Transcription
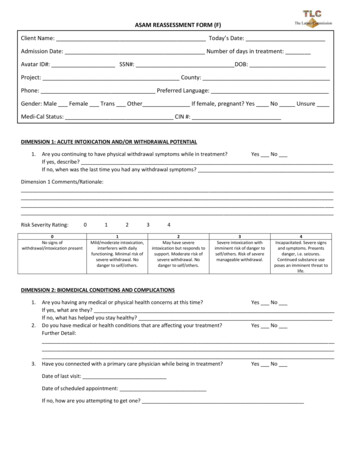
ASAM REASSESSMENT FORM (F)Client Name: Today’s Date:Admission Date: Number of days in treatment:Avatar ID#: SSN#: DOB:Project: County:Phone: Preferred Language:Gender: Male Female Trans Other If female, pregnant? Yes No UnsureMedi-Cal Status: CIN #:DIMENSION 1: ACUTE INTOXICATION AND/OR WITHDRAWAL POTENTIAL1.Are you continuing to have physical withdrawal symptoms while in treatment?Yes NoIf yes, describe?If no, when was the last time you had any withdrawal symptoms?Dimension 1 Comments/Rationale:Risk Severity Rating:0No signs ofwithdrawal/intoxication present0121Mild/moderate intoxication,interferers with dailyfunctioning. Minimal risk ofsevere withdrawal. Nodanger to self/others.342May have severeintoxication but responds tosupport. Moderate risk ofsevere withdrawal. Nodanger to self/others.3Severe intoxication withimminent risk of danger toself/others. Risk of severemanageable withdrawal.4Incapacitated. Severe signsand symptoms. Presentsdanger, i.e. seizures.Continued substance useposes an imminent threat tolife.DIMENSION 2: BIOMEDICAL CONDITIONS AND COMPLICATIONS1.2.3.Are you having any medical or physical health concerns at this time?Yes NoIf yes, what are they?If no, what has helped you stay healthy?Do you have medical or health conditions that are affecting your treatment?Yes NoFurther Detail:Have you connected with a primary care physician while being in treatment?Yes NoDate of last visit:Date of scheduled appointment:If no, how are you attempting to get one?
Dimension 2 Comments/Rationale:Risk Severity Rating:0123401234Fully functional/ able to copewith discomfort or pain.Mild to moderate symptomsinterfering with dailyfunctioning. Adequate abilityto cope with physicaldiscomfort.Some difficulty toleratingphysical problems. Acute,nonlife threatening problemspresent, or seriousbiomedical problems areneglected.Serious medical problemsbeing neglected duringtreatment. Severe medicalproblems present but stable.Poor ability to cope withphysical problems.Incapacitated with severemedical problems.DIMENSION 3: EMOTIONAL, BEHAVIORAL, OR COGNITIVE CONDITIONS AND COMPLICATIONS1.2.Have you ever been diagnosed with a mental health issue?What is your current mental health diagnosis?Yes No3.Are you connected with mental health services?Yes NoIf yes, contact info:If no, how are you attempting to connect and/or how can we help you?4.Are you having any mental health symptoms or emotional distress that is affecting your treatment?Yes No5.Is past abuse or trauma still causing you distress while in treatment?Yes No6.What coping skills have you learned or developed while in treatment to help with your mental health?Dimension 3 Comments/Rationale:Risk Severity Rating:0123401234Good impulse control andcoping skills. Nodangerousness, good socialfunctioning and self-care, nointerference with recovery.Suspect diagnosis of EBC,requires intervention, butdoes not interfere withrecovery. Some relationshipimpairment.Persistent EBC. Symptomsdistract from recovery, butno immediate threat toself/others. Does not preventindependent functioning.Severe EBC, but does notrequire acute level of care.Impulse to harm self orothers, but not dangerous ina 24-hr setting.Severe EBC. Requires acutelevel of care. Exhibits severeand acute life-threateningsymptoms (posing imminentdanger to self/others).
DIMENSION 4: READINESS TO CHANGE1.2.3.What changes have you made while in treatment?What will continue to motivate you or enhance your motivation to stay clean/sober?(Counselor’s observation) Stage of Change:Dimension 4 Comments/Rationale:Risk Severity Rating:0123401234Completely engaged intreatment.Ambivalent of the need tochange.Low commitment to changesubstance use. Passiveengagement in treatment.Unaware of need to change.Unwilling or partially able tofollow through withrecommendations fortreatment.Not willing to change.Unwilling/unable to followthrough with treatmentrecommendationsDIMENSION 5: RELAPSE, CONTINUED USE, OR CONTINUED PROBLEM POTENTIAL1.2.Date of your last use:How often do you have cravings, urges, or thoughts to use? Hourly Daily Weekly None3.4.5.6.Rate your desire to use. 0 No Desire 10 Strongest Desire0 1 2 3 4 5 6 7 8 9 10What are your main triggers at this time, if any?What coping skills have you developed/learned while being in treatment?What support groups or activities do you find helpful to your recovery?Dimension 5 Comments/Rationale:Risk Severity Rating:0123401234Low/no potential for relapse.Good ability to cope.Minimal relapse potential.Some risk, but fair coping andrelapse prevention skills.Impaired recognition of riskfor relapse. Able to selfmanage with prompting.Little recognition of risk forrelapse, poor skills to copewith relapse.No coping skills for relapse/addiction problems.Substance use/behavior,places self/other in imminentdanger.
DIMENSION 6: RECOVERY/LIVING ENVIRONMENT1.2.3.4.What housing options are you currently considering after residential treatment?Are you or will you be responsible for the care of another person(s), including family, children, pets, or others?Yes No If yes, explain:Have you developed a recovery and/or social support network?Yes NoHow do you plan on supporting yourself financially?Dimension 6 Comments/Rationale:Risk Severity Rating:00Able to cope in environment/supportive.121Passive/disinterested socialsupport, but still able tocope.3423Unsupportive environment,but able to cope with clinicalstructure most of the time.Unsupportive environment,difficulty coping even withclinical structure.4Environment toxic/hostile torecovery. Unable to cope andthe environment may pose athreat to safety.Re-Evaluation Disposition (UCLA tracking):Indicated Level of Care (G) Actual Level of care received (J)Recovery Support ServicesASAM 1.0ASAM 2.1ASAM 3.1ASAM 3.3ASAM 3.5ASAM 3.7ASAM 4.0Opioid Treatment Program (OTP)ASAM 1 – WMASAM 3.2 – WMASAM 3.7 – WMASAM 4 – WMOtherRecovery ResidenceMAT Services Recovery Support ServicesASAM 1.0ASAM 2.1ASAM 3.1ASAM 3.3ASAM 3.5ASAM 3.7ASAM 4.0Opioid Treatment Program (OTP)ASAM 1 – WMASAM 3.2 – WMASAM 3.7 – WMASAM 4 – WMOtherRecovery ResidenceMAT ServicesReason for Difference (if any - L):N/A, no differenceClient preferenceFamily ResponsibilityLack of insurance/paymentLevel of Care not avail Clinical JudgementGeographic limitationsLegal IssuesMgnd care refusalCt on waiting list for indicated level Other (M):Language Needs
IF referral being made but admission is expected to be delayed, reason (N): Waiting for LOC availability Waiting for Language specific services Incarceration Hospitalization Other (O):
ASAM 3.7 - WM ASAM 4 - WM Other _ Recovery Residence MAT Services Recovery Support Services ASAM 1.0 ASAM 2.1 ASAM 3.1 ASAM 3.3 ASAM 3.5 ASAM 3.7 ASAM 4.0 Opioid Treatment Program (OTP) ASAM 1 - WM