Transcription
Impact of CMS Readmission Reductionand Value-Based Purchasing Programson Rural PPS HospitalsIra Moscovice, PhDMichelle Casey, MSPeiyin Hung, MSPHRural Health Research Gateway WebinarOctober 20, 2015
Acknowledgements This research was supported by the Federal Office of RuralHealth Policy (FORHP), Health Resources and ServicesAdministration (HRSA), U.S. Department of Health andHuman Services (HHS) under PHS Grant #5U1CRH03717.The information, conclusions and opinions expressed arethose of the authors and no endorsement by FORHP,HRSA, or HHS is intended or should be inferred.
Overview CMS historically paid hospitals based on volume ratherthan performance; ACA authorized efforts to realignfinancial incentives to provide high quality care The Readmissions Reduction Program reducesMedicare payments for hospitals determined to haveexcess readmissions for specific conditions The Value-Based Purchasing program raises or lowersMedicare payment rates for hospitals based on howthey score on a range of quality measures Both programs apply to Prospective Payment System(PPS) hospitals; Critical Access Hospitals are exempt
Previous Studies Studies have found that safety-net hospitalsare more likely to be penalized under theReadmission Reduction and/or VPB Programs(Gu et al, HSR, 2014; Gilman et al, HealthAffairs, 2014 and 2015; GAO, 2015) Small rural hospitals ( 100 beds) had similarmedian VBP payment adjustments to hospitalsoverall in 2013-2014, but larger bonuses andsmaller penalties in 2015 (GAO,2015)
Readmissions Reduction ProgramProgram Basics Readmission rates are based on 3 years of Medicaredata, and risk-adjusted for patient demographiccharacteristics, frailty, and comorbidities.– FY 2013 -2014: AMI, heart failure, and pneumonia– FY 2015: COPD and elective hip & knee replacement added– FY 2017: CABG surgery added Maximum Medicare payment reductions were 1% forFY 2013; 2% for FY 2014; and 3% in FY 2015 andthereafter. Payment for all Medicare inpatient admissions arereduced by this amount.
Readmissions Reduction ProgramResearch Questions How did the proportion of rural and urbanhospitals that received penalties under theReadmission Reduction Program change overtime? Which hospital and county characteristics wereassociated with a higher likelihood of receivingreadmission penalties? How did condition-specific hospital readmissionrates differ for rural and urban hospitals?
Readmissions Reduction ProgramData and MethodsData CMS hospital-level, readmission penalty data for FY2013 - FY 2015 American Hospital Association Annual Survey FY 2012 Area Health Resource File 2012 Sample: 2,471 urban and 860 rural PPS hospitalsMethods Descriptive and bivariate statistics Two-group t-tests to identify significant differences incondition-specific readmission rates between urbanand rural PPS hospitals
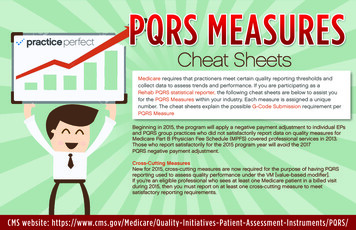
Readmissions Reduction ProgramResults: Percent of Hospitals PenalizedRural hospitalsUrban hospitals63.4%FY 201366.0%65.2%FY 201466.5%79.1%FY 201578.9%0%20%40%60%80%100%
Readmissions Reduction ProgramFY 2015 Results: Rural-Urban Differences Significant differences by hospitalorganizational and county characteristics– Size: among 50 bed hospitals, penalties morelikely for rural (70.5%) than urban (44.8%)– Ownership: among for-profit hospitals, penaltiesmore likely for rural (84.3%) than urban (73.1%)– Census Region: In NE, penalties more likely forurban hospitals than rural (89.9% vs. 81.6%); inSouth, penalties more likely for rural hospitals thanurban (85.7% vs. 79.2%)
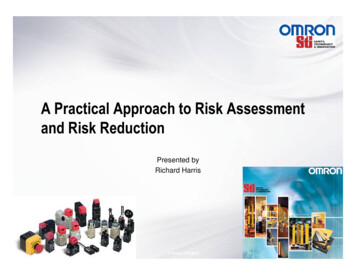
Readmissions Reduction ProgramFY 2015 Results: Hospital Size Larger rural hospitals are more likely to receivereadmission penaltiesAll Rural HospitalsN 857 50 bedsN 30950-99 bedsN 297100-299 bedsN 241300 beds79.1%70.5%84.6%83.0%N 100%90.0%20%40%60%80%100%
Readmissions Reduction ProgramFY 2015 Results: Ownership Type For-profit rural hospitals are more likely to bepenalized than other rural hospitalsAll Rural HospitalsN 85779.1%Private, not-for-profitN 44678.6%Government, non-federalN 239For-profitN 1700%20%76.2%84.3%40%60%80%100%
Readmissions Reduction ProgramFY 2015 Results: Medicare Inpatient Days Rural hospitals with a higher proportion of Medicareinpatient days more likely to receive readmission penaltiesAll Rural HospitalsN 857 13%N 22013% -18%N 19818.1% - 25%N 233 25%N 2060%20%79.1%73.2%75.8%81.8%86.9%40%60%80%100%
Readmissions Reduction ProgramFY 2015 Results: Medicaid Inpatient Days The same holds true for rural hospitals with higherproportions of Medicaid inpatient daysAll Rural HospitalsN 857 3%N 2403.01% - 5%N 1845.01% - 8%N 219 8%N 2140%20%79.1%72.5%75.0%83.6%86.5%40%60%80%100%
Readmissions Reduction ProgramFY 2015 Results: Census Region Rural hospitals: readmission penalties most likely inSouth, less likely in West57%74%86%82%
Readmissions Reduction ProgramFY 2015 Results: County Characteristics Penalties more likely for rural hospitals located in countieswith fewer primary care physicians per populationAll Rural HospitalsN 857 1:2,000 (fewer)N 3321:2,000 - 1:1,501N 25479.8%1:1,500 - 1:1,001N 20178.6% 1:1,000 (more)N 680%79.1%81.1%67.6%20%40%60%80%100%
Readmissions Reduction ProgramFY 2015 Results: County Characteristics Penalties also more likely for rural hospitals in countieswith lower median family incomeAll Rural HospitalsN 857 50,000N 493 50,000 - 59,999N 265 60,000 - 64,999N 4967.3% 65,000N 4866.7%0%79.1%82.7%76.7%20%40%60%80%100%
Readmissions Reduction ProgramFY 2015 Results: Readmission Rates byCondition Significantly lower (better) readmissionrates in urban hospitals for AMI patients Significantly lower (better) rates in ruralhospitals for patients with heart failure,pneumonia, and COPD Did not differ significantly betweenurban and rural hospitals for patientswith hip and knee replacements
Readmissions Reduction ProgramDiscussion/Implications Our study builds on previous research toshow that rural as well as urban hospitalswith fewer resources and greater needs aremore likely to incur readmission penalties Concerns about extent to which readmissionrates are influenced by factors outside thecontrol of hospitals, including socioeconomicstatus of patients
Readmissions Reduction ProgramDiscussion/Implications Additional concerns about penalty calculations– Aggregate penalties remain constant when nationalreadmission rates decline– Single-condition readmission rates face significantrandom variation due to small numbers MedPAC recommendations (July 2015):– Set a fixed target for readmission rates– Use all-condition readmission measure– Evaluate hospitals against group of peers with asimilar share of low-income Medicare beneficiaries
Value-Based Purchasing ProgramVBP Program Overview Maximum VBP bonuses and penaltiesincreased from 1% of Medicare paymentsin FY 2013 to 2% in FY 2017 VBP bonuses and penalties are based onachievement (relative to other hospitals) orimprovement (over hospital’s own baselineperformance), whichever is higher
Value-Based Purchasing ProgramCalculating VBP Performance Number of domains, quality measures withineach domain, and weight given to each domainhas changed over time Decreased emphasis on process measures Consistent focus on patient experience of care(HCAHPS) and outcome (mortality) measures Efficiency (Medicare spending per beneficiary)domain and patient safety measures addedstarting in FY 2015
VBP Scoring Domains and Weightingby Payment Fiscal YearFYFYFY2013 2014 2015FYFYFY2016 2017 2018Clinical Care: Process70%45%20%10%5%Patient Experience of Care30%30%30%25%25% 25%Clinical Care: Outcome-25%30%40%25% 25%Efficiency--20%25%25% 25%Safety----20% 25%-
Value-Based Purchasing ProgramResearch Questions Over the first three years of the program, whatproportions of rural hospitals and urbanhospitals received penalties and bonuses? How did the probability of receiving penaltiesvary as a function of hospital characteristicsand county characteristics? How did the probability of receivingbonuses/penalties change across time?
Value-Based Purchasing ProgramData Hospital Inpatient PPS final rule impact file,FY 2013 - 2015 American Hospital Association Annual Survey, FY2011-12 Area Health Resource File, 2011-13 Sample: all eligible general medical and surgicalacute care hospitals– 2,213 urban hospitals and 748 rural hospitals– Excluded 141 specialty care hospitals
Value-Based Purchasing ProgramMethods Chi-square tests examine factors associated withreceipt of bonus/penalty within a group of urban orrural hospitals Difference-in-difference models identify differentialeffects of the program on rural and urban hospitalsover time– Expected payment penalty was calculatedconditional on a hospital’s likelihood of beingpenalized in a year; likewise for expected paymentbonus.
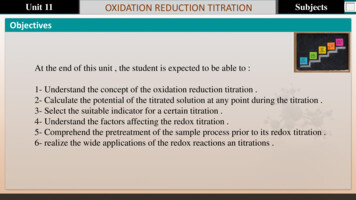
Value-Based Purchasing ProgramHospitals Receiving a Bonus or PenaltyFY 2013- FY 2015BonusPenalty49%49%FY 2013Rural (666)FY 201447%Urban (2,054)FY 201551%Urban (2,203)Urban (2,213)Rural (644)Rural (748)46%52%42%57%50%66%50%33%
Value Based Purchasing ProgramFY 2015 Bivariate Results Among rural and urban hospitals, probability of VBPpenalty significantly more likely for: Larger size Publicly owned Higher proportions of Medicare and Medicaidinpatient days Located in counties with lower median familyincome, higher uninsured rates, and fewer primarycare physicians per 1,000 county residents
Value Based Purchasing ProgramPercent of Hospitals with Penalty byCensus Region, FY 2015Urban: 50%Rural: 27%Urban: 42%Rural: 29%Urban: 48%Rural: 36%Urban: 54%Rural: 34%
Value-Based Purchasing ProgramMultivariate Analysis Which hospitals were less likely to get penalizedfor FY 2013 – 2015?– Hospital Characteristics: Rural vs. urban location, Ownership, System affiliation,Accreditation, Inpatient volume, Share of Medicare andMedicaid inpatient days, Census region– County Characteristics: Uninsured Rate among Population Age 18-64, Primary CarePhysicians per 1,000 Population
Value-Based Purchasing ProgramRural vs. Urban Location Rural hospitals had higher probability of receiving penalties forFY 2013 and 2014, but lower for FY 2015. Across the first three years, differences in expected paymentadjustments were less than 0.15%.Marginal Differences inProbability of Receiving Penaltiesbetween Rural and UrbanRural vs. UrbanHospitals2013201420152.5%**5.7%***-16.1%****p 0.05 **p 0.01 ***p 0.001
Value-Based Purchasing ProgramOther Hospital Characteristics Hospitals are more likely to be penalized if they are notaccredited or system-affiliated, have higher adjustedinpatient days, higher shares of Medicaid and Medicareinpatient days, and/or lower nurse staffing ratios.AccreditationMarginal Effects onProbability ofReceiving Penalties-5.0%*System Affiliation-4.7%**Adjusted Inpatient Days (per 1,000)0.7%***% of Medicare IPD as of Total Inpatient Days (per 10%)1.4%***% of Medicaid IPD as of Total Inpatient Days (per 10%)4.7%***Licensed Nurse Hours per Patient Day-0.7%***
Value-Based Purchasing ProgramCounty Characteristics Hospitals in counties with lower supply of primary carephysicians are more likely to get penalized No significant associations between uninsured rates andpenalty probability, but higher uninsured rates areassociated with higher expected amount of penaltiesMarginal EffectsOn Probability of Receiving PenaltiesCounty-level Uninsured Rateamong Population Age 18-64County-level Primary CarePhysicians per 1,000 Population2.04%-5.84%**
Value-Based Purchasing ProgramPayment Bonus Status: Changes OverTimeOf hospitals that received bonus in FY 2013:PenaltyBreak-EvenBonus68%64%68%75%FY 2014FY 2015FY 2014FY 2015Urban (N 1,134)Rural (N 328)
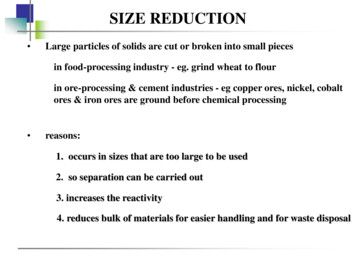
Value-Based Purchasing ProgramPayment Penalty Status: Changes OverTimeOf hospitals that received penalty in FY 2013:Penalty73%FY 201464%FY 2015Urban (N 1,046)40%Bonus82%FY 2014Break-EvenFY 2015Rural (N 326)
Value-Based Purchasing ProgramDiscussion/Implications Which hospitals are more likely to receiveVBP penalties? Hospital characteristics: non-accredited, non-systemaffiliated, public ownership, lower licensed nursestaffing per inpatient day, higher proportions ofMedicare and Medicaid inpatient days County characteristics: higher uninsured rates, lowerprimary care physician supply, lower householdincome and education level How much control do hospitals have overthese factors?
Value-Based Purchasing ProgramDiscussion/Implications VBP is budget neutral: total bonuses mustequal total penalties Which factors are responsible for ruralurban differences in the likelihood ofreceiving VBP penalties or bonuses overtime? Changing metrics or changing performance?
Readmissions Reduction and Value-Based Purchasing ProgramsDiscussion/Implications Amount of penalties may not seem large, but – Hospitals may be incurring penalties undermultiple programs: Readmissions, VBP, HospitalAcquired Condition, EHR Meaningful Use– Penalties occurring in context of overall precariousfinancial condition of many rural hospitals Average Medicare acute inpatient margin for a ruralPPS hospital was -2.6% in 2012 56 rural hospitals have closed since 2010
Additional InformationHung, Casey & Moscovice. Which Rural and Urban HospitalsHave Received Readmission Penalties Over Time? Universityof Minnesota RHRC Policy Brief, October 2015.http://bit.ly/1jTV3HiMichelle Casey: mcasey@umn.eduIra Moscovice : mosco001@umn.edurhrc.umn.edu
Maximum VBP bonuses and penalties increased from 1% of Medicare payments in FY 2013 to 2% in FY 2017 VBP bonuses and penalties are based on achievement (relative to other hospitals) or improvement (over hospital’s own baseline performance), whichever is higher . VBP