychium)Nail bedNail plateHyponychiumILLUSTRATION BY dave klemmEpidermisCollagen fibersDistal phalanxFigure 1. Anatomy of the nail.340 American Family Physicianwww.aafp.org/afpVolume 77, Number 3 February 1, 2008
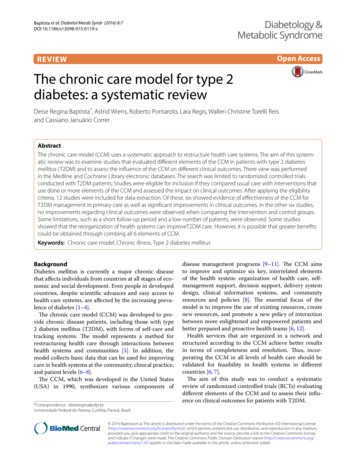
ParonychiaMEDICAL TREATMENTFigure 2. Acute paronychia with accumulationof purulent material under the lateral nailfold.(particularly in the abscess cavity) causesblanching of the overlying skin and cleardemarcation of the abscess. In patientswith severe infection or abscess, a specimenshould be obtained to identify the responsible pathogen and to rule out methicillinresistant S. aureus (MRSA) infection.13DIFFERENTIAL DIAGNOSISPsoriasis and Reiter syndrome may alsoinvolve the proximal nail fold and canmimic acute paronychia.10 Recurrent acuteparonychia should raise suspicion for herpetic whitlow, which typically occurs inhealth care professionals as a result of topicalinoculation.12 This condition may also affectapparently healthy children after a primaryoral herpes infection. Herpetic whitlowappears as single or grouped blisters with ahoneycomb appearance close to the nail.8Diagnosis can be confirmed by Tzanck testing or viral culture. Incision and drainageis contraindicated in patients with herpeticwhitlow. Suppressive therapy with a sevento 10-day course of acyclovir 5% ointmentor cream (Zovirax) or an oral antiviral agentsuch as acyclovir, famciclovir (Famvir), orvalacyclovir (Valtrex) has been proposed,but evidence from clinical trials is lacking.15February 1, 2008 Volume 77, Number 3Treatment of acute paronychia is determinedby the degree of inflammation.12 If an abscesshas not formed, the use of warm water compresses and soaking the affected digit inBurow’s solution (i.e., aluminum acetate)10 orvinegar may be effective.5,11 Acetaminophen ora nonsteroidal anti-inflammatory drug shouldbe considered for symptomatic relief. Mildcases may be treated with an antibiotic cream(e.g., mupirocin [Bactroban], gentamicin, bacitracin/neomycin/polymyxin B [Neosporin])alone or in combination with a topical corticosteroid. The combination of topical antibiotic and corticosteroid such as betamethasone(Diprolene) is safe and effective for treatmentof uncomplicated acute bacterial paronychiaand seems to offer advantages compared withtopical antibiotics alone.7For persistent lesions, oral antistaphylococcal antibiotic therapy should be used inconjunction with warm soaks.11,16,17 Patientswith exposure to oral flora via finger suckingor hangnail biting should be treated againstanaerobes with a broad-spectrum oral antibiotic (e.g., amoxicillin/clavulanate [Augmentin], clindamycin [Cleocin]) because ofpossible S. aureus and Bacteroides resistanceto penicillin and ampicillin.3,11,17,18 Medications commonly used in the treatment ofacute paronychia are listed in Table 1.3,10-13,17-22SURGICAL TREATMENTAlthough surgical intervention for paronychia is generally recommended when anabscess is present, no studies have compared the use of oral antibiotics with incision and drainage.23 Superficial infectionscan be easily drained with a size 11 scalpelor a comedone extractor.12 Pain is quicklyrelieved after drainage.17 Another simpletechnique to drain a paronychial abscessinvolves lifting the nail fold with the tip ofa 21- or 23-gauge needle, followed immediately by passive oozing of pus from thenail bed; this technique does not requireanesthesia or daily dressing.24 If there is noclear response within two days, deep surgical incision under local anesthesia (digitalnerve block) may be needed, particularly inchildren.8,10,11 The proximal one third of thewww.aafp.org/afp American Family Physician 341
ParonychiaTable 1. Commonly Used Medications for Acute and Chronic ParonychiaDrugAntibiotics in (Cleocin)*Trimethoprim/sulfamethoxazole(TMP/SMX; Bactrim, Septra)*Antibiotics (topical)Bacitracin/neomycin/polymyxin Bointment (Neosporin)Gentamicin ointmentMupirocin ointment (Bactroban)Antifungal agents (oral)Fluconazole (Diflucan)Itraconazole (Sporanox)Nystatin (Mycostatin)200,000-unit pastillesAntifungal agents (topical)Ciclopirox topical suspension(Loprox TS)Clotrimazole cream (Lotrimin)Econazole cream (Spectazole)Ketoconazole cream (Nizoral;brand no longer available in theUnited States)Nystatin creamTypical dosageComments500 mg/125 mg orally threetimes daily for seven daysor875 mg/125 mg orally twicedaily for seven days150 to 450 mg orally three orfour times daily (not to exceed1.8 g daily) for seven days160 mg/800 mg orally twicedaily for seven daysDosage adjustment may be necessary in patients withrenal impairment; cross-sensitivity documented withcephalosporins; diarrhea may occurThree times daily for fiveto 10 daysThree or four times dailyfor five to 10 daysTwo to four times dailyfor five to 10 daysOvergrowth of nonsusceptible organisms withprolonged use—100 mg orally once dailyfor seven to 14 days200 mg orally twice dailyfor seven daysHepatotoxicity and QT prolongation may occurOne or two pastilles four timesdaily for seven to 14 daysTwice daily until clinicalresolution (one monthmaximum)Three times daily until clinicalresolution (one monthmaximum)Three or four times daily untilclinical resolution (one monthmaximum)Once or twice daily untilclinical resolution (one monthmaximum)Three times daily until clinicalresolution (one monthmaximum)Antiviral agents for herpetic whitlow200 mg orally five times dailyfor 10 days250 mg orally twice dailyFamciclovir (Famvir)†for 10 days500 mg orally twice dailyValacyclovir (Valtrex)†for 10 daysAcyclovir (Zovirax) †Adjust dosage in patients with severe hepatic dysfunction;associated with severe and possibly fatal colitis; informpatient to report severe diarrhea immediatelyHigh doses may cause bone marrow depression;discontinue therapy if significant hematologic changesoccur; caution in folate or glucose-6-phosphatedehydrogenase deficiencyAvoid contact with eyes; may irritate mucous membranes;resistance may result with prolonged useAntacids may reduce absorption; edema may occurwith coadministration of calcium channel blockers;rhabdomyolysis may occur with coadministration ofstatins; inhibition of cytochrome P450 hepatic enzymesmay cause increased levels of many drugsAdverse effects include nausea, vomiting, and diarrheaAvoid contact with eyes and mucous membranesAvoid contact with eyes; if irritation or sensitivity develops,discontinue use and begin appropriate therapyAvoid contact with eyes; if irritation or sensitivity develops,discontinue use and begin appropriate therapyAvoid contact with eyes; if irritation or sensitivity develops,discontinue use and begin appropriate therapyAvoid contact with eyes; if irritation or sensitivity develops,discontinue use and begin appropriate therapyNausea, vomiting, rash, deposition in renal tubules, andcentral nervous system symptoms may occurDosage adjustment recommended in patients with renalimpairmentAssociated with onset of hemolytic uremic syndromecontinued342 American Family Physicianwww.aafp.org/afpVolume 77, Number 3 February 1, 2008
Table 1. Commonly Used Medications for Acute and Chronic Paronychia (continued)ParonychiaDrugTypical dosageCommentsCorticosteroids (topical)Betamethasone 0.05% cream(Diprolene)Betamethasone valerate 0.1%solution or lotion (Beta-Val)Twice daily for one to twoweeksOnce or twice daily for oneto two weeksIf infection develops and is not responsive to antibiotictreatment, discontinue use until infection is controlledProlonged therapy over large body surface areas maysuppress adrenal function; if infection develops,d
01.02.2008 · acute paronychia are 3,10-13,17-22listed in Table 1. SURGICAL TREATMENT Although surgical intervention for paro-nychia is generally recommended when an abscess is