Transcription
Review sive-non-invasive-cardiology/IVC filter retrieval.M Jyotsna*, N LalitaDepartment of Cardiology, Nizam’s Institute of Medical Sciences (NIMS), Punjagutta, Hyderabad–TS IndiaAbstractIn this review article the major indications of Inferior Vena Caval (IVC) filter implantationand need for their retrievals are discussed. In addition to the routine methods of retrieval,the advanced methods are also described. Complications, precautions and various treatmentstrategies have been addressed. As this is an evolving field new advancements are expected infuture.Keywords: IVC filters, Retrieval, Pulmonary thromboembolism, Complications.Accepted on October 31, 2018IntroductionInferior Venal Caval (IVC) filters are of proven value forprevention of Pulmonary Thromboembolism (PTE) in subsetof patients with Deep Vein Thrombosis (DVT). After aninitial protection period of PTE is over and there is resolutionof DVT, the IVC filters need to be removed [1]. In literaturethe reported retrieval rates are as low as 8.5% [2]. Thedevelopment of dedicated service lines for patients with thesedevices has positively impacted retrieval rates. Minocha et al.study reporting an increase in retrieval rates from 29% to 60%after the establishment of a dedicated IVC filter service [3].Indications for IVF filter implantationOver the past 20 years there is a definite increase in theusage of IVC filters. Now it is used more frequently in DVT(prophylactic indication) than Pulmonary Thromboembolism(PTE) [4,5].12 Contraindication to anticoagulant-only therapy. Documented failure of agulation therapy).therapydespite Concurrent administration of fibrinolytic therapy. Pregnancy labor and delivery. Severe trauma to the head or spinal cord. Thrombolysis of acute ilio-caval venous thrombosis. Massive pulmonary embolism–if associated withinstability then filter implantation showed decreaseincidence of further PTE and mortality [6]. Whencombined thrombolysis and within 2 days of acuteDVT, implantation of filter in this fragile period isshown to be a better choice by Choi et al. [7]. Severe trauma to or multiple fractures of the longbones. Major pelvic or acetabular fractures iliofemoralvenous injury. Rosenthal et al. recommended bed sideimplantation IVC filters under ultrasound guidance insevere trauma patients for prevention of embolizationeven in the early stages [8]. Prolonged immobilization with multiple injuries. Prophylaxis in the setting of specific surgicalprocedures, such as malignancy resection, facial injuryrepair, or gastric bypass. Acute withdrawal of oral anticoagulants before generalsurgery. Period of transition to oral anticoagulants due toheparin-induced thrombocytopenia. Pulmonary embolus in the setting of diminishedcardiopulmonary reserve. Young patients at short-term high risk for pulmonaryembolus. Free-floating vascular thrombus on venography. Chronic thromboembolicpulmonary embolectomy). Thromboembolic disease with limited cardiopulmonaryreserve (corpulmonale). Filter complications-insertion site thrombosis.disease(undergoingTypes of filtersa. Permanent filters: In this article we are concentratingon retrieving of filters, so not much discussed aboutthese filters. If any filter related complications occursin these filter, then surgical removal is the choice ofremoval.b. Temporary filters: To overcome the disadvantages ofpermanent filters, temporary filters were introduced.These filters have an access outside as they remainattached to a wire or catheter. They can usually be leftJ Invasive Noninvasive Cardiol 2018 Volume 1 Issue 3
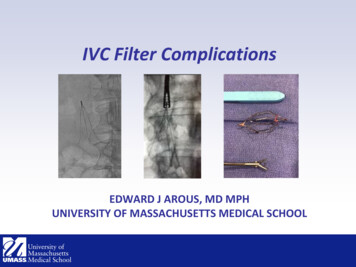
Citation: Jyotsna M, Lalita N. IVC filter retrieval. J Invasive Noninvasive Cardiol. 2018;1(3):12-19.for a week. As infection, thrombosis and migrationrate are high, filters are difficult to manage and do notserve the intented purpose properly, these filters arenot in use now.c. Retrieval filters: These filters can be retrieved oncethe need of filter coverage is over. There is changingtrends in implantation and retrievals of filters overtwo decades. In the past five years the retrieval rateswere increased from 12.0% to 17.7%. Implantationsand retrievals have been done with equal frequency byboth the cardiologists and radiologists (13.0%-13.8%)[9].Why should IVC filters be removed?IVC retrieval helps to reduce the risk associated withhaving a permanent IVC filter (a foreign body withinthe human body). The following complications can beameliorated by retrieval of the IVC filter.a. Occlusion of the filter due to thrombus is the mostfrequent complication of the filters. Incidence variesfrom 6% to 30% [10]. The filter related thrombosiswas more with first generation filters (especiallypermanent filters) [11]. The thrombosis wassignificantly decreased with the subsequently secondgeneration filters OPTEASE and GUNTHER TULIP(temporary filters) [12].b. IVC filters left in-situ for a long time have been foundto develop device-related complications such asfracture, device migration, organ penetration and IVCperforation. IVC perforation is suspected when thefilter components extend 3 mm beyond the IVC wallon CT scan [13].c. We had a case of retrieval filter implantation for massivePTE with DVT on oral anticoagulation. After twomonths, patient was admitted with acute abdominalpain and fall of hemoglobin. CT abdomen showedlarge hematoma in the wall of the large bowel alongwith peri-filter IVC hematoma. After stabilizationsurgical removal of the filter was done. Similar caseof duodenal involvement was reported [14].d. Post thrombotic syndrome.e. Patients with the anti-phospholipid syndrome-Usuallypermanent filters are used and patient requireslifelong anticoagulation in this group. But Baig et al.demonstrated that the safety of retrieval of IVC filterswith continuation of anticoagulation [15].When to remove the IVC filters?a. Normally IVC filter to be removed as soon as theunderlying indication for filter deployment was over,preferably within 30 days [16].b. For the patients who cannot take anticoagulationtemporarily, like immediate postoperative period, theimplanted IVC filter should be removed once patientbecomes eligible to take anticoagulation.c. When IVC filter implantation was done for prophylacticreasons like immobilization, then filter to be oncepatient is ambulated.d. Special attention should be paid to prophylactic filtersplaced in trauma patients, a situation in which thefilter can typically be removed within a relativelyshort time interval as patients begin to ambulate or aretransitioned to anticoagulation [17].In earlier studies it was thought that prolonged dwelltime after IVC filter implantation is predictor for failure ofretrieval. Eventually with the development of different filterspecific retrieval devices, even in the longer dwell time cases,filters could be are successfully revived [18-21]. In general,patients of retrieval IVC filters should be followed regularlyand all attempts should be made to remove the filter once thecrisis period of implanted is tide over [22]. An Informaticsapproach to facilitate tracking the patient has been proposedby Juluru K [23].Conditions where advanced retrival techniques arerequireda. Embedded hookb. Severe tiltc. Filter strut penetration into the caval walld. Prolonged dwelling timee. Advanced agef. Filter head positiong. Filter designMethods of IVC filter removal- percutaneousRoute of removalConical shape filters like GUNTHER TULIP (WILLIAMCOOK EUROPE APS) are to be removed from internaljugular approach only. Polyhedron designed filters likeOPTEASE to be removed from the femoral route. Helicaldesigned filters like Crux can be removed in both routes.Usually internal jugular approach is preferred over femoralapproach for implantation of IVC filters as filter tilt and filtertip abutment is better, but Choi disproved that. In additionthey showed that the femoral route takes less fluoscopic time[24].Simple retrieval-routine techniqueIt is always advisable to have a contrast venogram to ruleout the presence of thrombus in addition to previous noninvasive tests to see for IVC or filter thrombus (Figure 1). Wecan use usual snares or separate retrieval kits provided by thecompanies to remove the filters.The essential steps in removal are:J Invasive Noninvasive Cardiol 2018 Volume 1 Issue 313
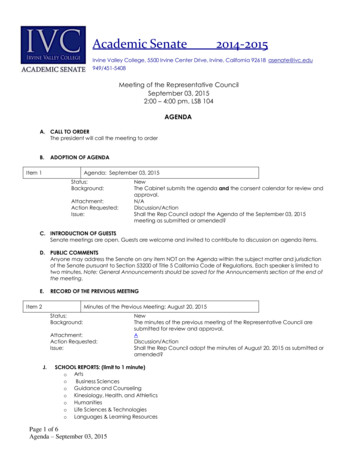
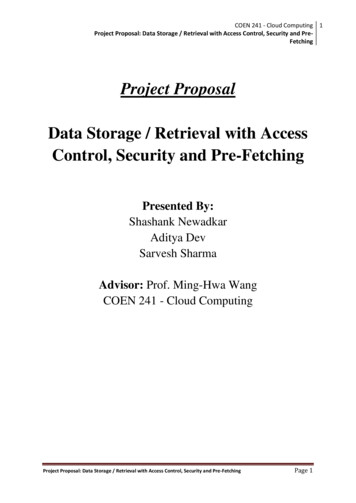
Jyotsna/LalitaPTCA wireFigure 2. In house devices for IVC filter retrieval.Figure 1. First step in IVC filter retrival - Contrast venogram – Nothrombus.i. Hold the hook with snare. Usually the filter collapses ifdwell time is shorter. If not sheath manipulations are requiredfor the retrieval.ii. A sheath to facilitate coaxial collapse of the filter anddisengagement from the caval wall. Pushing the sheath overthe filter with simultaneous pull on the filter to be done.iii. Once the filter partially enters into the sheath care to betaken not to release the pull on the snare. A constant pullingforce on the filter is required till the whole of collapsed filterenters into the sheath.Complex retrieval-modification in the retrievalprocedureA complex retrieval was defined as one requiring morethan standard sheath and snare technique [25].i.Loop or sling technique: Snares can be used tohold the filter hook and retrieve the filter. To hold the filterhook instead of snare, we can use the peripheral 0.35 incheswire (called as Stiff Wire-Displacement Technique) or evencoronary wire also can be used. (Figure 2). In the casecoronary wire loop more sheath push on the filter is requiredto separate the filter from the IVC wall. Pull on the hook ofthe filter by coronary wire may not generate sufficient forcefor IVC collapse, on other hand may distort or break the wire[26].Attention: If your catheter looks as if it is in IVC, but snaredose not reach the filter tip means catheter is a branch thanin proper IVC lumen. Then check with contrast in separateviews and reposition the sheath (Figure 3).ii. Balloon displacement: With snare to hold the hook,a peripheral balloon is passed between the filter andIVC wall to dislodge the filter.Figure 3. Diagrams showing the improper position of sheath whileretiving the filter.iii. Dissection technique (Endomyocardial/Endobronchialforceps dissection techniques): These instruments areused to hold the hook.iv. Hangman technique: This is a modified loop snaretechnique. In this a 5-F reverse curve catheter (ex: SOSOmni Catheter from AngioDynamics) and Glidewire(like Terumo wire from Radifocus are used to create awire loop between the filter neck and IVC wall (hencethe name “Hangman”), as opposed to between thefilter legs. This method is more suitable when there issevere tilt or embedded hook [27].J Invasive Noninvasive Cardiol 2018 Volume 1 Issue 314
Citation: Jyotsna M, Lalita N. IVC filter retrieval. J Invasive Noninvasive Cardiol. 2018;1(3):12-19.v. Telescoping sheaths to increase longitudinal rigidityand prevent buckling as the sheath is passed over thefilter.vi. Realignment Technique: Shaped guide catheter toengage tilted hook.vii. Dual-Access Technique: The stiff wire was insertedthrough the femoral or jugular approach between thefilter apex and the IVC wall, and snared from thealternate approach. Wire traction is simultaneouslyapplied in caudal and cephalic directions.A cautionary note: The through-and-through wire shouldbe protected by long covering sheaths or catheters to prevententry or pelvic vein lacerations during this maneuver (i.e.,‘‘cheese-slicing’’). This approach can release the filter apexfrom the IVC wall. The snare inserted through the directionof retrieval, is used to remove the repositioned filter.viii. Sandwich Technique (Parallel Wire and Dual-SheathTechnique): The recalcitrant filter is freed or untilted betweenthe two sheaths as sandwich. In this technique, the guidewires are passed through a guiding catheter along either sideof the filter nose. These wires are snared and exteriorizedthrough the opposing sheaths. The catheter and sheath arecontact into the snug against the filter, and then the upward ordownward force is applied into the filter. Single wire is usedfor this technique but we recommend the use of parallel wiresfor the better encapsulate of filter. The parallel wire techniquealso minimizes the filter disassembly during traction. Theretrieval sheath is used to remove the disengaged filter. Avariation of this technique was described by Owens et al [27].ix. Robotic assisted IVC filter retrieval: In this, a 90 cm9F robotic sheath is advanced into the IVC with theMagellan Robotic System. The CloverSnare 4-LoopVascular Retriever (Cook Medical) is to be advancedthrough the robotic sheath to capture the hook andretrieve the filter [4]. The system’s sterability andflexibility allow for greater control in narrow vessellumens and complex situations.x. Excimer Laser Assisted IVC Filter Retrieval: The excimerlaser is used to separate the filter from IVC wall.Causes of failure of routine method for retrievalThe reasons and some of the suggested modifications forthe routine IVC filter retrival failure are:i. Filter tilt: curved inner catheters/sheaths like Flexorsheath with Ansel 2 modification can be used to directthe catheter tip towards the hook [1].ii. Encasement of the filter hook in the IVC wall by a fibrincap: above mentioned advanced retival techniquesmay be useful.iii. Incorporation of filter elements into the caval wall:Hangmen technique or robotic assited or excimerlaser assisted methods may be helpful.iv. Significant extra-caval perforation of filter elements:Surgical removal is betterv. Filter fracture: Try to remove percutaneously, if failedthe removal by surgical route.vi. Significant filter thrombus: not to plan the removal atthat time, better to treat the thrombus first.vii. Caval occlusion: Is controversial where to remove orleave the filter.Recent study done by Kleedehn et al. showed that the filterhook orientation did not correlate with retrieval complexity.Filter insertion vein did not correlate with filter tilt. Filter tiltand hook apposition to the caval wall at the time of retrievalcorrelated with retrieval procedure complexity [25]. Furtherwith COLLECT AND DENALI filters, the tilt rate is furtherlow [28]. According to Gotra et al and Geisbüsch, the shorterdwell time, lower mean tilt, caudal migration and less cavalwall penetration are positive predictors of successful IVCfilter retrieval [29,30].Surgical approachOpen surgical approach requires laparotomy and venalreconstruction.ComplicationsEven though IVC filter retrieval can be performed as a daycare procedure safely, some complications may occur withthis procedure [31]. The complication rate varies dependingon the type of retrieval and varies from 0.4% in routine to5.3% with advanced technique [18].i. IVC dissectionii. IVC intussusceptioniii. IVC thrombus/stenosisiv. Filter fracture with embedded strutv. IVC injury with haemorrhage [32]. If haemorrhageoccurs then prolonged balloon tamponade mayprevent urgent surgery. But the chances of thrombosisand stenosis are there if prolonged balloon inflationis done, so it is advisable to follow these patientssubsequently [33].vi. Vascular injury from complicated venous accessvii. Other complications related to a filter changingposition after the original placementControversies in retrievalAs a rule all filters to be removed once the indication is lost,but controversy is when there is chronic total occlusion of IVCfilters. Acute IVC occlusion is usually symptomatic and requiredtreatment with thrombolysis, but chronic occlusions are not [34].Imaging modalities1. Pre-retrieval CT: CT scan as a routine procedure isJ Invasive Noninvasive Cardiol 2018 Volume 1 Issue 315
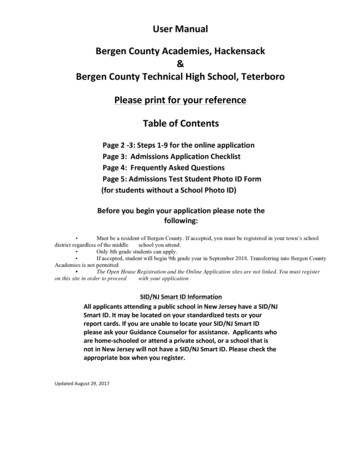
Jyotsna/Lalitanot required for retrieval. But CT abdomen is usefulwhen dwell time of filter is 180 days or plain X-rayabdomen shows severe tilting or gross displacement orpatient has suspicion of bleed due to filter penetration[35].The figure given below to show the flowchart of IVC filterretrieval (Figure 4).2. Intavascular Ultrasound (IVUS): IVUS, a specializedultrasound technique has a major role in IVC imagingespecially during endovascular procedures. It detectsintraluminal thrombus, degree of stenosis andextrinsic structures of vein and it also detects evenfibrous bands, webs or trabeculations in recanalizedveins which are not well visualized [36].3. Magnetic Resonance Venography (MRV): MRV isa diagnostic technique which is used to detect IVCthrombus and also post therapy follow up imaging.Contrast and non-contrast are the types of MRV,detect the lumen size of vein, overall extent ofthrombus, anatomical and pathological variants. Theadvantages are high accuracy central veins imagingwithout operator dependence and lack of radiation(non-contrast) [37].StudiesFor IVC filter implantation even though multiple studiesare there, the two important studies are PREPIC 1 and 2.The results of PREPIC 1 and PREPIC 2 do not providejustification for routine placement of IVC FILTER in patientswith PTE [38-40].There are few studies on IVC retrieval:i. Excimer laser assisted IVC filter retrieval study byRobert Lewandowski is recuiting the cases. Althoughthe technical failures are rare, these are due toexcessive endo-luminal scarring at the point of IVCfilter implantation. Advanced removal techniques areoften employed in difficult cases. The excimer lasersheath has been successfully used at North-western forpatients who had failed all other retrieval techniques[41].ii. Failed retrieval of Inferior Vena Cava (IVC) Filters:Long-Term Outcomes–by Lyon et al. Multiinstitutional registry results showed retrieval of theCelect filter was performed safely as long as 466 daysafter implantation. Out 95 implantation patients filterretrieval was attempted in 58 patients successfullyretrieved in 56 filters (96.6%). Unsuccessful retrievalattempts were attributed to filter tilt or excessive tissueFigure 4. Flow chart of removal of IVC retrieval.J Invasive Noninvasive Cardiol 2018 Volume 1 Issue 316
Citation: Jyotsna M, Lalita N. IVC filter retrieval. J Invasive Noninvasive Cardiol. 2018;1(3):12-19.growth with the hook embedded in the endothelium inone [42].iii. Study of IVC filter retrieval with the Günther TulipVena Cava Filter: Smouse et al. filter retrieval wasattempted in 275 patients and successful in 248(90.2%). The mean filter indwell time was 58.9 daysof implanted 554 patients. Study demonstrated reliableretrieval rates at 12 weeks, with successful retrievalsup to 17 months after implantation [43].iv. Prospective, multi-center, Single-arm study to assessthe safety of retrieval of the recovery G2 Filter(EVEREST): 100 Patients were enrolled consecutivelybetween December 2005 and July 2006. Retrievalwas attempted in 61 patients. Fifty-eight of the 61filters (95%) were successfully retrieved. Retrievalof the recovery G2 filter was safe and successful inmost patients. Caudal migration was observed as anunexpected phenomenon. [44]v. Retrieval rates in the United States: In this study byAhmed et al. [45] showed that the filter placementvolume declining from 61,889 in 2012 to 38,095 in2016. Filter retrievals however, increased from 4,327in 2012 to 8,405 in 2016. The net filter retrieval rateper annual filters placed increased from 6.9% in 2012to 22.1% in 2016, yielding an average filter retrievalrate and compound annual growth rate of 11.6% and18.1%, respectively.vi. Analysis of the final DENALI trial data: Stavropouloset al. in this study showed that in 200 patients DenaliIVC filter was implanted and filter placement wastechnically successful in 199 patients (99.5%). Filterswere clinically successful in 190 patients (95%). Therate of PE was 3%. Filter retrieval was attempted 125times in 124 patients and was technically successful in121 patients (97.6%) [46].vii. The RETRIEVE trial by Smouse et al.: A total of 125patients was implanted with the Crux filter betweenJune 2010 and June 2011 for fol
generation filters OPTEASE and GUNTHER TULIP (temporary filters) [12]. b. IVC filters left in-situ for a long time have been found to develop device-related complications such as fracture, device migration, organ penetration and IVC perforation. IVC perforation is suspected when the filter