Transcription
Psychology, Health & MedicineISSN: 1354-8506 (Print) 1465-3966 (Online) Journal homepage: https://www.tandfonline.com/loi/cphm20Stress and psychosomatic symptoms in Chineseadults with sleep complaints: mediation effect ofself-compassionNancy Xiaonan Yu, Jessie S. M. Chan, Xiaowen Ji, Adrian H. Y. Wan, Siu-manNg, Lai-Ping Yuen, Cecilia L. W. Chan & Celia H. Y. ChanTo cite this article: Nancy Xiaonan Yu, Jessie S. M. Chan, Xiaowen Ji, Adrian H. Y. Wan, Siuman Ng, Lai-Ping Yuen, Cecilia L. W. Chan & Celia H. Y. Chan (2019) Stress and psychosomaticsymptoms in Chinese adults with sleep complaints: mediation effect of self-compassion,Psychology, Health & Medicine, 24:2, 241-252, DOI: 10.1080/13548506.2018.1546014To link to this article: shed online: 13 Nov 2018.Submit your article to this journalArticle views: 94View related articlesView Crossmark dataFull Terms & Conditions of access and use can be found ation?journalCode cphm20
PSYCHOLOGY, HEALTH & MEDICINE2019, VOL. 24, NO. 2, 6014Stress and psychosomatic symptoms in Chinese adults withsleep complaints: mediation effect of self-compassionNancy Xiaonan Yu a, Jessie S. M. Chanb,c, Xiaowen Jib, Adrian H. Y. Wanc, Siuman Ngb, Lai-Ping Yuend, Cecilia L. W. Chanb,c and Celia H. Y. ChanbaDepartment of Social and Behavioural Sciences, City University of Hong Kong, Hong Kong, China;Department of Social Work and Social Administration, Faculty of Social Sciences, The University ofHong Kong, Hong Kong, China; cCentre on Behavioral Health, Faculty of Social Sciences, The University ofHong Kong; dInternational Association for Health and Yangsheng, HongKong, ChinabABSTRACTARTICLE HISTORYAlthough stress has been widely acknowledged to link to psychosomatic dysfunctioning, the underlying mechanism that transmitsthe impact is not adequately investigated. This study examinedself-compassion as a potential mediator that may explain thepathway from stress to depressive and somatic symptoms. Datain the present study were drawn from a baseline survey of 998Chinese participants who enrolled in an intervention study onsleep disturbance in Hong Kong. Participants completed measuresof perceived stress, self-compassion, depressive symptoms, andsomatic symptoms. The results showed that stress was associatedwith depressive symptoms (r .79, p .01) and somatic symptoms(r .47, p .01). The path analyses showed that low levels of selfcompassion mediated the association between stress and psychosomatic symptoms. Our findings provide insight into the pathwayhow stress affects psychosomatic symptoms. The interventionprograms for stress management to improve psychological andphysical functioning are recommended to consider selfcompassion as a promising component in practice.Received 17 January 2018Accepted 31 October 2018KEYWORDSStress; self-compassion;depressive symptoms;somatic symptoms; ChineseIntroductionStress has been widely documented to lead to psychological dysfunctions (Stroud,Davila, & Moyer, 2008; Tennant, 2002) and somatic symptoms (Murberg & Bru,2007; Nomura, Nakao, Sato, Ishikawa, & Yano, 2007). Accumulated evidence hasbeen reported to denote the possible underlying mechanisms such as biomedical andpsychosocial factors to explain the above link (Benight & Harper, 2002; Koo, Russo,Ferguson, Nestler, & Duman, 2010). An important direction of investigating thepotential mediators is to identify malleable components which can be modified in costeffective intervention programs and in turn alleviates the impacts of stress.CONTACT Cecilia L. W. Chancecichan@hku.hkDepartment of Social Work and Social Administration, TheUniversity of Hong Kong, 5/F, Jockey Club Tower, The Centennial Campus, Pokfulam, HKSAR; Celia H. Y. Chanchancelia@hku.hkDepartment of Social Work and Social Administration, The University of Hong Kong, 5/F, JockeyClub Tower, The Centennial Campus, Pokfulam, HKSARNancy Xiaonan Yu and Jessie S. M. Chan contributed equally to this work. 2018 Informa UK Limited, trading as Taylor & Francis Group
242N. X. YU ET AL.In the transactional model of stress, individuals whose pressure exceeds one’s capacityto cope are at risk for various dysfunctions including depression and physical problems(Lazarus & Folkman, 1984). Under stressful situations, depressive symptoms have beenfrequently found to coexist with physical complaints (Demyttenaere et al., 2006; LloydWilliams, Dennis, & Taylor, 2004). The theoretical frameworks explaining the pathwayssuggest that the impact of stress on psychosomatic disorders is not simply a direct link,and that some factors may play important mediating roles to transmit the impact (Aldwin,2007; Taylor & Aspinwall, 1996). Factors include biological (e.g., hypothalamic–pituitary–adrenal [HPA] abnormalities, serotonin-transporter-linked polymorphic region[5-HTTLPR] gene), developmental (e.g., childhood experience), psychological (e.g., cognitive style, negative affectivity), and sociodemographic factors (e.g., poverty, gender) havebeen explored to explain the link between stress and psychosomatic disorders (Hammen,2005; Watson & Pennebaker, 1989). Compared with the biological, developmental, andsociodemographic characteristics, psychological factors are more easily to be altered inintervention programs. Identifying the psychological mechanism that may explain theimpact of stress on psychosomatic disorders is important to inform development ofpotentially effective strategies for stress management programs tailored for the needs ofa target population. Different to the deficit-oriented approach to focus on maladjustment,positive attributes have received increasing attention due to the prominence of theirprotective roles in building resilience amongst adversity with empirically-supported evidence of effective intervention strategies (Seligman & Csikszentmihalyi, 2000). The potential psychological mechanism via positive psychological attributes underlying the impact ofstress has not been well understood.Self-compassion is an important construct with emerging evidence in health psychology research (MacBeth & Gumley, 2012). It represents an ability to show compassion toward oneself and have a nonjudgmental relationship with oneself in the face offailures and shortcomings (Neff, 2003b). Self-compassion entails three components inthe face of suffering or personal failures: (a) self-kindness: being kind to oneself andunderstanding personal shortcomings, but not judging oneself with self-criticism; (b)common humanity: viewing one’s imperfect experiences as part of the shared humanexperience, but not isolated and defeated; and (c) mindfulness: maintaining balancedawareness of one’s negative thoughts and feelings with openness, but not suppressing orruminating them (Neff, 2003b). Self-compassion represents a sense of spirituality thatstems from Buddhist psychology. Previous studies showed that practicing Buddhistswere more self-compassionate than other groups, and Buddhists who practiced forlonger periods reported higher levels of self-compassion than new practitioners (Neff,2003a). On the other hand, self-compassion was conceptualized with secular terms(Neff, 2003b). This psychological construct is similar to psychology concepts such asunconditional positive regard (Rogers, 2007), unconditional self-acceptance (Cristea,Montgomery, Szamoskozi, & David, 2013), and self-empathy (Tantillo, 1998). Themeasurement of self-compassion, the Self-Compassion Scale (Neff, 2003a), constitutesnonreligious language and has been widely used among non-religious populations.In meta-analysis studies, self-compassion has been reported to be negatively correlatedwith affective disorders (e.g., depression, effect size r .51) (MacBeth & Gumley, 2012). Inaddition, self-compassion remained significant to predict well-being among stressful individuals after controlling for factors such as goal regulation and social support that had been
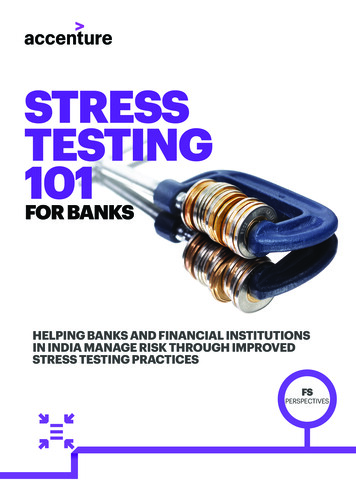
PSYCHOLOGY, HEALTH & MEDICINE243previously reported as predictors of well-being (Neely, Schallert, Mohammed, Roberts, &Chen, 2009). Moreover, self-compassion also has been shown to be associated with lifesatisfaction (Neff, Pisitsungkagarn, & Hsieh, 2008), positive affect, happiness, and optimism(Neff & Vonk, 2009). Compared to the abundant evidence showing the link between selfcompassion and psychological well-being, only limited studies have investigated the potential physical health-promoting role of self-compassion (Terry & Leary, 2011). For example,a study documented that individuals with low levels of self-compassion have reported moresomatic symptoms (Castilho, Pinto-Gouveia, & Duarte, 2015), and another study reportedthat only two composites of self-compassion such as self-judgement versus self-kindnessand over-identification versus mindfulness were associated with more physical symptomswhile the composite of isolation versus common humanity was not significantly associatedwith physical symptoms (Hall, Row, Wuensch, & Godley, 2013). Individuals with higherlevels of self-compassion were found to have more health-related cognitions and affect andseek medical attention sooner when experiencing symptoms and illnesses as they hada proactive approach to health, benevolent self-talk, and a tendency of self-kindness(Terry, Leary, Mehta, & Henderson, 2013). Similarly, a recent study showed that selfcompassion was associated with fewer physical symptoms and the association was mediatedby health-promoting behaviors (Dunne, Sheffield, & Chilcot, 2018). Therefore, as a healthyform of self-acceptance, self-compassion may play a protective role to counteract the effectof stress on psychological disorders and somatic symptoms. Previous studies showed thatself-compassion mediated the effects of various stressors on depression and indicators forsubjective well-being (Joeng & Turner, 2015; Raque-Bogdan & Hoffman, 2015). However,limited studies have examined self-compassion under stress in the Asian populations (Neffet al., 2008; Wong & Mak, 2013), although this concept originated from Buddhist thoughtsin Asia. It is important to note that self-compassion, with well-developed interventionstrategies to modify, is one of the essences of mindfulness-based interventions (Kuykenet al., 2010). If lack of self-compassion has been proven as an underlying mechanism viawhich stress exerts impacts, there would be a rationale to target self-compassion as one ofthe intervention modules in stress-relief programs.Sleep disturbance is common and is one of the most prevalent somatic symptoms inpatients with cancer, chronic pain, or depression (Cheung, Lau, & Waldmann, 1981;Ohayon, 2005; Savard, Simard, Blanchet, Ivers, & Morin, 2001). Individuals with sleepdisturbance have reported lower quality of life, and more frequent help-seeking andhealthcare utilization (Cheung et al., 1981; Zammit, Weiner, Damato, Sillup, &McMillan, 1999). Using a large Chinese sample with sleep disturbance, this studysought to understand how stress affects depressive and somatic symptoms by examiningthe potential mediator of low levels of self-compassion. We hypothesized that theassociation between stress and psychosomatic symptoms will be mediated by low levelsof self-compassion. The mediation model is shown in Figure 1.Materials and methodsParticipantsThe sample was drawn from baseline data of a mind-body intervention study on sleepdisturbance. The inclusion criteria were 1) being Chinese, 2) self-reporting to have sleep
244N. X. YU ET AL.Depressive symptomsStressSelf-compassionSomatic symptomsFigure 1. The hypothesized mediation model for self-compassion to mediate the associationsbetween stress and psychosomatic symptoms.complaint, and 3) aged above 18 years. After the study was announced in the pressconference through different mass media in the local community, people who hadinterest in the study were screened for eligibility after completing an online questionnaire. A total of 1,004 joined the baseline survey, and six were excluded in data analysisbecause of incomplete assessment. Participants provided informed consent onlinebefore the study commenced. Ethics approval was obtained from the InstitutionalReview Board of the University of Hong Kong and Hong Kong Hospital AuthorityWest Cluster (UW13-485).MeasuresStress was measured using the 10-item Perceived Stress Scale (Cohen & Williamson,1988). This measure has been widely used to measure the perception of stress.Participants rated the frequency of their stressful feeling and thoughts during the pastmonth, e.g., ‘Have you been upset because of something that happened unexpectedly’,‘Have you felt difficulties were piling up so high that you could not overcome them’.The Chinese version has been used to measure stress perception in a clinical sample(Leung, Lam, & Chan, 2010) and elderly people (Ng, 2013) in Hong Kong. TheCronbach’s alpha (α) was .88 in the present study.Self-compassion was measured using the 26-item Self-Compassion Scale with theChinese version (Neff, 2003a; Neff et al., 2008). This measure assesses compassiontoward oneself in face of setbacks and sufferings (Neff, 2015). There are three components with opposite dimensions of compassionate versus uncompassionate behavior:treating oneself with kindness (e.g., ‘I’m kind to myself when I’m experiencing suffering’) versus judging oneself (e.g., ‘When times are really difficult, I tend to be tough onmyself’), viewing one’s flaws and mistakes as common to all people (e.g., ‘When I’mdown and out, I remind myself that there are lots of other people in the world feelinglike I am’) versus being isolated by one’s imperfection (e.g., ‘When I’m feeling down,I tend to feel like most other people are probably happier than I am’), and havingmindful awareness about one’s suffering (e.g., ‘When something upsets me I try to keepmy emotions in balance’) versus avoiding or exaggerating them (e.g., ‘When somethingpainful happens I tend to blow the incident out of proportion’). Confirmatory factoranalysis in the present study showed that our data of the 26 items supported the6-factor model (Chi-square 1016.03, p .05, RMSEA .05, CFI .95, TLI .94,
PSYCHOLOGY, HEALTH & MEDICINE245SRMR .05), and secondary factor analysis replicated the single factor model (Chisquare 55.05, p .05, RMSEA .09, CFI .99, TLI .97, SRMR .02), providingstrong evidence for the theoretical construct of self-compassion. We computed theoverall score to represent the levels of self-compassion, with higher scores indicatinghigher levels of self-compassion. The Cronbach’s α was .93 in the present study.Depressive symptoms were measured using the Center for Epidemiologic StudiesDepression Scale (Radloff, 1977), one of the most widely used self-report measures fordepressive symptoms. The Chinese version has been shown to have good internalconsistency and validity in a Hong Kong Chinese community sample (Cheung &Bagley, 1998). A total score of this scale was used to indicate the severity of depressivesymptoms. The Cronbach’s α was .94 in the present study.Somatic symptoms were measured using the Somatic Symptom Inventory (Kroenkeet al., 1994). This measure assesses the common physical complaints including nausea,muscle soreness, back pains, neck pains, headaches, and heavy feelings in arms or legs.Participants rated how much they were bothered by these symptoms over the last week,using a Likert scale ranging from ‘not at all’ to ‘a great deal’. The total score of the itemswere used to present the levels of somatic symptoms. The Chinese version has beenused in an insomnia sample in Hong Kong (Chung, Yeung, Kwok, & Yu, 2014). TheCronbach’s α was .95 in the present study.Data analysisThe socio-demographic characteristics of the participants are presented. Pearson correlations were computed to examine the bivariate associations among the study variables. In the path analyses, the observed variables instead of latent variables were usedbecause this approach produces more conservative path coefficients (Stephenson &Holbert, 2003). Goodness of model fit was indicated using several fit indices: 1) chisquare (χ2) test of model fit, 2) root mean square error of approximation (RMSEA), 3)the comparative fit index (CFI), 4) Tucker Lewis index (TLI), and 5) standardized rootmean square residual (SRMR). RMSEA value of less than .06, together with CFI andTLI of close to .95 or above, and SRMR value of less than .08 between the hypothesizedmodel and the observed data, indicate a relatively good fit (Hu & Bentler, 1999). Theindirect effects of self-compassion were estimated. Bootstrapping was used to obtainconfidence intervals. Mplus 7 was used for the data analyses, and p .05 was consideredstatistically significant.ResultsTable 1 provides the demographics for the sample. The majority of the sample arewomen (n 759, 76.1%). Women reported more stress (women: 23.17 5.76, men:21.72 6.89, F 4.07, p .003) and somatic symptoms (women: 69.25 22.73, men:63.06 21.61, F 1.91, p .001) than men. Age was positively correlated with selfcompassion (r .18, p .01) and negatively correlated with stress (r .19, p .01),depressive symptoms (r .15, p .01), and somatic symptoms (r .11, p .01).Single participants reported less self-compassion (single: 16.55 3.66, married:17.32 3.80, F 3.32, p .04) but more depressive symptoms (single: 29.94 13.47,
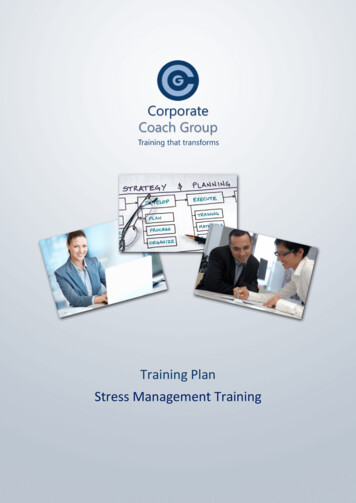
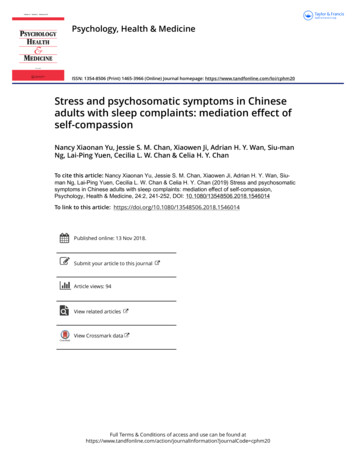
246N. X. YU ET AL.Table 1. Demographic characteristics of the participants (N 998).n (%) or Mean SD (range)SexMenWomenAge (years)Marital statusSingleMarriedDivorced or widowedEducational levelPrimary or belowSecondaryTertiary or higherMonthly income (HK )No income 940,000–49,999 50,000239 (23.9%)759 (76.1%)52.29 11.39 (18–82)204 (20.4%)661 (66.2%)131 (13.1%)103 (10.3%)420 (42.1%)473 (47.4%)345 (34.6%)172 (17.2%)173 (17.3%)96 (9.6%)40 (4.0%)37 (3.7%)54 (5.4%)married: 26.86 13.17, F 6.82, p .001) than married participants. No significantdifference on educational level was shown for any variable. Participants with highmonthly income (monthly income HK 50,000: 18.69 4.14, F 2.67, p .01)reported more self-compassion than those had no income (no income: 16.89 3.64)or low income (monthly income HK 10,000: 16.76 3.33).Bivariate associations among the study variables are shown in Table 2. The perception of stress was associated with depressive symptoms (Pearson’s r .79, p .01) andsomatic symptoms (r .47, p .01). Self-compassion was negatively associated withstress (r .71, p .01), depressive symptoms (r .68, p .01), and somaticsymptoms (r .45, p .01). Depressive symptoms were associated with somaticsymptoms (r .54, p .01).In the path analysis to predict depressive and somatic symptoms, after controlling fordemographic characteristics, the structural model fit the data well, χ2(5) 17.65, p .01;RMSEA .05; CFI .99; TLI .97; and SRMR .01. Regarding the path from stress todepressive symptoms, total effect, total indirect effects, and direct effect were significant (p .01, Figure 2). The results are the same for somatic symptoms (Figure 2). The resultsusing the bootstrap method were identical. These results suggest that individuals whoperceived stress presented low levels of self-compassion, which in turn were associatedwith depressive and somatic symptoms.Table 2. Bivariate correlations of study variables.StressSelf-compassionDepressive symptomsSomatic symptoms**, p .01Mean SD22.82 6.0717.13 3.7727.94 13.2367.77 22.61Stress‒ .71**.79**.47**Self-compassionDepressive symptoms‒ .68** .45**‒.54**
PSYCHOLOGY, HEALTH & MEDICINE24760.19 (2.81)Depressive symptoms1.32 (.06)-.91 (.10)Stress-.44 (.01)Self-compassion.97 (.15)6.96 (.33)42.20 (5.19)-.1.52 (.25)Somatic symptoms379.04 (17.72)Figure 2. The path analysis results of the mediation model for self-compassion to mediate theassociations between stress and psychosomatic symptoms.Note: Coefficients in bold are significant at p .01. Values in parentheses are standard errors for the coefficients.Demographic characteristics including sex, age, marital status, educational level, and monthly income were controlledbut not shown in this figure.DiscussionFurther to supporting existing evidence on the direct effects of stress on depressivesymptoms and somatic symptoms, the present study provides new information on theindirect pathway to delineate the underlying mechanism. Our findings showed thatstressful individuals reported low levels of self-compassion, which in turn transmittedthe impact of stress on depressive and somatic symptoms. Therefore, self-compassion isa useful framework to understand the pathway that stress impacts psychosomaticsymptoms. This positive attribute has the potential for developing clinical programsfor alleviating the impacts of stress.Consistent with the abundant evidence supporting transactional model of stress aboutthe role of stress on psychosomatic dysfunctions in the Western and Asian samples(Castilho et al., 2015; Kim & Cha, 2015; Korinek, Loebach, & Teerawichitchainan, 2016),our findings in a Chinese sample showed that stress is a risk factor for depressive andsomatic symptoms. Although such impacts of stress have been affirmed in differentcultures, there may be distinct mechanisms specific to the studied populations to explainhow the effect exerts (Aranda & Knight, 1997). To address this standpoint, this presentstudy moved further to illustrate the mediating process via self-compassion.Our findings showed higher self-compassion levels among older participants, married individuals, and high-income participants than other groups. Our findings on selfcompassion not only support the limited reports in the Asian samples that low levels ofself-compassion was associated with depression (Wong & Mak, 2013) and somaticcomplaints (Castilho et al., 2015), but also demonstrate that this construct worked asan underlying mechanism linking stress to psychosomatic symptoms in the presentstudy. Our findings highlight the importance of lack of self-compassion in understanding psychopathology in challenging and traumatic circumstances (MacBeth &Gumley, 2012). These results further inform integration of self-compassion into stressmanagement programs to enhance well-being and prevent functional declines. Byincreasing self-compassion toward themselves, stressful individuals may learn to change
248N. X. YU ET AL.their cognitive style and improve their self-care capacity to handle stressors. Theeffectiveness in alleviating emotional distress has been shown in a number of selfcompassion intervention modalities (Barnard & Curry, 2011), including mindful selfcompassion program, compassionate mind training, and acceptance and commitmenttherapy (Barnard & Curry, 2011; Germer & Neff, 2013). For example, a mindfulnessbased stress reduction program was shown to effectively improve self-compassion,reduce stress, and enhance quality of life among health care workers (Shapiro, Astin,Bishop, & Cordova, 2005).After statistically controlling for the indirect effects via self-compassion, the directpathways from stress to depressive and somatic symptoms were substantially reducedyet statistically significant, suggesting that self-compassion has accounted for the mediation effects in part and there are other mediators contribute to explain these associations. Further research should investigate other potential mediators, includingbehavioral (e.g., substance abuse) or physiological factors (e.g., cortisol, serotonin) inaddition to psychological factors (e.g., hope, gratitude, social support), to elucidate theadjustment process. Psychological perspective alone may be insufficient to address theimpact of stress, and biomedical, spiritual, and social perspectives would complementan integrated biopsychosocial intervention paradigm to relieve the impacts of stress.Because Asians, from collectivist cultures, have been described as having a more interdependent self-awareness (Markus & Kitayama, 1991), and because they may have beenexposed to Buddhist teachings through cultural cultivation, Asians might be expected to bemore self-compassionate than Westerners (Neff, 2003b). However, Asians have also beenshown to be self-critical (Kitayama, Markus, Matsumoto, & Norasakkunkit, 1997), suggesting that they may have less self-compassion than Westerners (Neff, 2003b). A studycomparing the cross-cultural difference of self-compassion showed that self-compassionwas the highest in Thailand, followed by the United States, with Taiwan as the lowest,suggesting that general East-West differences could not explain the differences (Neff et al.,2008). However, another study showed comparable levels of self-compassion among theChinese and American participants though the Chinese showed higher levels in selfkindness, common humanity, isolation, and over-identification dimensions (Birkett,2014). Further research examining self-compassion in different ethnic communities mayhelp provide a more complete picture of self-compassion as well as how this constructcontributes to psychosocial well-being in specific cultures.There might be arguments regarding the possibility of replacing self-compassion withother psychological or psychiatric constructs such as self-hatred. Self-hatred is associatedwith psychopathology and maladaptive functioning – the typical focus of traditionalpsychological theories and research (Singer, 2004). On the other hand, exploring selfcompassion contributes to positive psychology, which focuses on human strengths andpotentials, such as their capacity to be happy, to love, and to forgive (Seligman &Csikszentmihalyi, 2000). Social and behavioral sciences could and should play an importantrole in identifying actions and attitudes that help individuals to have richer and moresatisfying experiences in life (Diener, 2000). Previous evidence showed that self-compassioncontributed to quality of life, life satisfaction, hope, and resilience (Kemper, Mo, & Khayat,2015; Neff & Faso, 2015; Van Dam, Sheppard, Forsyth, & Earleywine, 2011). In addition,self-compassion was associated with reduction in depression, anxiety, and stress (Diedrich,Grant, Hofmann, Hiller, & Berking, 2014; MacBeth & Gumley, 2012). Being broader and
PSYCHOLOGY, HEALTH & MEDICINE249embracing a positive connotation compared to self-hatred, self-compassion fits in well withthese positive psychological functioning while maintaining a healthy connection withothers (Barnard & Curry, 2011; Neff, 2003a).There are several limitations in this study. First, the cross-sectional design precludesinference about the direction of influences. A prospective, longitudinal design wouldcontribute significantly to the understanding about the relation between stress and selfcompassion. For example, previous intervention studies have shown the possibility thatself-compassion training predicted decreases in perceived stress (Gard et al., 2012;Shapiro et al., 2005). Future studies may investigate the possibility that unbearablestress leads to diminished self-compassion or vice versa. Second, the self-report measures may raise the possibility for shared method variance that magnify the associationsamong the variables of interest. The observation, interview-based rating methods, orsubjective measures such as cortisol for measuring the stress level, could be consideredin future research. Third, participants responded on the perception of stress, withoutprobing into the nature (e.g., work pressure, interpersonal conflicts, bereavement) andoccurrence (e.g., duration, severity) of specific stressful events. This rating may besubject to the emotional bias. Fourth, participants were recruited in a large clinicaltrial on insomnia, so the results may not be generalized to the community population.ConclusionsIn conclusion, in addition to examining the associations between stress and depressive andsomatic symptoms in a large Chinese sample, the present study highlights the protectivefactor of self-compassion which serves as an important pathway to account for the abovelink. Our findings demonstrate the need to specify the underlying mechanism that promotes psychological and physical functioning in stressful situations which would representthe active components to be incorporated in the invention programs to enhance resilience.Since cost-effective intervention techniques for enhancing self-compassion have been wellestablished, this malleable therapeutic agent can be readily integrated in stress-reliefcounseling and therapies, with evidence-based practice, in the Chinese population.Informed by the partial mediation findings in the present study, future research is calledfor investigation of other potential mediators underlying this association to have betterunderstanding about the underlying mechanisms. In addition, as self-compassion may belinked with specific cultural features among various ethnic communities, future crosscultural studies may address the possible variation in the indirect effect of how selfcompassion contributes to the link between stress and psychosomatic symptoms amongpopulations suffering from threats and challenges.Disclosure statementThe authors have no competing interests to report.FundingThis work was supported by the Centre on Behavioral Health Research Fund of the University ofHong Kong.
250N. X. YU ET AL.ORCIDNancy Xiaonan dwin, C. M. (2007). Stress, coping, and development: An integrative perspective (2nd ed.).New York: Guiford.Aranda, M. P., & Knight, B. G. (1997). The influence of ethnicity and culture on the caregiverstress and coping process: A sociocultural review and analysis. The Gerontologist, 37, 342–354.Barnard, L. K., & Curry, J. F. (2011). Self-compassion: Conceptualizations, correlates, & interventions. Review of General Psychology, 15, 289–303.Benight, C. C., & Harper
Stress and psychosomatic symptoms in Chinese adults with sleep complaints: mediation effect of self-compassion . Health & Medicine, 24:2, 241-252, DOI: 10.1080/13548506.2018.1546014 . Review Board of the University of Hong Kong and Hong Kong Hospital Authority West Cluster (UW13-485).