Transcription
Electronic ASAM Assessmentsfor Substance Use Disorders:Innovative PilotsGary Tsai, MDTina Kim, PhDDesirée Crèvecoeur-MacPhail, PhD*Speakers do NOT have any financial relationship with the ASAM. Dr. Tsai is amember of the American Society of Addiction Medicine (ASAM).
2Outline Framing the Issue Background on the Drug Medi-Cal OrganizedDelivery System (DMC-ODS) Waiver Electronic ASAM Assessment &Screener – An Overview ASAM CONTINUUMTM Pilot ASAM Triage Tool Pilot Summary – Lessons Learned
Polling the Audience How many in here are in the SUD / MH /physical health field? How many people in the room have heard ofthe ASAM Criteria before? How many people have used electronicassessment tools in the past? How many have heard of the ASAMCONTINUUMTM or Triage Tool?53
4FRAMING THE ISSUE:The Drug Medi-CalOrganized DeliverySystem (DMC-ODS)Waiver
5START-ODSSYSTEM TRANSFORMATION TO ADVANCERECOVERY AND TREATMENTLos Angeles County’s Substance Use Disorder Organized Delivery SystemThe Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver, knownlocally as START-ODS, is the greatest opportunity in recent history to designa substance use disorder (SUD) system that has the financial and clinicalresources to more fully address the multifaceted needs of SUD patients.Foundational Principles Patient-centered approach to service delivery Fuller continuum of SUD care aligned with chronic care model of addiction treatment High quality & medically necessary services based on the ASAM Criteria Key Goal Providing the right service, at the right time, for the rightduration, in the right setting Better integrate and coordinate care both within the SUD system and with otherhealth systems (e.g., physical & mental health)
6Self-Referrals &County Stakeholders*Substance Abuse Service Helpline (SASH)-Responsible for initial screening andreferral to SUD provider3. Direct-to-providerSpecialtySUD SystemClient Engagement &Navigation Service (CENS)-SUD assessors and navigators atco-located State, Countyand city sitesSUD Providers-*No wrong door approachResponsible for delivery of SUD servicesCommunication & care coordinationMain Entryways into the Specialty SUD System
7Necessary Changes to the Specialty SUD System Transition from a largely paper-based SUD system to an electronic,technology-based system to help meet the enhanced requirements ofSTART-ODS and align with health industry standards Facilitate greater access to services Clinical documentation Utilization management Data collection Billing Leverage technology to better organize and coordinate services bothwithin the SUD system and between other health systems Sage Electronic Health Record (EHR) for the specialty SUD system Service & Bed Availability Tool (SBAT) web-based service locatoravailable to the general public that serves as a dashboard of availablespecialty SUD treatment services that can be filtered by level of care,available beds, language, service type, and special populations served
8ELECTRONIC ASAMASSESSMENT & SCREENER –AN OVERVIEW
9Electronic ASAM Assessment: ASAM CONTINUUMTM ASAM CONTINUUMTM Software FULL web-based ASAM assessment that covers ALL 6 ASAM dimensions Standardized, computer-guided, structured interview Validated computer algorithm uses information gathered during interviewto confirm medical necessity and appropriate ASAM level of care (LOC), inconjunction with the counselor/LPHA’s clinical opinion 60 – 120 min, depending on the client6 ASAM Dimensions1.2.3.4.5.6.Acute intoxication and/or withdrawalpotentialBiomedical conditions andcomplicationsEmotional, behavioral, or cognitiveconditions and complicationsReadiness to changeRelapse, continued use, or continuedproblem potentialRecovery/living environment
10
11
12Electronic ASAM Screener: ASAM Triage Tool ASAM Triage Tool BRIEF web-based ASAM screener that covers ALL 6 ASAM dimensions Compilation of 20 questions from the ASAM CONTINUUMTM Standardized, computer-guided, structured interview Computer algorithm uses information gathered during interview todetermine an appropriate provisional ASAM LOC, in conjunction with thecounselor/LPHA’s clinical opinion 10 – 20 min, depending on the client Important Note: Assessment tools are only tools. They should augmentbut NOT replace sound clinical judgment by counselors and clinicians
13ASAM Triage Tool
14System Design – Important ConsiderationsClinical Needs Need valid (accurate/reliable), efficient, and feasible ASAMbased tool that performs a comprehensive, multi-dimensionalassessment that considers the whole person (SUD, physicalhealth, mental health, environmental, etc). Use of comprehensive, standardized software that considersdozens of factors when making level of care determinationscan save time and effort, and help to ensurenecessary/appropriate services and address healthdisparities by making level of care recommendation processmore objective and reducing provider and treatment biases.Upfront investments in good assessmentsDownstream efficiencies and improvements
15System Design – Important ConsiderationsClinical Needs (cont’d) Providing SUD care at the appropriate level of care isassociated with better treatment outcomes, whereas underor over-treatment can result in sub-optimal outcomes(Magura et al, 2003). Ultimately, a good SUD assessment should result inimproved SUD and health outcomes.According to prior studies by ASAM (Gastfriend, 2017), comparedto treatment as usual, the ASAM CONTINUUMTM resulted in: 25% - 300% reductions in no shows to next level of treatment 30% reduction in dropout from treatment 3x improvement in addiction severity outcomes at 3 months 25% increase in numbers of patients ready for step-down
16System Design – Important ConsiderationsAdministrative Needs Managed care entities need to review and preauthorize/authorize certainservices.A validated tool that offers LOC recommendations can significantlyreduce the back-and-forth between SUD providers andadministrative entities by providing a LOC standard that both sidescan agree on.Workforce Development Needs Given that SUD counselors comprise 70 – 90% of California’s specialtySUD workforce and focus on SUD during their training, using astandardized, validated, and comprehensive tool such as the ASAMCONTINUUMTM may have the secondary benefit of training counselorson conducting comprehensive biopsychosocial assessments.Training as a Secondary Benefit Over time, the implementation ofa standardized, validated, and comprehensive assessment tool mayupgrade the knowledge of the workforce system wide.
17ASAMTMCONTINUUMPILOT
18Aims of the Pilot Assessment Duration Time requirements Do training or experience make a difference? Satisfaction with ASAM CONTINUUMTM Clinical Knowledge Acquisition Increased knowledge of SUD assessment anddiagnosis principles Level of Care Determination Match between ASAM CONTINUUMTMrecommended LOC & clinical recommendation *Preliminary data is still being analyzed.
19MeasuresMeasuresDescriptionPilot Project QuestionnaireDemographic information, ASAMtraining/assessment experience,Professional status, years ofexperience in SUD treatmentCONTINUUMTM Knowledge PrePost Test15-item test to measure theknowledge of SUD assessment anddiagnosis principlesCONTINUUMTM Satisfaction Survey20-item survey designed to measureattitudes about ASAMCONTINUUMTM utility andsatisfaction
20Participant CharacteristicsParticipantCharacteristicsOverall(n 27)Female14Mean ll(n 27)Professional StatusRegisteredIntern/Counselor6 (22%)Latino/Hispanic14 (52%)Certified Counselor20 (74%)White7 (26%)Licensed Clinician1 (4%)African American3 (11%)Years at Current Job4.3Asian2 (7%)8.4Other1 (4%)Years of Experience inSUD 5 yearsEducation LevelHigh school or less11 ( 41%)5 years and more10 (37%)16 (59%)Associate Degree7 (26%)Training GroupBachelor Degree7 (26%)Trained11 (41%)Master’s Degree1 (4%)Not trained16 (59%)
21ASAMTMCONTINUUMFINDINGSPILOT
2227CounselorsAssessmentsExclusion Criteria Duplicates Assessments completed overmultiple days / 30 or / 400 minutes827493# of Assessments Minimum: 3 Maximum: 59 Average: 18
23Tool Administration DurationMean Time (minutes) to complete theASAM CONTINUUMTM Assessment100809386FirstAssessmentLastAssessmentN 27N 27696040200Overall MeanN 493
24Tool Administration Duration (cont’d)Changes in Mean Time (minutes) to Complete the ASAM CONTINUUMTMAssessment for Trained & Untrained 200TrainedUntrainedN 11First AssessmentN 16Last AssessmentOverall
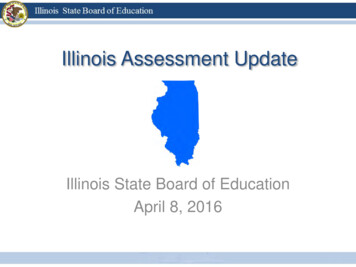
25Association between Practice/Experienceand Assessment Duration# of Assessments byParticipantThe Learning Curve1002001809616080606040Time (minutes)Time (minutes)120140120100806040202000 17N 12318 N 3703 4 5 6 7 9 101415161718192122272931345859
26Satisfaction with ASAM CONTINUUMTMNegative Experience*Positive Experience*KnowledgeacquisitionEasy to collectclient infoASAM trainingwas helpfulEasy to use67%63%58%System problem58%Take away timespeaking to clientNot user friendly54%* Percent of staff that agreed or strongly agreed50%38%
27Focus Group Feedback:Strengths of ASAM CONTINUUMTM Collects a lot of good information Less room for personal biases Seems professional Improved knowledge on assessment Good opportunity for rapport building
28Focus Group Feedback:Improvements to ASAM CONTINUUMTM The inclusion of a narrative report would be helpful The length made it difficult to elicit valid information fromclients Issues with ASAM CONTINUUMTM level of caredetermination Additional topic areas would be helpful: Domestic violence (lifetime experience) The Adverse Childhood Experiences (ACE) Sexual offense (victim or perpetrator) Additional open-ended questions for biopsychosocial
29ASAM TRIAGE TOOLPILOT
30Aims of the Pilot Feasibility of Implementation Level of Care Determination match with ASAMCONTINUUMTM 36 Cases were entered into both the ASAM Triage Tooland the ASAM CONTINUUM systems and comparisonswere made. *Preliminary data is still being analyzed.
31Focus Group Participant CharacteristicsParticipantCharacteristicsOverall(n 27)ParticipantCharacteristicsOverall(n 27)Female19 (70%)Mean Age46 (11.2)RegisteredIntern/Counselor20 (74%)Certified Counselor20 (74%)White2 (7%)Licensed Clinician1 (4%)African American2 (7%)Mean Years at Job8 (6.5)Native American1 (4%)13 (7.5)Other2 (7%)Years of Experience inSUD 5 yearsRace/EthnicityLatino/HispanicEducation LevelHigh school or less1 (4%)Professional Status5 years and moreAssociate Degree17 (64%)Training GroupBachelor Degree7 (26%)TrainedMaster’s Degree 2 (7%)Not trained6 (22%)5 (19%)21 (81%)26 (96%)1 (4%)
32ASAM TRIAGE TOOL PILOTFINDINGS
33ASAM Triage Tool Time Requirements Total triage assessments 873 Total assessors 30 Mean assessments per assessor 29 (sd 34.8) Mean time (minutes) first 10.5 (sd 9.8) Mean time (minutes) last 8.4 (sd 8.7) No significant differences in time betweenfirst triage and last triage (p .096)
34ASAM Triage Tool – Focus GroupFeedbackBenefits Easy to Administer Useful Summary ReportsConcerns Accuracy of the recommended LOC Overriding the LOC Technical glitches / logistical issues
35Focus Group Recommendations Review accuracy of algorithm Add questions on trauma Ensure a paper-based tool is available Provide training and technical assistance
36SUMMARY – LESSONSLEARNED
37Summary – Lessons Learned Given that the ASAM Criteria is also new to many specialtySUD systems, implementing electronic ASAMassessment/screener involves not just getting usersfamiliar with the tools, but with the underlying ASAMCriteria as well TRAINING Overall positive experience with electronic ASAMassessment/screener ASAM CONTINUUMTM Comprehensiveness of the health assessmentStandardization and minimization of potential treatment biasPerceived professionalism of using the toolPerceived administrative benefits from simplified utilizationreview workflow and process ASAM Triage Tool Easy to use and serves its purpose
38Summary – Lessons Learned Refinements in the tools are necessary, particularly with respectto the LOC matching. Recalibrating Cultural Perceptions Part of this also requires educating the general public, as most peoplethink of SUD treatment as being in “rehab for 90 days” and envisionresidential treatment, even when residential treatment may not benecessary Recalibrating the Tools ASAM software algorithm is being adjusted to address the issue ofcases not resolving to any level of care. Other Next Steps ASAM software package being expanded to include a summary report. Single log-in process Accessing the tools will be made easier withstandardized electronic health record (EHR) that will be implementedfor most specialty SUD providers in LA County.
39Summary – Lessons Learned Provider and Administrative Readiness Successful implementation requires time, TRAINING, and a capable IThelp desk. Secure ID token, login/password problems, staff turnover, etc.Important Points of Emphasis As with the use of any assessment tool, it will be easier andquicker to use with time and experience. Assessment tools are only tools and they do NOT replace soundclinical judgment by counselors and clinicians. Balancing the use of a standardized electronic assessment with theneed for clinical flexibility is a learned art, and user judgment shouldALWAYS be involved in the decision-making process.
Discussion / Q&A40
Electronic ASAM Assessment: ASAM CONTINUUMTM ASAM CONTINUUMTM Software FULL web-based ASAM assessment that covers ALL 6 ASAM dimensions Standardized, computer-guided, structured interview Validated computer algorithm uses information gathered during interview to confirm medical necessity and appropriate ASAM level of care (LOC), in