Transcription
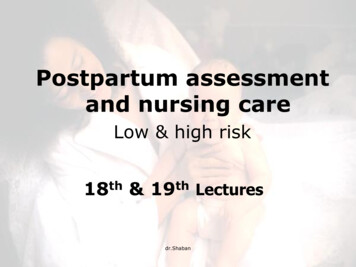
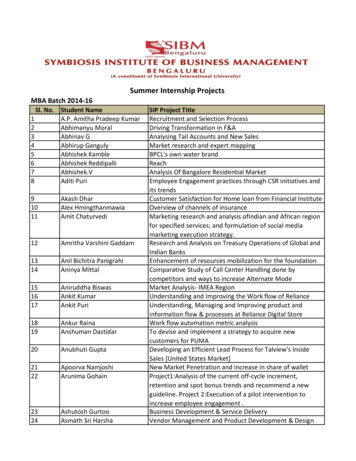
ISSUE BRIEFAugust 2019Improving Postpartum Care: State Projects Conducted through the PostpartumCare Action Learning Series and Adult Medicaid Quality Grant ProgramIntroductionThe postpartum visit provides an opportunity to assesswomen’s physical recovery from pregnancy andchildbirth, and to address chronic health conditions (suchas diabetes or hypertension), mental health status(including postpartum depression), and family planning(including contraception and pre-pregnancy counseling).The visit is also an opportunity to counsel women onnutrition, breastfeeding, and other preventive healthissues.Adult Medicaid Quality Grant Program: Measuring andImproving the Quality of Care in Medicaid. This twoyear grant program was designed to support stateMedicaid agencies in developing staff capacity tocollect, report, and analyze data on the Adult Core Set.Figure 1. Percentage of Women Enrolled inMedicaid and CHIP Who Delivered a Live Birth witha Postpartum Care Visit on or Between 21 and 56Days after Delivery, FFY 2014 (n 34 states)For this reason, improving the rate and content ofpostpartum visits were areas of focus for the Medicaidand the Children’s Health Insurance Program (CHIP)Maternal and Infant Health Initiative. To establish abaseline and monitor performance moving forward, theCenter for Medicaid and CHIP Services (CMCS) addedthe Postpartum Care (PPC-AD) measure to the MedicaidAdult Core Set from the Core Set’s inception in 2013.The postpartum care (PPC) visit rate ranged from 20 to90 percent among the 34 states 1 using Adult Core Setspecifications to report the measure for federal fiscalyear (FFY) 2014. The median postpartum visit rate was58 percent, with a 21-point spread between the 25th and75th percentiles. As shown in Figure 1, there wassubstantial room for states to improve the PPC visit ratefor Medicaid and CHIP beneficiaries.In order to drive improvement on this measure, CMCSconvened the Postpartum Care Action Learning Series(referred to as the Action Learning Series). The ActionLearning Series was a structured, team-basedcollaborative learning experience which provided 10states an opportunity to develop and implement qualityimprovement (QI) projects to improve postpartum carein Medicaid and CHIP. In addition, CMCS launched the1Source: Mathematica analysis of 2014 Adult Core Set reports.The Action Learning Series and AMQ participant statesimplemented small tests of change to first identify andvalidate their proposed interventions. As such, theseactivities did not necessarily result in changes instatewide core set postpartum care measure rates.However, these projects gave states experience inundertaking QI activities and gave them valuableinformation on what strategies were and were noteffective. States could then work toward spreading andscaling those small tests of change that demonstratedproof of concept. This fact sheet describes the QI teamsThe term “states” includes the 50 states and the District of Columbia.This issue brief is a product of the Technical Assistance and Analytic Support for the Medicaid and CHIP Quality Measurement and ImprovementProgram, sponsored by the Center for Medicaid and CHIP Services. The technical assistance team is led by Mathematica, in collaboration with the NationalCommittee for Quality Assurance, Center for Health Care Strategies, AcademyHealth, and Harbage Consulting.1
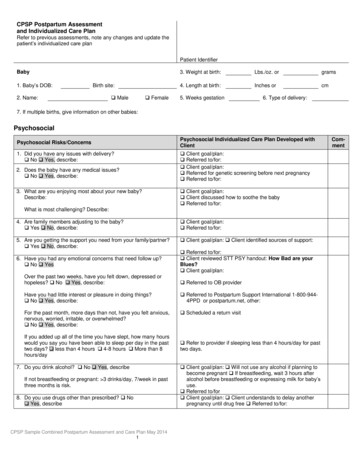
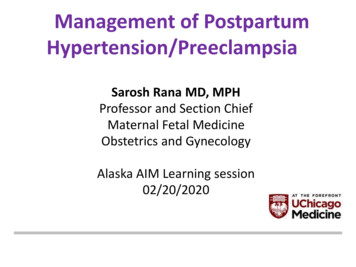
in the 10 states, their aims, the interventions they tested,their results, and lessons learned. In addition, this factsheet provides summaries of the postpartum care-relatedprojects that four states undertook as Adult MedicaidQuality (AMQ) grantees.Team leaders: Chris McInnish, Melinda Rowe—Alabama Medicaid AgencySummary of state QI strategiesPartners: Alabama Department of Public HealthStates tested a variety of strategies to improve the PPCvisit rate, the content of the visit, and access to effectivecontraception. Figure 2A (next page) displays a driverdiagram representing the primary drivers (systemcomponents) and secondary drivers (activities) the statesidentified for improving the PPC visit rate. The primarydrivers included: changes to payment and billingpolicies; team-based care using case managers, carecoordinators, and community health workers (CHWs) toconnect women to services such as transportation;beneficiary engagement using appointment remindersand education; and provider education about theimportance of the PPC visit.Aim: The specific aims related to PPC were: (1) toincrease the PPC-AD rate from 76 to 78 percent; (2) toincrease the percentage of postpartum women whoparticipated in the Plan First Program (the state’sMedicaid family planning waiver) from 34 to 36 percent;and (3) to increase to 45 percent the percentage ofpostpartum women who kept their primary careappointments.With regard to improving the content of the PPC visit,including increased access to effective methods ofcontraception, figure 2B (next page) displays a driverdiagram representing the primary system componentsand activities states identified. The primary driversincluded: payment policies; team-based and patientcentered care delivery models; provider and teammember education; and beneficiary engagement througheducation.The state profiles that follow describe the policy andprogram changes that the 14 states tested, results (ifavailable), and next steps. The profiles also describelessons states learned about implementing the QI processand about improving postpartum care in Medicaid andCHIP. At the conclusion of the Action Learning Series,several states planned to continue their efforts toimprove postpartum care by aligning with other state QIactivities, such as the infant mortality CollaborativeImprovement & Innovation Network (CoIIN). 2 Inaddition, several states planned to continue their effortsto improve postpartum contraceptive care underCMCS’s Maternal and Infant Health Initiative (MIHI)grant program. 32 The CoIIN to Reduce Infant Mortality is a public–privatepartnership to reduce infant mortality and improve birth outcomes.See -coiins.2State profilesAlabamaProject summary: Medicaid beneficiaries who remainedon Medicaid after the 60-day postpartum period and whohad a current or previous adverse birth outcome wereeligible for the project. Maternity care contractor casemanagers visited new mothers in the hospital beforedischarge to determine whether the mother met criteria forparticipation in enhanced interconception care (ICC) casemanagement. Eligible women who agreed to participatewere referred to case managers at the Alabama Departmentof Public Health (ADPH) who referred women and theirinfants to primary care providers for postpartum and wellchild care. In addition, ADPH case managers distributedthe Alabama Collaborative Improvement and InnovationNetwork to Reduce Infant Mortality ICC Guidelines tothe mothers’ primary care providers (389 physicians)from January 2013 to January 2015 to educate them onICC including the postpartum visit.A total of 1,149 women were referred for ICC casemanagement and ADPH case managers located 924 (80percent) of the women. Of the 924 women, 673 (59percent of those originally referred) agreed to receive ICCservices. Of those who agreed to receive ICC services,283 (42 percent of participants) had a PPC visit within 60days postpartum. The percentage of postpartumbeneficiaries participating in Plan First increased from 34to 75 percent.More information about the MIHI grant program is available h/data-andmeasurement/index.html.3
Figure 2A. Aim and Key System Drivers and Activities to Improve the Rate of Postpartum Care VisitsFigure 2B. Aim and Key System Drivers and Activities to Improve the Content of the Postpartum CareVisit3
Results: The statewide PPC visit rate increased from 76percent at baseline (FFY 2013) to 80 percent in March2015.Lessons learned: Adhering to strict eligibility criteriafor inclusion in the intervention made it difficult toenroll a sufficient number of participants to assess theintervention’s impact.Next steps: Alabama planned to transition to Medicaidmanaged care and was developing 11 regional careorganizations to deliver and manage care under acapitated payment system. A quality assurance advisorycommittee of providers, stakeholders, and researchersincluded the PPC-AD measure as one of the requiredquality measures regional care organizations must report.In addition, Alabama planned to collect and report dataand assess progress on postpartum contraceptive careunder the MIHI grant program.ArizonaTeam leader: Kim Elliott—Arizona Health Care CostContainment System (AHCCCS)Team members: Jakenna Lebsock, quality leader;Laurene Kordell, data manager—AHCCCSPartners: Mercy Care Plan; UnitedHealthcare; RobertKrauss, DO, obstetrician and medical director—Bridgeway Health Solutions; and private obstetricalpracticesAim: By July 2015, to have increased by 50 percent therates of postpartum visits and provider–patient familyplanning discussions at the obstetrical practice with thelargest Medicaid population in the state.Project summary: The Arizona team tested severalchanges as part of the project, including: (1) adding areminder call 72 hours before the PPC visit in addition tothe existing reminder call 24 hours before the visit; (2)writing an order in the woman’s hospital chart remindingthe provider to remind the woman to schedule the PPCvisit appointment; (3) distributing PPC visit reminderpostcards to women after delivery; and (4) encouragingproviders to use the teach-back method 4 to engagewomen in family planning discussions. All of the officesof the pilot site practice implemented the 72-hourreminder calls; the remaining interventions targeted fivephysicians from a geographic area where the postpartumvisit compliance rate was low.4 Resources on the teach-back method are available seTeachBack!.aspx.4Results: The pilot site successfully implemented the 72hour postpartum visit reminder, so that all postpartumwomen with scheduled appointments received either anelectronic reminder (60 percent) or phone call fromoffice staff (40 percent). Although the pilot siteencouraged providers to write PPC visit orders inpatients’ records at the hospital, the pilot site was notable to evaluate how often orders were implemented, asproviders reported that this practice was alreadystandard. Similarly, in response to learning about theteach-back method to aid in family-planning discussions,providers reported that they already used a comparablemethod and felt it was helpful in communicating withpatients.At baseline (January 10 to April 2, 2014), 59 percent ofwomen in the pilot site made a postpartum visit beforethe QI project started, and 54 percent made a postpartumvisit during the second round of data collection(February 1 to April 1, 2015). The family-planningservices discussion rate was 82 percent at baseline andremained the same at the second round of datacollection.Lessons learned: More time for follow-up is necessaryto assess the full impact of the interventions. Datacollection took longer than anticipated because theelectronic health record did not capture all of thenecessary data points and staff at the pilot site had tomanually extract some data through chart reviews.Next steps: The Arizona team planned to use the resultsfrom the QI project to facilitate discussions with healthplans on ways to increase the PPC visit rate and on theeffective use of contraceptive methods. The team alsoplanned to focus on improving data collection and tocontinue assessing how to use data to initiate change toincrease the PPC visit rate.CaliforniaTeam leader: Julia Logan—Department of Health CareServices (DHCS)Team members: Susannah Cohen, Vivian Szeto, andSydney Armendariz—DHCS; Barbara Boehler—Communicare Health CentersPartners: Communicare Health Centers; PetalumaHealth Clinic; Marin County Clinic; CaliforniaDepartment of Public Health; LA Care Health Plan;Health Net Partnership Health Plan; Text4baby;
California Maternal Quality Care Collaborative; CaliforniaWIC AssociationAim: By December 31, 2015, to increase by 10 percentover baseline the postpartum visit rate in the pilot sites.Project summary: The California team convened astatewide learning collaborative of key DHCS andMedicaid managed care plan staff including qualitydirectors, medical directors, and health educators. TheQI collaborative used regular, action-orientedteleconferences to share challenges and lessons learned,identify and resolve state and local barriers, and receiveand provide technical assistance. One learningcollaborative member, LA Care, shared a successfulmodel, the Healthy Mom Postpartum Program, whichwas developed to address problems identified during abarrier analysis. The program components includescheduling assistance, transportation, interpreter services,and member incentives to attend the postpartum visit.The program served nearly 50 percent of potentiallyeligible women and participants had a postpartum visitrate of 76 percent in 2014.Results: No results were available by the end of theproject.Lessons learned: It takes time to engage clinics and totailor the pilot programs to the clinics’ concerns andbarriers. Collaboration was key to receiving clinics’ buyin. Incorporating feedback from clinic staff who workdirectly with Medi-Cal members was also important.Finally, the team learned that the clinics and managedcare plans have competing priorities and limitedresources for QI projects.Next steps: The California team planned to conducttelephone interviews with new mothers who gave birthat a Communicare Health Center to ask them about theirexperiences with health care during and after pregnancy;their reasons for missing appointments and solutions toavoid missed appointments; their opinions on the valueof PPC visits; and the effectiveness of incentives, suchas gift cards and text message reminders, to encourageattendance at PPC visits. California planned toimplement interventions at the state, managed care plan,and clinic levels. At the state level, DHCS planned toupdate PPC visit documentation policies regardingglobal billing and delivery notification procedures.Managed care plans also planned to update theirdocumentation policies and conduct member outreachduring the prenatal period. Clinics planned to conductpatient outreach and to educate patients about PPC visitsand long-acting reversible contraceptives (LARCs). The5California team planned to test patient reminders early inthe postpartum period. In addition, California planned tocollect and report data and assess progress onpostpartum contraceptive care under the MIHI grantprogram.GeorgiaTeam leaders: Janice Carson, Erika D. Lawrence—Georgia Department of Community Health (DCH)Team members: Amerigroup Community Care;Georgia Regents University (GRU); Peach State HealthPlan; WellCare of Georgia, Inc.Partners: Amerigroup: Eagles Landing OBGYNPractice (ELOGA); GRU: GRU Women’s ClinicalServices; Peach State: Georgia Obstetrical andGynecological Society and DeKalb Women’s SpecialistOBGYN Associates; WellCare: Grady MemorialHospitalAims: (1) By June 30, 2015, to increase by 10percentage points over baseline the number of Medicaidand PeachCare for Kids women who had a postpartumvisit within 21 to 56 days of delivery. (2) To increase by20 percentage points the number of low-income womenin their last trimester of pregnancy who engaged in areproductive life plan discussion and selected immediatepostpartum LARC insertion as their contraceptivemethod.Project summaries and results: Each care managementorganization (CMO) focused on a high-volume providerto improve the PPC-AD visit rate. The projects weredesigned to determine whether provider and membereducation along with other interventions would improvethe PPC-AD visit rate and effective contraceptive use.The approaches and progress varied across the fourCMOs.Amerigroup project: The Amerigroup pilot siteprovided prenatal education about the importance ofPPC visits to members, educated providers about thepostpartum care visit Healthcare Effectiveness Data andInformation Set (HEDIS) guidelines, and provided officescheduling staff with financial incentives tied to womenkeeping their appointments.Amerigroup results: At baseline (January 1 toDecember 31, 2013), the PPC-AD visit rate was 67percent. After the interventions, in February, March, andApril 2015, the rates were 78, 65, and 68 percent,respectively. A postpartum rapid-cycle performanceimprovement project was put in place at Amerigroup.
GRU project: The GRU pilot site educated patientsabout reproductive life planning and the PPC visit duringthe prenatal visits to test whether women would choosepostpartum LARC insertions immediately following thereproductive life plan discussions. A delay in finalizingsystem configurations for hospital reimbursement ofLARCs by DCH and the CMOs was a barrier toimmediate postpartum insertion.GRU results: GRU’s baseline (June through December2014) PPC visit rate was 58 percent; the rate fromJanuary to April 2015 was 54 percent. Staff noted thatmany of the patients sent to GRU for delivery receivedprenatal and PPC from other providers in thesurrounding area. These women are included in GRU’sdenominator but might receive their PPC visits fromanother provider.WellCare project: WellCare’s pilot site initiallyfocused on providing PPC visits in the patient’s home,along with member and provider education. The siteteam experienced challenges obtaining data to determinethe baseline PPC-AD visit rate, identifying members toparticipate, and holding regular planning meetings withstakeholders. WellCare could not implement a plannedpostpartum home health visit intervention because itcould not secure a licensed provider or vendor tocomplete the specified elements of the visit inaccordance with the standards. Instead, pilot siteleadership and clinicians received education on the fullHEDIS specifications and the difference between thePPC visit and the visit for an incision check.WellCare results: This intervention resulted in a 4point increase in the PPC care visit rate above the goalof 36.3 percent. As a next step, WellCare instituted asecond intervention—to have pilot site clinicians educatemembers at 35 weeks gestation about the importance ofthe PPC visit and the difference between the PPC visitand a visit for an incision check.Peach State project: Peach State identified a highvolume, low postpartum visit rate compliant provider toserve as the pilot site for its project. A proactive outreachmanager called members to remind them to scheduletheir postpartum visits three to six weeks after delivery.The outreach manager offered assistance withscheduling, if needed. The calls were made seven daysafter a delivery, and data were collected to evaluate theeffectiveness of the intervention.Peach State results: No results were available by theend of the project.6Lessons learned: The pilot sites must be fully committedto the project and the defined goals. This commitmentrequires time, resources, and dedicated staff. The detailsmust be discussed fully before confirming the pilot sites.Changes in pilot site personnel significantly affect theimplementation and effectiveness of the project. Effectivecommunication among the state, the CMO, and the pilotsites is essential to identify issues, discuss solutions, andoffer assistance as necessary.The Georgia team identified a unique issue in workingwith an academic site that requires institutional reviewboard approval or a waiver from such approval toparticipate with state Medicaid agencies on QI projects.Because such approvals can be time-consuming, the teamlearned the importance of providing for enough lead timewhen implementing QI projects in academic settings.Next step
Adult Medicaid Quality Grant Program: Measuring and Improving the Quality of Care in Medicaid. This two-year grant program was designed to support state Medicaid agencies in developing staff capacity to collect, report, and analyze data on the Adult Core Set. Figure 1. Percentage of Women Enrolled in