Transcription
Critical Incident Stress Debriefing andLaw Enforcement: An Evaluative ReviewAbigail S. Malcolm, MSJessica Seaton, MSAimee Perera, PsyDDonald C. Sheehan, MAVincent B. Van Hasselt, PhDEmergency and disaster mental health may have century-old foundations, but itsdevelopment as a field is far from complete (Everly, 1999). One of the more populartactical interventions within the field is the Critical Incident Stress Debriefing (CISD) modelof small-group crisis intervention, developed by Jeffery T. Mitchell (sometimes referred toas the ‘‘Mitchell Model’’). CISD is but one intervention that falls within the strategic arrayof crisis interventions collectively referred to as Critical Incident Stress Management (Everly& Mitchell, 1999; Sheehan, Everly, & Langlieb, 2004). With the advent of CISD camea burgeoning number of case studies, personal accounts, and clinical research reports allfocused on the efficacy of CISD. The purpose of this paper is to examine and critique theliterature specifically addressing the Mitchell Model of CISD with law enforcement.Suggestions for directions that future research on CISD with police officers might take arediscussed. [Brief Treatment and Crisis Intervention 5:261–278 (2005)]KEY WORDS: CISD, CISM, law enforcement, debriefing, group crisis intervention.High impact events, such as the OklahomaCity Bombing, the 1993 World Trade CenterBombing, the Pan Am Disaster, and theFrom the Center for Psychological Studies, Nova South eastern University (Malcolm, Seaton, Perera, Van Hasselt)and the Law Enforcement Communication Unit, FederalBureau of Investigation Academy (Sheehan).Contact author: Vincent B. Van Hasselt, Professor, Centerfor Psychological Studies, Nova Southeastern University,3301 College Avenue, Fort Lauderdale, FL 33314-7796.E-mail: 19Advance Access publication June 29, 2005September 11, 2001, attacks, tax the resourcesof civilians and emergency responders alike(National Institute of Mental Health [NIMH],2002). The response to these events and theresultant research revived an interest in the fieldof emergency mental health. A former BaltimoreCounty firefighter developed the most influen tial intervention, to date, for emergency re sponders in the wake of critical incidents.Mitchell (1983) created Critical Incident StressDebriefing (CISD) in the 1970s to help emer gency responders quickly recover from aª The Author 2005. Published by Oxford University Press. All rights reserved. For permissions, please e-mail:journals.permissions@oupjournals.org.261
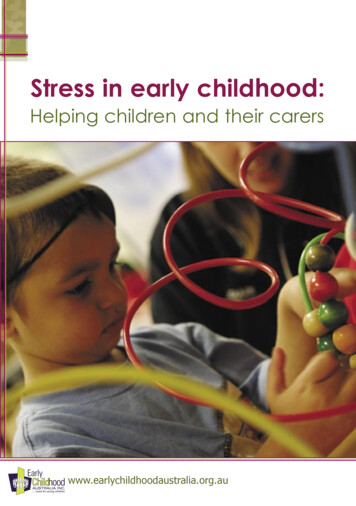
MALCOLM ET AL.traumatic incident. CISD (sometimes referred toas the ‘‘Mitchell Model’’) is a formalized sevenphase group discussion pertaining to a criticalincident, disaster, or traumatic experience.Later, Mitchell collaborated with Everly anddeveloped the strategic Critical Incident StressManagement (CISM) system, ‘‘a comprehensive,integrated multi-component crisis interventionsystem’’ (Mitchell & Everly, 2001). CISM rep resents an effective, strategic continuum ofcare approach to crisis intervention (Sheehan,Everly, & Langlieb, 2004; Wagner, 2005).As CISM developed during the 1990s, over350 crisis response teams were created. TheInternational Critical Incident Stress Founda tion (ICISF) is composed of these teams. ICISFmembers are trained to understand the basicphysiology and psychology of stress, stressmanagement, and traumatic stress. Knowledgeabout traumatic stress allows CISM members tofacilitate the appropriate CISM component inthe acute crisis phase. Table 1 delineates thecore components in the functional integrationthat CISM uses to adapt interventions for theappropriate incident.CISM continues to expand on its originalmodel by incorporating new research andstrategies from the fields of emergency mentalhealth, psychology, faith interventions, mili tary procedures, and individual CISM teamexperience (Everly, 2003a, 2003b; Everly &Langlieb, 2003). It is imperative to understandthat the comprehensive, multifaceted, inte grated nature of CISM was designed for theneeds of emergency responders, their families,and their organizations (Everly & Mitchell,1999). CISM was not developed to replacepsychotherapy or to interfere with the naturalrecovery of human resiliency. Rather, CISMwas designed to facilitate a triagelike process,for a nonpsychiatric population, in the face ofa critical incident as a means of returning theindividual and/or the organization to levels ofprior functioning (Everly & Mitchell, 1999;262Wessely & Deahl, 2003). Moreover, CISD wasdesigned as a small-group crisis interventionwithin the overarching strategic CISM contin uum of care (Everly & Mitchell, 1999).Critical Incidents and Critical IncidentStress DebriefingsA ‘‘critical incident’’ has been defined asa stressful event that is so consuming it over whelms existing coping skills (Kureczka, 1996).A more functional definition describes a criticalincident as an event that has the potential tointerfere with a person’s normal management ofeveryday stress. The Mitchell Model carefullydifferentiates between a critical incident anda crisis response. Again, a critical incident is theevent itself, which is ‘‘critical’’ due to itspotential to engender dysfunction. A crisisresponse is defined as the actual presentationof an individual whose coping resources havebeen overwhelmed by the incident and there isevidence of impairment (Caplan, 1964).One approach to address reactions ofemergency responders to critical incidents isdebriefing. Unfortunately, many researchershave used the term debriefing to encompassa variety of incident–response interventions.This paper uses the terms CISD to refer to theMitchell Model and debriefing to refer to allother descriptions of crisis intervention in theliterature.CISD consists of a group of emergencyresponders, all of whom were involved in thesame critical incident, and the CISD interventionteam members deployed for service. In lawenforcement, the CISD team consists of at leastone peer, who is a law enforcement officer, andat least one mental health professional. The CISDis composed of seven stages. The first stage,Introduction, takes the time to describe theprocess, rules of CISD (i.e., confidentiality), andexpectations. During the Fact Phase, the secondBrief Treatment and Crisis Intervention / 5:3 August 2005
CISD and Law EnforcementTABLE 1. Core Components of CISMInterventionTimingActivationGoalFormat1. Strategic planningPrecrisisphaseCrisisanticipationSet expectations,improve coping, stressmanagementGroups, teams,organizations2. Demobilizations andstaff consultationsShiftdisengagementEventdrivenInform, consult, andallow psychologicaldecompression; stressmanagementLarge groups/organizations3. Assessment of needAnytimepostcrisis4. DefusingPostcrisis(within 12 hr)SymptomdrivenSymptom mitigationtriage, possible closureSmall groups5. CISDPostcrisis(1-10 days,3-4 weeksmassdisasters)Symptom orevent drivenFacilitate psychologicalclosure, triage, symptommitigationSmall groups6. Individual crisisintervention 1:1AnytimeanywhereSymptom drivenSymptom mitigation,return to functioning,referral if neededIndividual7. Family CISMAnytimeSymptom orevent drivenFoster support andcommunications,symptom mitigation,closure if possible,referral if neededFamilies/organizations9. Pastoral crisis interventionAnytimeSymptom drivenMitigate‘‘crisis of faith,’’assist in recoveryIndividuals,families, group10. Follow-up referralAnytimeSymptom drivenAssess mental status,assess needed careIndividual/families8. Community andorganizational consultationNote. CISM ¼ Critical Incident Stress Management; CISD ¼ Critical Incident Stress Debriefing. Adapted from Everly and Mitchell, 1999(p. 21); Everly and Langlieb, 2003.stage, officers are asked to say who they are andwhat their role was in the incident. The nextstage (Thought Phase) asks the officer to sharehis or her first thoughts after the incident. TheReaction Phase, the fourth stage, explores thepersonal reactions surrounding the event. Inthe fifth stage, the Symptom Phase, signs andsymptoms of critical incident stress are discussedand normalized. In the next stage, the officers aretaught different ways of dealing with criticalincident stress in their lives (Teaching Phase).Finally, the Reentry Phase encourages officers todiscuss any other issues and ask questions. Mostimportantly, this phase focuses on returning theofficer to duty. Each stage represents a gradualstep designed to return the emergency re sponder to his/her precritical incident level offunctioning (Mitchell, 1991).Brief Treatment and Crisis Intervention / 5:3 August 2005263
MALCOLM ET AL.Case Example: Oklahoma CityOn April 19, 1995, at 9:02 a.m. a bomb explodedand destroyed the Alfred P. Murrah federalbuilding in Oklahoma City, OK. One hundredand sixty-eight people were killed and morethan 500 were wounded in the blast (Ottley,2003). Although the immediate and long-termeffects on emergency responders includedanxiety, depression, suicide, increased alcoholconsumption, sexual misconduct, increased di vorce rates, and Posttraumatic Stress Disorder(PTSD), levels of these anticipated problemswere lower than predicted (Owen, 1999;Plumberg, 2000; Raymond, 1999).In the wake of this tragedy, researchers havedubbed the aftermath of Oklahoma Citya ‘‘good’’ disaster, indicating that the generaloutcome surpassed what might be expectedfollowing a terrorist attack (Owen, 1999). Theimplementation of the strategic CISM system(and more specifically, CISD via Project Heart land and the Oklahoma Critical Incident StressManagement Network) helped to manage theharmful aspects of traumatic stress (Klinka,1996, 1999). Contributing to the success ofthe outcome was the cooperation and collabo ration among the multidisciplinary team ofemergency response workers (firefighters, lawenforcement officers, emergency medical sup port, clergy, and volunteers). According to CityManager Brown (1995), the team effort of theworkers set a new standard in the face ofdisaster, named, ‘‘The Oklahoma Standard.’’The Oklahoma City response followed the CISMmodel, including CISD for police, and provedthat if followed properly, it is an effective wayto minimize the impact of a critical incident.Review of ResearchSubsequent research from the OklahomaCity Bombing provided support for the CISD264model of crisis intervention. However, CISD isnot without its detractors, and there is exis tent research contradicting the case studysupport for the Mitchell Model (see reviewsby Bledsoe, 2004; Rose, Bisson, & Wessely,2002; Wessely, Rose, & Bisson, 2000). Contro versy has always been associated with newinterventions, and further empirical research isrequired to ascertain the effects of the CISD onreducing harm from critical incidents. How ever, although there is a modicum of researchconcerning the specialized area of emergencymental health, several studies offer evidence ofthe utility of CISD for law enforcementpersonnel. Many of these articles are personalaccounts, of police officers themselves, and areprimarily subjective and anecdotal reports. Thestudies discussed below were selected based ontheir (a) empirically oriented focus and (b)attempt to ascertain the heuristic value of CISDin law enforcement populations.Research Findings1. Robinson and Mitchell (1993) evaluatedthe impact of 31 debriefings on twogroups: emergency services personnel(including 13 police officers) whoparticipated in 18 of the 31 debriefingsand hospital and welfare staff whoparticipated in 13 of the 31 debriefings.The investigators developed their ownevaluation questionnaire, askingparticipants to rate the impact of thecritical incident and the value of thedebriefing using a 5-point scale (1 ¼none; 5 ¼ great) and their perceivedimpact of the event on other personneland family. Additional open-endedquestions (i.e., reasons this criticalincident had an impact on them, otheraspects of their lives that were affectedby their recall of the critical incidentBrief Treatment and Crisis Intervention / 5:3 August 2005
CISD and Law Enforcementincluding family and signs of stress)were included to collect subjective data(e.g., 40% of emergency servicepersonnel indicated that their familieswere impacted by their own criticalincident). Then, following any of the 31debriefings, they mailed thequestionnaire to persons who consentedto being a participant in their study 2weeks postdebriefing. Sixty percent ofall the individuals who participated inthe 31 debriefings consented andresponded to the questionnaire.The hospital and welfare staff ratedthe impact of the critical incident, at thetime of the event, an average of 3.3compared to 2.2 for the emergencyservice personnel. When the evaluationquestionnaire was administered, bothgroups showed a significant reductionin their average rated impact of theevent, although the emergency servicepersonnel showed a larger decrease.CISD was not only rated as valuable butalso viewed as responsible, at least, inpart, for a reduction in stress symptoms(e.g., fatigue, tearing, sleepdisturbances) for both groups.Additionally, both groups rated thedebriefing as considerably valuable tothemselves and other personnel (a rangeof 3.8–4.5). Subjective data also werecompiled about the broader effects ofthe critical incidents and thedebriefings. For example, the evaluationshowed that (a) the type of criticalincident impacts the prevalence ofreported stress symptoms, (b) over 50%of the participants stated that the eventcaused them to recall prior criticalincidents, (c) the most common sign ofstress in emergency service personnelwas cognitive (e.g. sleep disturbance,preoccupation with the incident), and(d) the 96% of emergency responderswho noted decrease in stress symptomsattributed part of their improvement tothe debriefing, particularly because thedebriefing provided an opportunity totalk about the incident.2. Nurmi (1999) assessed the impact ofCISD on police, firefighters, and nursesinvolved in the 1994 rescue of the ferryEstonia off the coast of Finland. Nursesdid not receive CISD because it was nothospital policy, whereas the police andfirefighters did take part in debriefings.All three groups were assessed using theImpact of Event Scale-Revised, the PennInventory, the SCL-90-R, and a speciallydeveloped Perceived Satisfaction withCISD questionnaire. Nurmi found thenurses to be significantly moredistressed than police officers andfirefighters based on the differences inoutcome using the abovementionedmeasures. Responses of the latter twogroups on the Perceived Satisfactionquestionnaire revealed that a majority(81%) found the debriefing to be useful.3. Bohl (1991) examined police officers inSouthern California using the State-TraitAnxiety Inventory, the Beck DepressionInventory, and the Novaco ProvocationScale. All officers had experienceda critical incident 3 months prior to theassessment. Also, 40 underwent a briefpsychological intervention as perdepartmental policy. A second group of31 officers did not receive anyintervention, again, due to departmentpolicy. Bohl found that the officers whoparticipated in the brief interventionshowed a statistically significantdecrease in their rates of stress symptoms(e.g., depression, flashbacks, and anger).4. Smith and de Chesnay (1994) evaluateda CISD program with a South CarolinaBrief Treatment and Crisis Intervention / 5:3 August 2005265
MALCOLM ET AL.police department. Ten officers, from anagency of 100 employees, wereinterviewed by the primary investigator.The primary investigator contacted eachof the 10 officers following a debriefingthat he himself had led. Each officer wasoffered the opportunity to participate inthe study or decline participation; theyall accepted the offer. A semistructuredinterview format allowed theparticipants to discuss any area of thecritical incident, the debriefing, and anyrelated stress. Results indicated that 9 ofthe 10 officers felt that CISD wasbeneficial in helping to reduce theirstress.5. Leonard and Alison (1999) assessedgroups of Australian police officers (N ¼60) who did (n ¼ 30) and did not (n ¼ 30)receive CISD following a shootingincident. The evaluation packetincluded (a) a questionnaire asking fordetails about the incident (e.g., priorexperiences regarding the shootingincident, appraisal of personal safetyduring the shooting incident, supportreceived from the department regardingthe shooting incident), (b) the CopingScale (Carver et al., 1989), and (c) theState-Trait Anger Expression Inventory.They found that the CISD group hadmore shots fired and more people killedor injured in the incident, had scoredhigher on active coping, and weresignificantly less angry than the nonCISD group, on all measures. Leonardand Alison suggested that officers in thenon-CISD group may have reportedelevated anger and poor coping skillsdue to the fact that CISD was not offeredto them; of the 30 officers who did notreceive CISD, it was stated that theyeither refused CISD or were ‘‘overlookedby the Department.’’2666. Carlier, van Uchelen, Lamberts, andGersons (1998) studied trauma in Dutchofficers who responded to a plane crash.The investigators selected their groupsfrom the 200 police officers who arrivedat the crash site, of whom 45% weredebriefed and 55% were not. Thecontrol group of nondebriefed officersconsisted of officers who, according toCarlier et al. (1998), did not attend dueto ‘‘operational reasons’’ (e.g., length ofservice time on scene) or becauseofficers chose not to (e.g., not on duty attime of debriefing, volunteered tocontinue with service dutyuninterrupted). The investigatorsassessed 105 officer participants, 59 ofwhom had not been debriefed andtherefore comprised their control group.The investigators completed the testingat the police departments. They usedthe structured interview for PTSD atboth 8 and 18 months postdisaster.The 8-month assessment revealed thatalthough some of the officers displayedPTSD symptoms postdisaster, only twomet DSM-III-R criteria; there were nosignificant differences between theresearch groups. Results were similar forthe 18-month postdisaster evaluation.7. Carlier, Voerman, and Gersons (2000)described their intervention as theMitchell Model of CISD andadministered debriefings immediatelyafter an unspecified trauma. Theexperimental group of officers (n ¼ 86)had been recruited for participationfollowing their CISD. One control groupof officers (n ¼ 82) did not receive thedebriefing due to operational reasons,which were not stated in the article.Another ‘‘external control group’’(n ¼ 75) consisted of officers whoexperienced a previous traumatic eventBrief Treatment and Crisis Intervention / 5:3 August 2005
CISD and Law Enforcementprior to the institution of debriefingofferings within the department.The pretest and 24-hr postincidenttest phases involved administration ofthe Spielberger State-Trait AnxietyInventory to debriefed andnondebriefed officers but not to theexternal control group. One weekpostincident, the investigators assessedthe debriefed and nondebriefed groupsusing the Self-Rating Scale for PTSD andthe Peritraumatic DissociativeExperiences Questionnaire. Theexternal control group was assessedwith the Impact of Events and thePeritraumatic Dissociative ExperiencesQuestionnaire. The debriefed and nondebriefed groups were again evaluated6 months posttrauma using thestructured interview for PTSD, theAnxiety Disorders Schedule-Revised,additional DSM-IV-related issues (e.g.,dissociation, history of psychiatricillnesses), and several open-endedquestions regarding perceived support,satisfaction with the debriefing, andstress.The investigators found no significantdifferences between groups inpsychological symptoms, number ofsick days taken, or rate of returning towork. However, 98% of the officersreported satisfaction with the debriefingsessions.8. The NIMH (2002) reviewed 17 studies(see Table 4) that used self-describedpsychological debriefings to addressgroups and individuals followingvarious disasters and traumatic events.The review evaluated articles forstandards of research design that weremet, were unmet, or raised otherconcerns. Reviewed articles includeda wide range of populations (medicalpatients, bank tellers, law enforcementofficers). The majority of the groupcrisis intervention ‘‘debriefings’’applied to emergency services, andmilitary personnel yielded positiveoutcomes. However, the debriefingsapplied to individual medical andsurgical patients led to no significantchange and, in some cases, indicatednegative outcomes.9. Young (2003) focused on theeffectiveness of debriefings with lawenforcement populations. Theoverarching goal of this study was toassess the effect of periodic stressdebriefings (debriefings were based onthe Mitchell model of CISD) on officers’levels of depression and PTSDsymptoms. The author suggested thatthe lack of statistically significantfindings in this study reflected on thedebriefings’ lack of focus on internalpolice department stressors (e.g.,supervisors, administrative duties). Itwas not suggested that the resultsindicated a negative effect from thedebriefings; in fact, subjectively, policeviewed the debriefings as helpful andpositive (Young, 2003).10. Sheehan et al. (2004) utilized theapplication of best practices to providelaw enforcement with practical, yetempirically based, informationregarding the issue of law enforcementresponse to critical incidents and criticalincident stress. Their study surveyed 11organizations, including federal, state,and city agencies, and ascertained theirresponse to major critical incidents (e.g.,Waco, 9/11). Using both interviews andwritten descriptions, the authors citedhow these agencies structurallyresponded to large-scale disasters andrelayed their findings to offer tacticalBrief Treatment and Crisis Intervention / 5:3 August 2005267
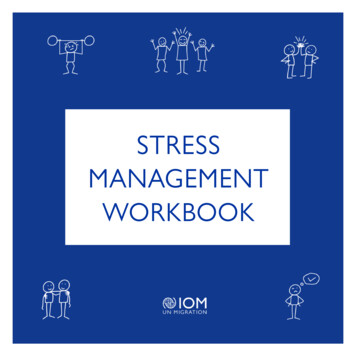
MALCOLM ET AL.TABLE 2. Concerns for CISD Research With Law EnforcementAssessment concernsCISM/CISD specificsCulture as a VariableMeasurementsControl groupOverlapping culture concernsDefinitions and terminologyProper application of CISDPotential for randomized studiesCulture of copsAcceptance of CISDOverlapping assessment concernsNote. CISM ¼ Critical Incident Stress Management; CISD ¼ Critical Incident Stress Debriefing.and stylistic response options for otherlaw enforcement agencies. While thisstudy supported the use of postincidentcrisis intervention, such as CISM,a resounding conclusion from allagencies reviewed in the article focusedon the lack of preincident responses.The authors suggested increasedattention to applying a comprehensiveapproach in response to major criticalincidents, including (a) preincidenteducation, (b) preincident training, and(c) early-warning screening.11. Meta-analysis findings of Roberts,Everly, & Camasso (2005) included theeffect size of multicomponent CISM.The high-average, 2.11, effect size formulticomponent CISM providedstatistical significance and practicalcomparability that most notablysupports the use of debriefings withina comprehensive, multifaceted,integrated continuum of crisisintervention. In sharp contrast, thestudies of one-shot relatively briefdebriefings had low overall effect sizesand were not statististically significant.This study offers federal, state, and localagencies a backbone of strong researchto develop crisis intervention programs,including law enforcement.12. Wagner (2005) approached the issue ofCISD effectiveness within the field ofemergency services, including lawenforcement, with a review of literature.Wagner addresses the controversy of268CISD in the field of emergency mentalhealth and implied an increased need forcritical evaluation of relevant literature,specifically in reference to theapplication of CISD to specializedpopulations (e.g., emergency serviceworkers). The overall conclusion of thisreview supports the use of CISD;however, the author is rightfully carefulto specify the effectiveness of CISDwhen applied with emergency serviceworkers and as part of a comprehensiveresponse program.Discussion: Practical ScientificSuggestionsThe pattern of disparate findings in the arti cles reviewed above mirrors CISD researchin general (Wagner, 2005; Wessely & Deahl,2003). Specifically, the reports above havemany of the same terminological and researchdesign shortcomings as other CISD investiga tions (Everly, Flannery, & Mitchell, 2000;Everly & Mitchell, 2000). Because in this paperwe focuse on the variable of law enforcementculture, concerns we have identified regardingresearch on CISD with this population areillustrated in Table 2.AssessmentOverlapping Culture Concerns. Althougheach area in Table 2 identifies specific issuesin the research, the overlapping aspect of theseobservations deserves attention. For example,Brief Treatment and Crisis Intervention / 5:3 August 2005
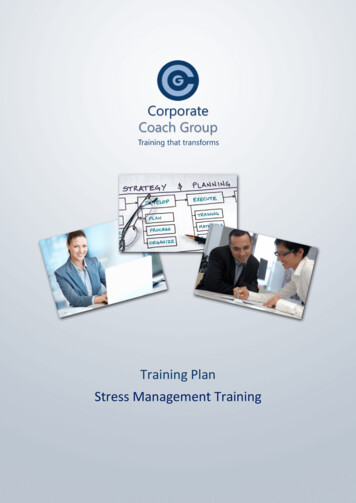
CISD and Law Enforcementconducting research using police officerssustains its own inherent challenges due toshift work, unwillingness to disclose, andlack of validated measurements. An investi gator knowledgeable about police culturewould likely inquire about how methodologywas adjusted for a 24-hr occupation or howresearchers gained access and trust within anygiven department. However, before addressinglaw enforcement culture, psychosocial instru ments used in the studies require scrutiny withregard to their potential threat toward thestrength and validity of their findings.Measurements. One of the critical issues inassessment is balancing objective and sub jective measurements. Police officers mustappear as if they are in control, well-adjusted,and calm. Therefore, a reliance on objectivemeasurements, particularly those which areface valid (e.g., Beck Depression Inventory),will not accurately assess police officer stress.Similarly, dependence on personal interviewsto assess the effectiveness of CISD does notproduce unequivocal results.This lack of useful and valid assessment toolspermeates CISD research in general. Specifi cally, there is an overreliance on self-reportedmeasurements and a lack of objective assess ment (NIMH, 2002). In addition, there isa paucity of evaluation tools validated on policeofficers: a notable exception is the LawEnforcement Officer Stress Survey (LEOSS;Van Hasselt, Sheehan, Sellers, Baker, & Feiner,2003). However, a mixture of measurementsprovides a more well-rounded assessment tobalance out the anticipated ‘‘cop culture’’concerns. It is also important to note that mostvalid assessment devices that measure psycho logical symptoms will not answer questionsabout the perceived effectiveness of CISD. Ifinvestigators intend to examine how CISDaffects particular psychological symptoms,they must employ instruments specific to thesymptoms they are examining (e.g., State-TraitAnger Scale, Beck Depression Inventory).However, if they wish to examine the efficacyof CISD, researchers must be sure to (a) assesswith psychometrically sound instruments and(b) generalize from symptom-specific evalua tion tools (e.g., Robinson and Mitchell, 1993,used a Likert-type scale to measure perceivedeffectiveness; Nurmi, 1999, developed a Per ceived Satisfaction questionnaire). In addition,several of the articles reviewed mentionedoccupational records (e.g., absenteeism, sickand family leave, disciplinary history). How ever, none implied that these type of datareflect the impact of CISD. It is important tonote that one of the primary goals of CISD is toreturn the officer to a premorbid (i.e., pre critical incident) level of functioning, whichincludes getting back to work without man dates or discipline (Wessely & Deahl, 2003).Assessment issues regarding law enforcementand CISD are not strictly police culture con cerns. Indeed, they are relevant to research onCISD in general. However, assessment of lawenforcement carries its own challenges and mustbe addressed when conducting CISD researchwith this population (Sheehan & Van Hasselt,2003). Table 3 outlines suggestions specific tothis problem pulled from previously reviewedstudies.Control Groups. Robinson and Mitchell(1993) discussed the complexity, but under scored the importance, of creating adequatecontrol groups for CISD investigations. MuchCISD research does not have a control conditionthat includes police officers. The lack of suchcontrols makes it difficult to generalize the fa vorable findings of Robinson and Mitchell andof Nurmi (1999) to police officers. In contrast,Smith and de Chesnay (1994) only used policeofficers for the in-depth personal interviews;however, they did not include a control groupto confirm their subjective results.Brief Treatment and Crisis Intervention / 5:3 August 2005269
MALCOLM ET AL.TABLE 3. Suggestions for Clinical Assessment With Law EnforcementResearch-specific suggestionsCop culture-specific suggestions1. A combination of subjective and objectiveassessment tools serves both informative andqualitative purposes1. Face valid instruments should not be used as theonly type of assessment tools within any given study,certainly not with police officers2. The use of a mixed battery of assessment toolsshould be consistently administered throughout thestudy to the same sample, in the same order andunder the same conditions2. The use of record checks (absenteeism, sickleave, family leave) provides some of the most validassessments of police officers response to any givenevent and should be used in combination with otherassessment tools whenever, ethically, possibleCreating adequate control conditions thatethically control the variables of interestbetween groups is problematic. However, thereare basic differences, which, if addressed,would make the experimental control in lawenforcement/CISD research more reliable: (a)increased use of law enforcement officers incontrol groups, (b) improved awareness ofcop culture in the selection of control groupswithin an individual law enforcement agency,and (c) improved attention to departmentaldifferences in the selection of control groupsbetween various law enforcement agencies.For example, many of the articles reviewedhere describe the demographical difference
International Critical Incident Stress Founda tion (ICISF) is composed of these teams. ICISF members are trained to understand the basic physiology and psychology of stress, stress management, and traumatic stress. Knowledge about traumatic stress allows CISM members to facilitate