Transcription
9chapter nineDecision andCompliance Support:Utilizing the DatabaseLearning OutcomesAt the end of this chapter, the student should be able to:9.19.29.3Describe the uses of the dashboard inPrimeSUITE to meet Meaningful Usestandards.Explain how data and information areused in decision support.Set up system reports usingPrimeSUITE.9.4Set up custom reports using PrimeSUITE.9.5Illustrate uses for an index.9.6Describe uses for a registry.9.7Explain how data gathered inPrimeSUITE is used in thecredentialing process.Copyright 2012 The McGraw-Hill CompaniesKey TermsAggregateBenchmarkingCenter for Medicare and Medicaid Services (CMS)Clinical Decision Support (CDS)Core objectivesCredentialingCustom reportDashboardDetail reportDrug formularyHealthcare Integrity and Protection Data Bank(HIPDB)IndexIn-networkMeaningful useMenu objectivesMaster Patiet Index (MPI)National Practitioner Data Bank (NPDB)Physicians’ Quality Reporting Initiative (PQRI)QueryRegistrySummary reportVariable175
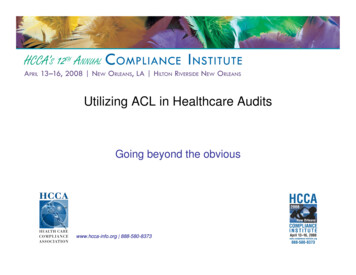
The Big PictureWhat You Need to Know and Why You Need to Know ItRunning reports, supplying information to agencies, and ensuring compliance with licensingagencies, Medicare/Medicaid rules, managed care plans, and accrediting agencies are allresponsibilities of administrative personnel. This person may be an MA who is an office manager, a health information professional, or a healthcare administrator. Participation in the Meaningful Use incentive program, in particular, will require submission of data that showscompliance with the standards in order to receive incentive grants. In this chapter, we will coverPrimeSUITE functionality that allows us to prove compliance with Meaningful Use, licensingagency, insurance providers, and state and federal reporting requirements.9.1Using the Dashboard in PrimeSUITEto Meet Meaningful Use StandardsIn order for eligible professionals and hospitals to receive stimulusmoney, they must successfully show meaningful use of electronichealth data. In other words, eligible professionals and hospitals thatimplement (or upgrade) certified electronic health record systems andcomply with the core and menu objectives (covered below) will be eligible for monetary grants. The Center for Medicare and MedicaidServices (CMS) will administer the program. An agency of theDepartment of Health and Human Services, CMS is responsible foradministering the Medicare program. The core objectives that showmeaningful use of electronic health information include those listed in176Medicare Core Objectives, 2011Core ObjectiveExplanationUse of computerizedphysician order entry(CPOE)Medication orders made by care providers are done electronically rather than in writing in a paper recordDrug-drug and drugallergy checksAn alert system exists, based on the medications and allergies entered for a patient, for potential drug to drug, or drugto allergy effectsePrescribingCare providers place prescriptions electronically rather thanby paperRecording of patientdemographicinformationThe following demographics must be collected on allrecords:– Preferred language– Gender– Race– Ethnicity– Date of birthRecording of a problemlistA listing of all current and active diagnoses for which thepatient is being treated must be maintainedhttp://connect.mcgraw-hill.comCopyright 2012 The McGraw-Hill CompaniesTABLE 9.1
Copyright 2012 The McGraw-Hill CompaniesRecording of a medication listA listing of all current and active medications being taken bythe patient; if the patient is on no medications, the recordmust reflect that as wellRecording of amedication allergy listA listing of medication(s) to which the patient is allergicRecording of vital signsOn each visit, the following must be recorded:– Height– Weight– Blood pressure– Body Mass Index (BMI)– Maintenance of a growth chart (for children 2–20 years,including BMI)Recording of smokingstatusFor patients 13 years of age and older, smoking status mustbe recordedClinical decision supportfunctionalityAt least one clinical decision support rule must be implemented. Example: A patient with a fasting blood sugarabove 120 mg/dL may trigger an alert for diabetes mellitus,type 2Reporting clinical qualitymeasuresEach provider must specify the Reporting Numerators,Denominators, and Exclusions for each quality measurereportedAbility to exchange keyclinical informationbetween/among careprovidersThe capability to share among care providers such information as problem list, medication list, allergies, and diagnostictest resultsAbility to provide anelectronic copy of healthinformationPatients must be provided with electronic health informationupon request; includes test results, problem list, medicationlist, and medication allergiesAbility to provide clinicalsummariesFor each office visit, a clinical summary should be providedto each patientPrivacy and SecurityprovisionsThe software in use meets or exceeds standards set forthby the ONC Meaningful Use standards and includes technical specifications that ensure the privacy and confidentialityof information found in the databaseTable 9.1. For 2011, meeting the 15 core objectives listed in Table 9.1 isrequired.Core objectives are the basic functions that should be completedon a patient’s visit or hospitalization.For hospitals, the core objectives include all of those listed in thetable except ePrescribing.The 2011 Menu Objectives for Medicare include those listed inTable 9.2. Of the 10 listed, five must be met.Menu objectives are additional functions that allow for greateruse of EHR functionality, for instance running statistical reports,registries, or lists; checking for drug interactions; providing patientswith educational materials about their illness; and the like.CHAPTER 9 DECISION AND COMPLIANCE SUPPORT: UTILIZING THE DATABASE177
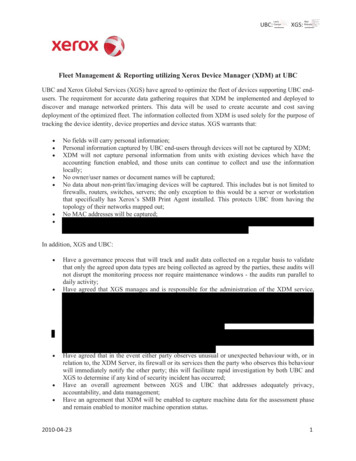
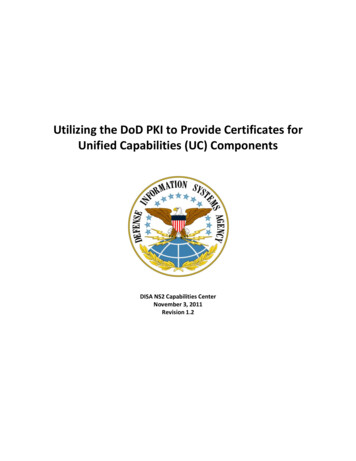
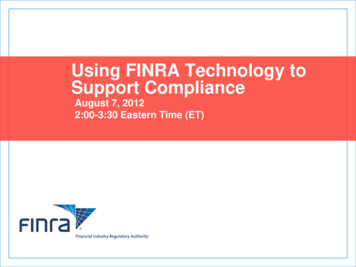
MenuObjectiveMedicare Menu Objectives, 2011ExplanationDrug-FormularyChecksThe office or hospital has access to at least one internal orexternal drug formulary (a list of provider-preferredgeneric and brand-name drugs covered under various insurance plans)Lab test ResultsDocumented in theEHRResults of laboratory tests ordered must be entered into thepatient’s EHR rather than being filed in paper format; resultsmay be entered electronically through electronic data interchange, scanned into the record via manual scanning methods, or manually keyed in to the record from the paperresultsKeeping of PatientListsThe ability to generate a list of patients with a specific conditionin order to satisfy quality improvement initiatives, reducedisparities, for research, or for outreach to patients with thatdiagnosisPatient RemindersGeneratedThe ability to send reminder letters (or electronic reminders) forpreventive and/or follow-up careTimely ElectronicAccessThe ability to provide patients with their electronic record withinfour business days of the information being available in electronic formPatient EducationAccess to educational resources using EHR technology and providing the resources to patients, if appropriateMedicationReconciliationDocumentation of medications the patient is taking as prescribedby other care providersSummary of CareThe care provider submits a summary of care to physicians or another healthcare facility that is assessing the patient or takingover the care of the patientImmunizationRegistriesThe capability to submit electronic data to immunization registries or other immunization information systems in accordancewith applicable lawSyndromaticSurveillanceThe capability to submit electronic data to public health agenciesin accordance with applicable lawSee Figure 9.1 for a Clinical Visit Summary given to a patient atthe conclusion of the visit, which would satisfy the Summary of Careobjective.Hospitals must incorporate five of the 10 menu objectives listedin Table 9.2 to be eligible for incentive grants in 2011.Medicaid–eligible providers (physicians, dentists, nurse midwives, nurse practitioners, or physicians’ assistants in rural healthclinics), with some restrictions based on percentage of patients whoare covered by Medicaid, will qualify for the full stimulus amount inthe first year if a practice shows they have adopted, upgraded, orimplemented EHR.178http://connect.mcgraw-hill.comCopyright 2012 The McGraw-Hill CompaniesTABLE 9.2
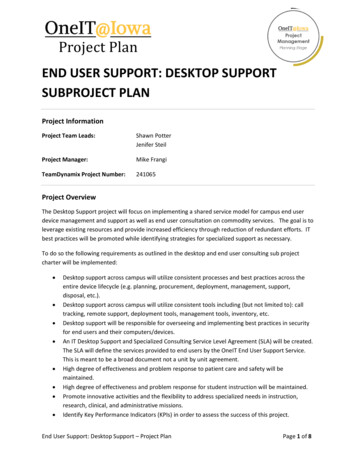
Figure 9.1 Clinical visit summaryGo to http://connect.mcgraw-hill.comto complete this exercise.HIMEHRPMEXERCISE9.1Copyright 2012 The McGraw-Hill CompaniesView a Practice’s DashboardIn the scenario that follows, we are going to view the dashboard (a visualcomparison of actual performance to required performance) of a particularphysician, Dr. William Childs. Notice that for each core and menu objective,the provider’s performance is compared to the required performance. Theoffice manager, health information professional, or other designated individualshould keep close watch on the dashboard to ensure compliance with meaningful use requirements. He or she would then take appropriate action shouldthe percentage of participation fall or should it be apparent that a care provider is in jeopardy of not meeting the threshold. Appropriate action wouldstart with education of the care providers to ensure they all understand theimportance of compliance with meaningful use and understand that not complying will put the practice in jeopardy for receiving stimulus funding.Follow these steps to complete the exercise on your own once youhave watched the demonstration and tried the steps with helpful prompts inpractice mode.1. Click MU Dashboard.2. Click Provider.3. The Search field is filled out with Childs. Press the tab key toconfirm your entry.4. Click William H. Childs MD.5. Click View.tipPrimeSUITE refers tothe core objectives as corerequirements.Take a few moments to review this dashboard. Notice that 15 of the 15required core objectives were met. This means that this physician used the(continued)179
EHR in his practice to fulfill all of the core objectives. Let’s look at one of thecore objectives—keeping a medication list. The requirement is that morethan 80% of all patients seen by the care provider need to have at least oneentry (or documentation that the patient is not currently prescribed anymedication) as a documented data item. Dr. Childs met this requirement96.9% of the time—he documented the medication(s) each patient is taking(or that they are not taking any) 96.9% of the time. For charting vital signs,Dr. Childs met that objective in 96.1% of his patients, while the requirementfor that objective is that for more than 50% of all patients (age 2 and over),records show documentation of the height, weight, and blood pressurerecorded as structured data. You have completed Exercise 9.1 Data and Information Used in DecisionSupportAccording to the Health Information Management and SystemsSociety, “Clinical Decision Support (CDS) is defined broadly as aclinical system, application, or process that helps health professionals make clinical decisions to enhance patient care. Clinical knowledge of interest could range from simple facts and relationships tobest practices for managing patients with specific disease states, newmedical knowledge from clinical research, and other types of information” (HIMSS, 2011).CDS includes reminders and alerts, diagnostic and therapeuticguidance, links to expert resources (CDC, Mayo Clinic, and clinicaltrials, for example), and results of best practices. Many EHR vendors link directly to one of these expert sites. The trigger that a clinical alert or support should be displayed comes from the data thathas already been captured in the patient’s record. This is where thedata dictionary and structured data that we covered in Chapter 2apply. In the exercise that follows, the trigger for the alert flag willbe the patient’s age (calculated by the system), the CPT codes forcolonoscopy, and whether or not one of those codes has beenassigned to any visit for a patient over the past 5 years (derivedfrom calculating five years prior to the date of the visit). Decisionsupport, or clinical decision support, is a functionality of an EHRwhose value cannot be overestimated. Use of CDS tools improvespatient safety, decreases duplication of procedures, reduces the performance of unnecessary testing, and as a result reduces the cost ofhealthcare, while improving patient outcomes, efficiency of care,and provision of clinically relevant, evidence-based care. Clinicaldecision support tools are built into most EHRs, includingPrimeSUITE.Recall that for 2011, meaningful use requires that at least oneclinical support rule be implemented through the use of an EHR,and that there is a means to track compliance. An alert that pops upto ask a patient if he or she has had a colonoscopy does not meet the180http://connect.mcgraw-hill.comCopyright 2012 The McGraw-Hill Companies9.2
requirement unless that alert appears based on certain informationfound in the EHR about that patient compared to evidence-based criteria that has been embedded in the EHR software. For instance, analert for colonoscopy would appear when a patient is 50 years of ageand older, and/or there is an entry in the patient’s problem list showing a history of rectal bleeding, or a family history of colon cancer isdocumented in the history section of his chart, and no CPT procedure codes for colonoscopy have appeared in the patient’s visit history in the past 5 years.Of course, if a care provider has this functionality availablethrough the practice’s EHR software and does not use it, then it is notbeneficial to the patient, to the care provider, to the practice, or tosatisfy meaningful use standards. There are still care providers whoview CDS systems as “cookbook medicine”; those who find it tootime consuming or who are annoyed by the pop-up reminders. Oneincentive to encourage the use of a CDS is pay-for-performance programs available in certain managed-care plans. In other words, if thepractice’s fiscal position is improved by using CDS technology, thenthe care providers are more accepting of CDS systems.Go to http://connect.mcgraw-hill.comto complete this exercise.HIMEHRPMEXERCISE9.2Build a Clinical Alert, Part ACopyright 2012 The McGraw-Hill CompaniesIn our next scenario, we are going to build a clinical alert in PrimeSUITE.This is a lengthy process for the alert we have chosen, so this will be donein two parts—Exercise 9.2 (Part A) and Exercise 9.3 (Part B).We are going to build a clinical alert for all patients who are 50 years ofage or older who have not had a colonoscopy in the past 5 years. To do this,we will use CPT codes for colonoscopy, of which there are eight. There aremany CPT codes for colonoscopy because the codes differ based on the reason for doing the procedure as well as the extent of the procedure. (You willenter these codes in the order code fields in numerical order during the exercise.) The colonoscopy codes are:4537845382453794538345380453844538145385These are called “filters,” which will select (or exclude) patients from thedatabase who do (or in this case do not) meet certain criteria. In this particular alert we will query the database for patients who are 50 years of age orolder and who do not have one of the colonoscopy codes listed aboveattached to any of their visits for the past 5 years; once the alert is set up,their electronic record will then have the red ribbon icon attached to showthat a colonoscopy is needed. To query means that we are going to search or“ask” the database for records that meet (or do not meet) the criteria noted inthe filters. In our example we are querying the database for patients who are50 years of age or older and who do not have one of the eight colonoscopycodes listed above attached to any of their visits over the past 5 years.(continued)181
You have completed Exercise 9.2 182http://connect.mcgraw-hill.comCopyright 2012 The McGraw-Hill CompaniesFollow these steps to complete the exercise on your own once you havewatched the demonstration and tried the steps with helpful prompts in practice mode. Use the information provided in the scenario above to completethe information.1. Click Clinical Alerts.2. The Clinical Alert Description field is filled out with Pt due forcolonoscopy. Press the tab key to confirm your entry.3. Click Clinical Alert Filters.4. Under the Include patients that meet All of the following criteria:section, click Field Name.5. Click scroll button.6. Click Patient: Age.7. Click Operator.8. Clicking the entry is greater than or equal to selects it.9. The Match Value field is filled out with 50. Press the tab key to confirm your entry.10. Under the Include the patients that have NOT had or do NOTmeet All of the following criteria: section, click Field Name.11. Click scroll button.12. Click Order: Order Code.13. Click Operator.14. Click matches any value in list.15. Clicking the entry Create Match List selects it.16. The Order: Order Code field is filled out. Press the tab key to confirmyour entry. (This is where you will start entering the codes, beginningwith 45378.)17. Click Add.18. The Order: Order Code field is filled out. Press the tab key to confirmyour entry.19. Click Add.20. The Order: Order Code field is filled out. Press the tab key to confirm your entry.21. Click Add.22. The Order: Order Code field is filled out. Press the tab key to confirm your entry.23. Click Add.24. The Order: Order Code field is filled out. Press the tab key to confirmyour entry.25. Click Add.26. The Order: Order Code field is filled out. Press the tab key to confirm your entry.27. Click Add.28. The Order: Order Code field is filled out. Press the tab key to confirm your entry.29. Click Add.30. The Order: Order Code field is filled out. Press the tab key to confirm your entry.31. Click Add.32. Click OK.
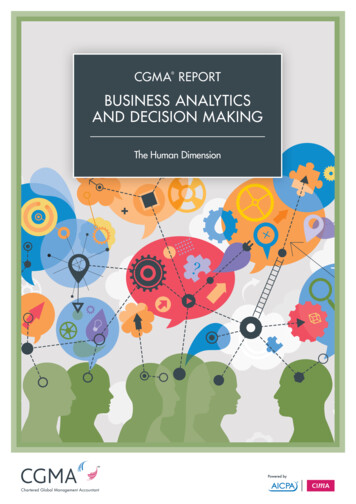
Go to http://connect.mcgraw-hill.comto complete this exercise.HIMEHRPMEXERCISE9.3Build a Clinical Alert, Part BIn Part B we will continue adding filters, and you will need the followinginformation:The URL needed for the Clinical Alert URL is: http://www.cdc.gov/cancer/colorectal/basic info/screening/guidelines.htm. This practice haschosen to use the Centers for Disease Control and Prevention (CDC) as theorganization from which they base their expert advice.This alert will be named “Colonoscopy Needed” (without the quotes).Follow these steps to complete the exercise on your own once youhave watched the demonstration and tried the steps with helpful prompts inpractice mode. Use the information provided in the scenario above to complete the information.1.2.3.4.5.6.7.8.9.10.11.12.13.14.In the second row from the top, click Field Name.Click scroll button.Click Order: Order Date.In the second row from the top, click Operator.Clicking the entry in the past selects it.Click #.Click 5.Click year(s).Clicking the entry OK selects it.Click OK.Click Clinical Alert Flag.Click Colonoscopy Needed.Click OK.The Clinical Alert URL field is filled out. Press the tab key to confirm your entry.15. Click Save.16. The Enter Alert Name field is filled out. Press the tab key to confirmyour entry.17. Click Save.Copyright 2012 The McGraw-Hill Companies You have completed Exercise 9.3 9.3Use of Report-Writer for System ReportsPrimeSUITE and other PM/EMR software offer a multitude of standard reports that are set to run at certain times (end of month, forexample) or on demand, as the information is needed. Some of thestandard reports available in PrimeSUITE are: Payment analysisProcedure code analysisProvider revenue summaryPatient balancesCHAPTER 9 DECISION AND COMPLIANCE SUPPORT: UTILIZING THE DATABASE183
Referring provider Appointment analysis reportFigure 9.2 Report Selection screen184http://connect.mcgraw-hill.comCopyright 2012 The McGraw-Hill CompaniesThe standard reports listed above and others in the reportslibrary are necessary for efficient running of the office. Not keepinga close watch over revenue, balances, and constantly battling scheduling conflicts is
9.1 Using the Dashboard in PrimeSUITE to Meet Meaningful Use Standards In order for eligible professionals and hospitals to receive stimulus money, they must successfully show meaningful use of electronic health data. In other words, eligible professionals and hospitals that implement (o