Transcription
Official Title of Study:A Randomized, Multi-center Phase III Study of Nivolumab versus Sorafenib as First-LineTreatment in Patients with Advanced Hepatocellular CarcinomaNCT Number: NCT02576509Document Date (Date in which document was last revised): July 2, 2018
STATISTICAL ANALYSIS PLANA RANDOMIZED, MULTI-CENTER PHASE III STUDY OF NIVOLUMAB VERSUSSORAFENIB AS FIRST-LINE TREATMENT IN PATIENTS WITH ADVANCEDHEPATOCELLULAR CARCINOMA(CHECKMATE 459: CHECKPOINT PATHWAY AND NIVOLUMAB CLINICAL TRIALEVALUATION 459)PROTOCOL(S) CA209459VERSION # 3.0Approved v 7.0930114510 7.0
Statistical Analysis PlanBMS-936558CA209459nivolumabTABLE OF CONTENTSSTATISTICAL ANALYSIS PLAN .1TABLE OF CONTENTS .22STUDY DESCRIPTION .112.1Study Design .112.2Treatment Assignment .122.3Blinding and Unblinding .132.4Protocol Amendments .132.5Data Monitoring Committee .142.6Blinded Radiology Review Committee .143OBJECTIVES .153.1Primary .153.2Secondary .154ENDPOINTS .164.1General Definitions of Efficacy Endpoints based on Tumor Assessment .164.1.1ORR.164.1.2PFS .164.1.3TTP .174.1.4DOR .184.1.5TTR .184.1.6DCR .184.1.7DDC .194.2Primary endpoint OS .194.3Secondary endpoints .194.3.1ORR.192Approved v 7.0930114510 7.0
Statistical Analysis PlanBMS-936558CA209459nivolumab4.3.2PFS .194.3.3PD-L1 expression .194.4.10Outcome Research .224.4.10.1EuroQoL EQ-5D-3L LE SIZE AND POWER .236STUDY PERIODS, TREATMENT REGIMENS AND POPULATIONSFOR ANALYSES .246.1Study Periods .246.2Treatment Regimens .246.3Populations for Analyses .257STATISTICAL ANALYSES .257.1General Methods .257.2Study Conduct .267.2.1Accrual .267.2.2Relevant Protocol Deviations .277.3Study Population .277.3.1Subject Disposition .277.3.2Demographics and Other Baseline Characteristics .287.3.2.1Demographics .287.3.2.2HCC Etiology.283Approved v 7.0930114510 7.0
Statistical Analysis PlanBMS-936558CA209459nivolumab7.3.2.3HCC Disease Characteristics .287.3.3Medical History and Pre-treatment Events .297.3.4Prior Anti-Cancer Therapies .297.3.5Baseline Examinations.297.3.6Discrepancies Between IVRS and CRF Stratification Factors.297.4Extent of Exposure .297.4.1Administration of Study Therapy .307.4.2Modification of Study Therapy .307.4.2.1Dose delay for nivolumab .307.4.2.2Dose delay for sorafenib .317.4.2.3Dose modifications for nivolumab .317.4.2.4Dose modifications for sorafenib.317.4.2.5Infusion interruptions and rate changes for nivolumab .317.4.3Concomitant Medications .327.5Efficacy .327.5.1Primary Efficacy Endpoint OS Analyses .327.5.1.1Primary Analysis .327.5.1.2Secondary Analyses .327.5.1.3Sensitivity Analyses .337.5.1.4Consistency of Treatment Effect on OS in Subsets .337.5.1.5Subject Follow-up .337.5.1.6Subsequent Therapy .347.5.2Secondary Efficacy Endpoint ORR Analyses .347.5.3Secondary Efficacy Endpoint PFS Analyses.357.5.4Interim Analyses and Multiple Comparison .377.5.4.1Interim Analyses .377.5.4.2Stagewise Hierarchical Testing Procedure for Primary Endpoint OS andSecondary Endpoints ORR and PFS.374Approved v 7.0930114510 7.0
Statistical Analysis PlanBMS-936558CA209459nivolumab7.6Safety .407.6.1Deaths .407.6.2Serious Adverse Events .407.6.3Adverse Events Leading to Discontinuation of Study Therapy .407.6.4Adverse Events Leading to Dose Modification .407.6.5Adverse Events .407.6.6Select Adverse Events .407.6.7Immune modulating medication .407.6.8Multiple Events .407.6.9Other Events of Special Interest .417.6.10Immune-Mediated Adverse Events .417.6.11Laboratory Parameters .417.6.12Vital Signs .417.6.13Immunogenicity Analysis .417.6.14Pregnancy .417.6.15Adverse Events By Subgroup .417.7Pharmacokinetics .417.8.1PD-L1 Expression .417.8.1.1Analyses of PD-L1 .427.9Outcome Research Analyses .447.9.1EQ-5D .447.9.2FACT-Hep.448CONVENTIONS .458.1Date Imputation .458.2Duration Calculation and Conversion .465Approved v 7.0930114510 7.0
Statistical Analysis PlanBMS-936558CA209459nivolumab8.3Decimal Places.468.4Analysis Software .469CONTENT OF REPORTS .4610DOCUMENT HISTORY .466Approved v 7.0930114510 7.0
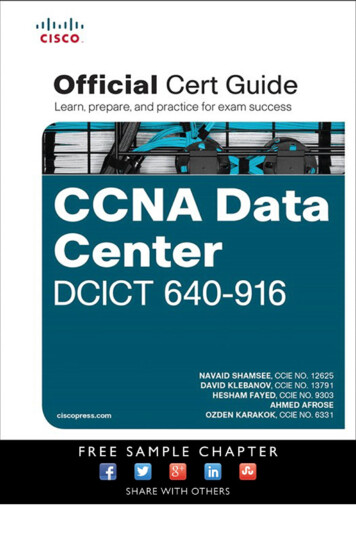
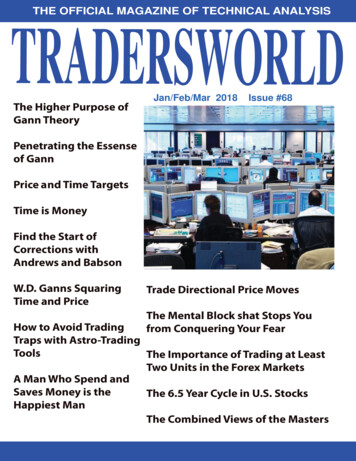
Statistical Analysis PlanBMS-936558CA209459nivolumab2STUDY DESCRIPTION2.1Study DesignThis is an open-label, two-arm, randomized, Phase 3 study in adult ( 18 years) male and femalesubjects with advanced HCC. Subjects must not be amenable for management with surgery orloco-regional therapy or have progressed after surgery or loco-regional therapy. Subjects mustnot have received prior systemic therapy for advanced HCC in keeping with the first-line settingof this study.After screening for eligibility and signing of informed consent, qualified subjects will berandomized in a 1:1 ratio to receive nivolumab or sorafenib. It is expected that approximately908 subjects will be screened for the study with approximately 726 subjects will be randomized,e.g., approximately 363 subjects will be randomized to each study arm. Randomization will bestratified by etiology (HCV vs. non-HCV [ie, HBV and HCC with no history of hepatitis virusinfection]), vascular invasion and/or extrahepatic spread (present or absent), geography (Asia vsNon-Asia).Subjects will receive open-label treatment with one of the following: Nivolumab 240 mg IV every 2 weeks until disease progression or unacceptable toxicity Sorafenib 400 mg PO BID until disease progression or unacceptable toxicityThe study design schematic is presented in Figure 2.1-1.11Approved v 7.0930114510 7.0
Statistical Analysis PlanBMS-936558Figure 2.1-1:CA209459nivolumabStudy Design SchematicOn treatment visits will occur at Day 1 and every 2 weeks thereafter. Tumor imagingassessments will occur 8 weeks from the date of randomization ( /-1 wk), then every 8 weeks( /- 1 wk) thereafter up to 48 weeks, then it will be every 12 weeks ( /- 1 week) until diseaseprogression or treatment is discontinued (whichever occurs later). Subjects will be treated untilunacceptable toxicity or disease progression. Following discontinuation of therapy, safety will beassessed through post-treatment Follow Up visit 2 ( 100 days from last dose). Survival statuswill be assessed every 3 months after follow up visits are completed, and may be completed viatelephone or in person visits.On both arms, treatment beyond initial investigator-assessed RECIST 1.1 defined progression ispermitted if the subject has investigator assessed clinical benefit and is tolerating study drug, asspecified in the protocol 31.This study’s primary endpoint is OS in all randomized subjects. Its secondary endpoints includeobjective response rate (ORR) and progression-free survival (PFS) based on tumor responseassessed by a blinded and independent central review (BICR) according to RECIST 1.1.2.2Treatment AssignmentCA209459 is a randomized, open-label study. After the subject’s initial eligibility is establishedand informed consent has been obtained, the subject must be enrolled into the study by calling aninteractive voice response system (IVRS) to obtain the subject number. Every subject that signsthe informed consent form must be assigned a subject number in IVRS. Specific instructions forusing IVRS will be provided to the investigational site in a separate document.The investigator or designee will register the subject for enrollment by following the enrollmentprocedures established by BMS. The following information is required for enrollment: Date that informed consent was obtained12Approved v 7.0930114510 7.0
Statistical Analysis PlanBMS-936558 CA209459nivolumabDate of birthGender at birthViral status at time of enrollment, if knownOnce enrolled in IVRS, enrolled subjects that have met all eligibility criteria will be ready to berandomized through IVRS. The following information is required for site entry in the IVRS priorto subject randomization: Subject numberDate of birthVascular invasion and/or extrahepatic spread (present or absent)Additional information will be automatically transferred to the IVRS by the Central Lab andmust be available prior to subject randomization: Etiology (HCV vs non-HCV) Confirmation of tumor tissue sample receipt and acceptability at Central LaboratorySubjects meeting all eligibility criteria will be randomized in a 1:1 ratio to nivolumab orsorafenib, stratified by the following factors: Etiology (HCV vs non-HCV) Vascular invasion and/or extrahepatic spread (present or absent) Geography (Asia vs Non-Asia)The randomization procedures will be carried out via permuted blocks within each stratum. Theexact procedures for using the IVRS will be detailed in the IVRS manual.2.3Blinding and UnblindingThis is an open-label study.2.4Protocol AmendmentsThis statistical analysis plan (SAP) incorporates the amendments in Table 2.4-1.Table 2.4-1:AmendmentAmendment 16Protocol AmendmentsDate of Issue15-Aug-2017Summary of Major Changes Changed ORR from a co-primary objective to asecondary objective of the study. OS is the sole primary endpoint of the study.Revised Protocol 0224-Aug-2016Incorporates Amendment 11Amendment 1124-Aug-2016 UpdatedStudyinformation Primary endpoint and objective changed from timeDirector/MedicalMonitor13Approved v 7.0930114510 7.0
Statistical Analysis PlanBMS-936558Table 2.4-1:AmendmentCA209459nivolumabProtocol AmendmentsDate of IssueSummary of Major Changesto progression (TTP) to objective response rate(ORR) Added requirement for confirmatory scan tobe performed for CR/PR assessment of bestoverall response (BOR)Management algorithms updated per revisednivolumab IBRevised Protocol 0101-Oct-2015Incorporates Amendment 02Amendment 0201-Oct-2015Addition of collection of peripheral blood mononuclearcells (PBMCs) and myeloid derived suppressor cells(MDSCs) collected from subjects at baseline fromselected sites, reduction of frequency of HCV RNAtesting for HCV infected subjects, clarification oflocoregional therapy inclusion criteria, as well as othermiscellaneous clarifications and corrections.2.5Data Monitoring CommitteeA DMC will be established to provide oversight and safety and efficacy considerations inprotocol CA209459. The DMC will provide advice to the sponsor regarding actions thecommittee deems necessary for the continuing protection of subjects enrolled in the study. TheDMC will be charged with assessing such actions in light of an acceptable benefit/risk profile fornivolumab. The DMC will act in an advisory capacity to BMS and will monitor subject safetyand evaluate the available efficacy data for the study.The BMS cl
Jul 02, 2018 · interactive voice response system (IVRS) to obtain the subject number. Every subject that signs the informed consent form must be assigned a subject number in IVRS. Specific instructions for using IVRS will be pro