Transcription
Version 1Health SystemRapid Diagnostic ToolFramework, Operational Guide, and Metricsto Measure the Strength of Priority Health System FunctionsBy David WendtWith contributions from BrunoBouchet, Ya-Shin Lin, LipikaNanda, Shanthi Noriega, NilufarRakhmanova, and Sarah SearlePREPARING FOR THE RAPID DIAGNOSTICi
Table of ContentsForeword. 2Annex 1: Selected References. 39Abbreviations. 3Annex 2: FHI 360 Health System Framework. 411. Introduction. 42. Detailed Guidance on the Steps. 8PHASE I: PREPARING FOR THE RAPID DIAGNOSTIC. 9Step 1) Draft the purpose and scope of the diagnostic. 9Step 2) Gain buy-in and recruit partners. 10Step 3) Recruit a core team. 10Step 4) Locate and review background informationon the health system and health systemstrengthening priorities.13Step 5) Orient the core country team on the RDT.14PHASE II: DESIGN AND PLAN THE RAPID DIAGNOSTIC.15Step 6) Identify which health system functionsto assess.15Step 7) Design the performance metrics.18Step 8) Develop a project work plan, specifyingresponsibilities and deadlines.23PHASE III: GATHER DATA AND ANALYZE HEALTH SYSTEMSTRENGTHS AND WEAKNESSES.25Step 9) Develop a data management system anddata gathering tools.25Step 10) Gather the Data.25Step 11) Analyze health system strengthsand weaknesses. 27PHASE IV: INVESTIGATE THE ROOT CAUSES OFHEALTH SYSTEM WEAKNESSES.29Step 12) Validate the findings from Phase III andidentify priority weaknesses. 30Step 13) Select topics for root cause analysis andgenerate hypotheses of causes. 30Step 14) Collect and analyze evidence on root causes. 30PHASE V: COMMUNICATE THE FINDINGS.34iiStep 15) Devise a communication strategy.34Step 16) Write the report. 37Step 17) Communicate the findings.38Health System Rapid Diagnostic ToolAnnex 3: Rapid Diagnostic Project Participants. 42Annex 4: Self-Assessment Form. 43Annex 5: Common Sources for Data. 44Annex 6: Performance Metrics Table Template. 48Annex 7: Kenya’s Indicator Dashboard. 49Annex 8: Methods for Prioritizing Ideas. 51Annex 9: Illustrative Collection of HealthSystem Functions.52Annex 10: Instructions for the Health SystemGeneric Indicator Tables.56Annex 11: Blank Indicator ConstructionWorksheet.57Annex 12: Example Indicator ConstructionWorksheet for an HSIS Function. 58Annex 13: Generic Performance Indicators forLeadership and Governance. 59Annex 14: Generic Performance Indicators forHealth System Financing.67Annex 15: Generic Performance Indicators forHealth System Information Systems.73Annex 16: Generic Performance Indicatorsfor the Health Workforce. 91Annex 17: Generic Performance Indicatorsfor Health Infrastructure, Equipment, andProducts. 101Annex 18: Generic Performance Indicators forthe Community Component. 110Annex 19: Generic Performance Indicators forService Delivery.115
Health SystemRapid Diagnostic ToolFramework, Operational Guide, and Metrics to Measurethe Strength of Priority Health System FunctionsBy David WendtWith contributions from Bruno Bouchet,Ya-Shin Lin, Lipika Nanda, Shanthi Noriega,Nilufar Rakhmanova, and Sarah Searle2012AcknowledgementsThis tool was developed with funding from the FHI 360 strategic initiative. In addition to the contributors listed on the cover, we would liketo thank: Tim Mastro, Gary West, Megan Averill, Johannes van Dam, Inoussa Kabore, Suzanne Essama-Bibi, Gina Etheridge, and KatherineLew for their support and input on the many drafts; Peter Cowley, Ngak Song, Gautam Barat, Steve Penfold, Nim Nirada, Mena Ly, and NgorSomany and the rest of their team for their hard work pilot testing the tool in Cambodia; Ruth Odhiambo, Linda Muyumbu, Brenda Opanga,Charity Muturi, Francis Waudo Siganga, Stephen Gichuki, Maurice Aluda, Joel Kuria, and the rest of their team for their hard work pilottesting the tool in Kenya; Genevieve d’Entremont for copy editing; and the FHI 360 Design Lab team for the layout.Copyright 2012 Family Health International.FHI 360 is a service mark of Family Health International.
ForewordStrong health systems are critical for achieving lasting results in health. In most low- andmiddle-income countries, issues such as limited numbers of health workers, unreliablesupply chains, inefficient use of resources, and other systemic weaknesses createbottlenecks that make it difficult to achieve results across disease control programs andhealth priorities.To design effective HSS strategies, governments and development partners (such as FHI360) must have solid evidence on health system strengths and weaknesses. Health systemperformance is difficult to define, let alone to measure through a single indicator. Healthsystems have innumerable moving parts, all interrelated and working together to bringabout improvements in the population’s health. Understanding how well these large andcomplex systems are performing their functions remains a priority for researchers andimplementers of public health programs.Although many health system assessment tools exist—focused on particular healthsystem building blocks or across the building blocks—the challenge for users (who maybe working at different levels of the health system or may be focused on different healthobjectives) is how to draw on these existing tools to assess the performance of thosefunctions most related to their context-specific priorities.FHI 360 developed the health system rapid diagnostic tool (RDT) to build the capacity of itspartners in designing their own customized diagnostic of health system performance andinforming local or national health systems strengthening (HSS) strategies. Together, FHI360 and its partners will identify priority health system functions; define performance ofthose functions; design performance metrics; and carry out their diagnostic.This assessment will result in a better understanding of strengths and weaknesses thatstakeholders at national and subnational levels can address through HSS interventions.For any questions or comments about the RDT, please contact the FHI 360 Health SystemStrengthening Department at HSSD@FHI360.org.2Health System Rapid Diagnostic Tool
AbbreviationsABCActivity-Based CostingICTInformation and communication technologyCCTCore country teamIMFInternational Monetary FundCDCUnited States Centers for Disease Controland PreventionKIIKey informant interviewCHeSSCountry health systems surveillance platformL&GLeadership and governanceCPIACountry Policy and Institutional AssessmentLMISLogistics management information systemCSOCivil society organizationLSMSLiving Standards Measurement StudyDDQTDistrict data quality teamM&EMonitoring and evaluationDfIDUnited Kingdom Department forInternational DevelopmentMDGMillennium Development GoalsMOHMinistry of healthMSHManagement Sciences for HealthNHANational Health AccountsNSONational statistics officeOOPOut-of-pocket spendingPAHOPan American Health OrganizationDHMTDistrict health management teamDHSDemographic and Health SurveysDQAData quality auditsDSSDemographic Surveillance SystemFBOFaith based organizationGAVIGlobal Alliance on Vaccines InitiativeGFATMGlobal Fund to Fight AIDS, Tuberculosisand MalariaPEPFAR United States President’s Emergency Planfor AIDS ReliefPHDProvincial health departmentPPPPrivate sector partnerQIQuality improvementRCARoot cause analysisRDTThe FHI 360 Health System Rapid Diagnostic ToolSAMService Availability MappingSCSteering committeeGGHEGeneral government expenditure on healthGHIUnited States Global Health InitiativeHIEPHealth infrastructure, equipment, and productsHISHealth information systemHIV/AIDSHuman immunodeficiency virus/acquiredimmunodeficiency syndromeHMISHealth management information systemSDService deliveryHealth Metrics NetworkSPAService Provision AssessmentHQHeadquartersSRSSample Registration SystemHRHHuman resources for healthTBTuberculosisHRISHuman resources information systemUSAIDHSISHealth system information systemUnited States Agency forInternational DevelopmentHSSHealth systems strengtheningWHOWorld Health OrganizationWHO/EMROWorld Health Organization Regional Officefor the Eastern MediterraneanWHO/SEAROWorld Health Organization Regional Officefor South and East AsiaWHO/WPROWorld Health Organization Regional Officefor the Western PacificHMNHSSD TO FHI 360 Health Systems StrengtheningTechnical OfficerHSSDFHI 360 Health Systems Strengthening UnitICPDInternational Conference on Populationand Development3
14IntroductionHealth System Rapid Diagnostic Tool
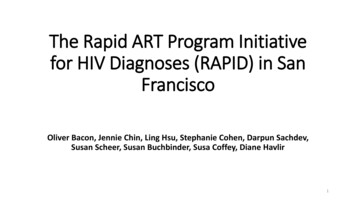
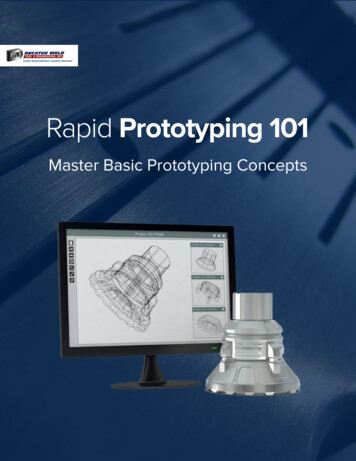
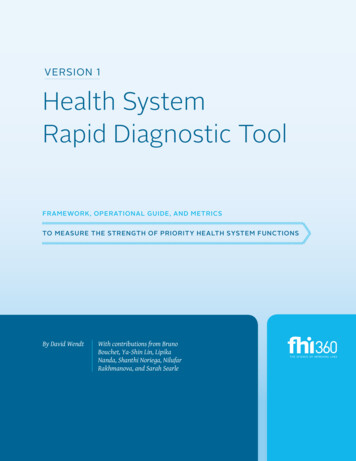
The FHI 360 Health Systems Strengthening (HSS) department developed thisdocument as a “how-to guide” for designing and implementing a customized healthsystem performance diagnostic. To accomplish this customization, this guide putsa heavy emphasis on a country-led design and planning process rather than ablueprint design of a performance diagnostic with a prescriptive (and usually verylong) list of indicators.Users of this guide can focus their diagnostic on theparts most relevant to their context. For instance,district health teams and their partners may findthat a comprehensive, national-level performanceassessment does not produce findings with sufficientdetails that are directly relevant to the specific issues ofa particular district. National assessments may help toset broad system strengthening strategies on a nationallevel, but they may not provide the sub-national levelsof the health system with a foundation of evidenceupon which to act. This guide will help users rapidlydiagnose the performance of those health systemfunctions that are within their scope of action, i.e.,the potential issues they could address with systemsstrengthening interventions.There are two core concepts we refer to throughout thisguide: health system building blocks and health systemfunctions. We use a slightly adapted version of theWHO’s health system building blocks framework (WHO2007) as an overall taxonomy for the major parts of thehealth system. The FHI 360 health system framework(Annex 2) recognizes the community componentas a distinct building block and makes explicit therelationships between building blocks.The concept of “health system functions” refers to thespecific processes performed within each health systembuilding block. For instance, the human resourcesfor health building block can be broken down into anumber of processes, such as: pre-service training,in-service training, establishing staffing norms, settingremuneration levels and conditions (i.e., salaries andother financial and non-financial payments/incentives),hiring, making salary and/or incentive payments,supervising staff, and more. There is not a universaltypology of functions for a health system, and thereforewe used the results of an extensive literature searchand selected key reference documents to develop ourown list (Annex 9) as a starting point for users of theguide to think about the critical functions performed intheir health systems.Improving health system results is the overall aimof health systems strengthening activities, but it isthrough strengthening particular functions that theseimprovements are achieved. Thus, our performancediagnostic approach seeks to uncover which functionsare and are not performing well, which in turn caninform decisions about which functions need to bestrengthened and how to strengthen them.The diagnostic process is organized into five phases,with each phase consisting of a few steps that lead tothe completion of a key output. The final result is adiagnostic that should be the starting point that healthsystem stakeholders and their partners use to designtheir HSS strategy. The steps to this process are outlinedin Figure 1, and the details of each step represent thecontent of this guide. Materials and tools for countryteams to use in this process are provided as annexes.Introduction5
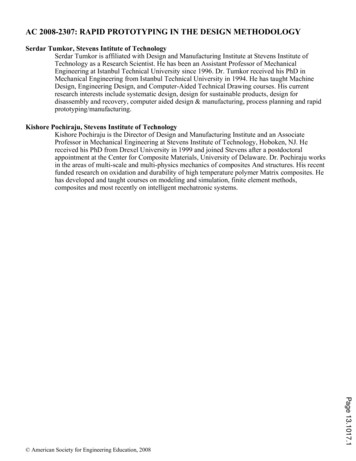
Figure 1:The FHI 360 processfor a diagnosticof priority healthsystem functions’performance** The steps with dotted linesinvolve workshops.Phase IPhase IIPreparationDesign & Planning1.Draft the purposeof the diagnostic2.Gain buy-in andrecruit partners3.Recruit core team4.Review documents5.Orient core teamSteering committeeand core countryteam established6Health System Rapid Diagnostic Tool6.Identify whichhealth systemfunctions to assess7.Design theperformancemetrics8.Develop a work planDiagnostic workplan finalized
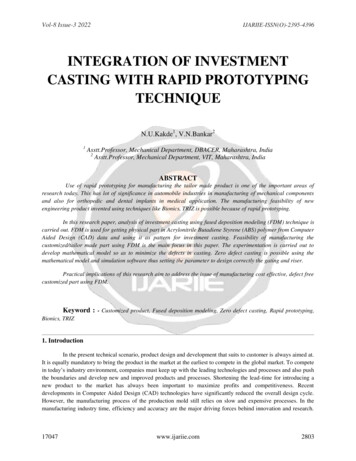
Phase IIIPhase IVPhase VData GatheringRoot Cause AnalysisCommunicate/Apply Findings12. Validate findingsand identify priorityweaknesses15. Develop thecommunicationstrategy10. Gather data13. Generate hypotheseson root causes16. Write thediagnostic report11. Analyze healthsystem strengths& weaknesses14. Collect andanalyze evidenceon root causes17. Communicatefindings9.Design datamanagement systemDiagnosticfindings availableon score cardsRoot causes ofmain weaknessesidentifiedDiagnostic reportcommunicatedIntroduction7
28DetailedGuidance onthe StepsHealth System Rapid Diagnostic Tool
Phase IPhase Istep 1Preparing for therapid diagnosticIn this phase, the initiators of the rapid health systems diagnostic (referred to as the“project initiators” throughout this document) will recruit key project personneland stakeholders and prepare them for designing and implementing the diagnostic.By the end of this phase, a core country team and a steering committee will beestablished and a draft purpose statement will be written.The process of planning and designing the performancediagnostic involves five steps:Step 1) Draft the purpose and scope of the diagnostic.Step 2) Gain buy-in from key stakeholders, andrecruit partners to form a steering committee.Step 3) Recruit personnel to establish a core countryteam (CCT).Step 4) Locate and review background informationon the health system and health systemstrengthening priorities.Step 5) Orient the core country team to the rapiddiagnostic tool (RDT).Step 1) Draft the purpose and scopeof the diagnosticThe first step of the RDT is for the project initiatorsto draft the purpose and scope they envision for thediagnostic. Although this will be reviewed and revisedby the steering committee and CCT members, theproject initiators need to articulate their vision in orderto: a) explain the project to stakeholders and potentialpartners; and b) determine who needs to be involved.Project initiators may want the RDT to focus onparticular levels of the health system, particularpriority health outcomes, and different geographicareas. They also may have different needs for using theRDT. For example, the APHIAPlus program in Kenyaused the RDT to set a baseline for an existing HIV/AIDS program with HSS objectives, whereas the FHI 360office in Cambodia and their provincial governmentpartners used it to explore opportunities for futureHSS programs not related to a specific disease or publichealth program.Defining the unique purpose and scope for the diagnosticis the cornerstone for designing and implementingone suited to the stakeholders’ needs. The purposeand scope will be the foundation for deciding whichstakeholders to involve, which health system functionsto focus on, and which indicators to measure.The purpose and scope need to be established at thevery beginning of the project and must be clear toThe project stakeholders are all those who have an interest inthe findings of the diagnostic. It is up to the project initiators,steering committee, and CCT to determine who among thisbroad group to involve at various stages of the diagnostic.1PREPARING FOR THE RAPID DIAGNOSTIC9
Phase Istep 2-3all participants throughout. This is why the processbegins with the project initiator(s) drafting a purposestatement that reflects the context-specific needs forconducting the diagnostic, as well the appropriatescope (the geographic and topic focus) for thediagnostic given those needs.To draft the purpose statement, project initiatorsshould consider whether future system strengtheninginitiatives will focus on:1.Pre-defined system strengthening objectivesa. If so, the RDT can be used to do a baseline assessmentand gap analysis of the health system functions relatedto these objectives.b. If not, the RDT can be used to explore health systemstrengths, weaknesses, and opportunities.2.Specific disease-focused priorities/objectivesa. If so, the project initiators should state that focus inthe purpose statement so that the steering committeeand CCT design a diagnostic focused on health systemissues linked to those disease priorities (in Step 7).3.A particular level of the health system (national,state, provincial, district, facility), targetgeographic areas, or target populationsa. If so, the project initiators should state this focus inthe purpose statement because it will shape the scopeof the diagnostic and help determine who the keystakeholders are.4.Particular health system building blocksa. If so, the project initiators can state that in thepurpose statement to guide the design process.A final consideration for the purpose is how thefindings will be used. In almost all cases FHI 360 and itspartners will use the findings to design HSS strategies/activities that address underlying root causes of healthsystem weaknesses and have broad and long-lastingeffects on health system outcomes.210We call this group a “steering committee,” but theproject initiators can use another name. The main pointis to have a group of people formally involved in givingdirection and oversight to the diagnostic.Health System Rapid Diagnostic ToolTable 1 provides an example of a purposestatement developed in Kenya and based onthe above considerations.Step 2) Gain buy-in and recruit partnersGovernment, civil society partners, donor agencies,and health system technical experts will all provideinvaluable inputs to the design and implementationof the rapid diagnostic. At the very beginning of theprocess, the project initiators should meet with thesekey stakeholders to discuss the needs for an assessmentand get their buy-in.Although these stakeholders and partners may nothave enough time to be involved in all the phases ofthe diagnostic, their input throughout the process willbe critical to its success. To facilitate their continualinvolvement, the initiators should create a formalmechanism/forum, such as a steering committee.This committee would provide direction and supportto the assessment, but would not be responsible forimplementation. In Table 2 we outline the potentialtiming and content of steering committee meetings.Stakeholder engagement does not end at the steeringcommittee. Those who have more time to commit tothe project and who have the technical capacity can bemembers of the core country team, which is responsiblefor implementing the RDT.Step 3) Recruit a core team3The Core Country TeamImplementing the RDT will require a core team ofpeople who can devote significant time and expertise tothe project. Although specific tasks and deadlines willnot be decided until Step 9 (when the CCT develops theSee Annex 3 for a diagram thatillustrates the relationship betweenthe project initiators, the CCT, thesteering committee, and stakeholders.3
Phase Istep 3Table 1: Purpose and scope of the health system diagnostic in KenyaDesignconsiderationsAPHIAPlusProject 4Implications for thepurpose and scopeAre there existing systemstrengthening objectives?APHIAPlus has 18 existing HSS objectivesAPHIAPlus will use the RDT for a baselineassessment of health system performancerelated to these objectives and to analyzegaps that need to be addressed in futureyears of the program.Will users of the findingsaim to strengthen the healthsystem as a means to achieveparticular health objectivesor outcomes?APHIAPlus aims to strengthen thehealth system to improve deliveryacross many service areas: HTC, HIVCare and Treatment, Maternal Health/PMTCT, Newborn/Child Health, RH/FP,Tuberculosis, Malaria, VMMC.APHIAPlus is interested in HSS that willstrengthen service delivery and outcomesacross priority health areas.Will the diagnostic focuson a particular level of thehealth system, geographicarea, or population?APHIAPlus is focused on Kenya’s RiftValley province.APHIAPlus will be diagnosing healthsystem performance in Rift Valley,engaging provincial-level stakeholders inthe design of the diagnostic, and usingdistricts, facilities, and communities in RiftValley as their units of analysis.Will the diagnostic focuson or leave out particularbuilding blocks?APHIAPlus’s strategic health systemfocus is reflected in its HSS objectives.The existing HSS objectives will be thebasis for deciding which health systemfunctions are and are not priorities.How will findings be used?APHIAPlus will use the findings tomonitor and evaluate improvements insystem performance and to inform thedesign of HSS activities in future annualwork plans.The findings need to inform annualdecision-making and provide a foundationfor evaluating results.Purpose statementand scope:“To establish a baseline on performance of the health system functions related to theAPHIAPlus HSS objectives in the Rift Valley province to: assess constraints to achievingthose objectives; inform the design of HSS activities that address underlying root causesof health system weaknesses and have broad and long-lasting effects on health systemoutcomes; and monitor and evaluate improvements in system performance.”The APHIAPlus Nuru Ya Bonde (NyaB) program is a five-year (January 2011–December 2015)cooperative agreement between FHI 360 and the United States Agency for InternationalDevelopment (USAID). The APHIAPlus NyaB program goal is to improve health outcomes and impactsin the Rift Valley Province of Kenya through sustainable country-led programs and partnerships.The APHIAPlus NyaB program focuses on four areas, namely: 1) health systems strengthening,2) integrated service provision, 3) demand creation, and 4) social determinants of health.4PREPARING FOR THE RAPID DIAGNOSTIC11
Phase Istep 3Table 2: Proposed content for meetings the steering committee will attendMeetingWhenContent of meetingsDesign Workshop #1Phase II –Step 6Initiators present and get input on the diagnostic purpose and scope, andfacilitate a discussion to identify priority health system functions.Steering CommitteeMeeting #1Phase II –Step 8CCT presents and gets feedback on the work plan (which includes theperformance metrics, roles and responsibilities, and project timeline).Data ValidationWorkshopPhase III –Step 12The CCT presents the assessment findings (i.e., the score card analysis of theperformance of the priority functions) and gets feedback on and validation ofthe results. The CCT also facilitates a session to identify which health systemweaknesses to focus on for the root cause analysis.Steering CommitteeMeeting #2Phase IV –Step 14The CCT can present and get feedback on the findings from the rootcause analysis.Draft ReportFeedback MeetingPhase V –Step 17The CCT can present and get feedback on the final report and facilitate adiscussion on the implications of the findings (i.e., the next steps).Table 3: Roles and responsibilities shared among CCT members12RoleResponsible forLeading the projectManaging the team, overseeing the work plan, managing relationships with external partners/stakeholders, and keeping the project on track and on schedule.Organizing meetingsand workshopOrganizing the invitations, location, materials, and other logistics for meetings and workshops.Facilitating meetingsand workshopsLeading agenda design, training and coordinating other facilitators/presenters, facilitatingworkshop sessions, and keeping the workshops and meetings on track and on time.Designing performancemetricsParticipating in identification of: health system functions to assess, critical determinants andeffects of health system performance, performance assessment questions, performanceindicators, and targets for those indicators.Managing dataDeveloping a data management (dashboard) system for the project; entering data into thesystem; generating summary reports/graphs from the data.Collecting dataSearching for data sources, meeting with key stakeholders to get access to data, gatheringtogether key documents and data sets, making site visits to relevant administrative units andfacilities, conducting key informant interviews as required, providing data for entry, identifyingand documenting gaps in data availability, and participating in data validation exercises.Data analysisPreparing the performance scorecards; presenting, discussing, and validating the findings;facilitating root cause analysis; and validating root causes hypotheses.Report writing anddisseminating findingsWriting the report and disseminating findings to key stakeholders.Health System Rapid Diagnostic Tool
Phase Iwork plan), the project initiators will need to outlinethe general roles and responsibilities in order to recruitand orient the team. We have outlined the general rolesand responsibilities in Table 3. CCT members will likelyplay multiple and overlapping roles.The project initiators should recruit the core countryteam (CCT) from FHI 360 country staff and from closegovernment and civil society partners (depending ontheir availability, capacity, and commitment). Workingwith government partners on the CCT will help creategreater ownership and transfer capacity for assessinghealth system performance to the participatingpartner. Such a collaborative partnership requires aclose working relationship, closely aligned objectivesfor the diagnostic (i.e., both parties have similar needsfor learning about health system performance), and asignificant time commitment from the partner, sincethey need to be involved in all phases of the diagnostic.The CCT should include a mix of three to five memberswho bring different skills covering monitoring andevaluation, knowledge about the country’s healthsystem, familiarity with key information sources onthe health system, and strong relationships with keygovernment offices. Annex 4 provides a template to helpidentify members of the CCT based on explicit criteria.When there is limited existing expertise on healthsystems, the FHI 360 country office, should contact theFHI 360 HSS department in the US (HSSD@FHI360.org)to discuss resources and opportunities for increasingthe knowledge and skills of potential team members.For example, the HSS Department developed a series ofshort (45 minute) eLearning courses on health systemsthat can provide the necessary background.Table 3 summarizes the roles and responsibilities ofthe CCT.Technical assistance from the FHI 360headquarters, FHI 360 regional offices,and/or other FHI 360 country officesFHI 360 has significant technical expertise disbursedacross the organization, including prior experienceimplementing health system performance diagnostics.To complement the capacity of the country team, HSSexperts from the FHI 360 HSS Department in the US andstep 4regional or country offices can be called on to providesupport throughout the process. It is particularlyimportant that external support start early during thedesign phase of the diagnostic.For FHI 360 country offices that have not done this sortof assessment before, we recommend a minimum ofone field mission for training the CCT and facilitatingthe design and planning process, followed by distancementoring and, if resources allow, a second mission tofacilitate and support root cause analysis.Step 4) Locate and review backgroundinformation on the healthsystem and health systemstrengthening prioritiesBefore beginning the design and planning of thediagnostic, the project initiators and/or CCT shouldsearch out important background information, such asexisting HSS strategies, past health system assessments,and major health system data sources. Many pastassessments may not have been widely disseminated,so the initiators should meet with key stakeholders andask them whether there are existing assessments orother documents/resources that the project should beaware of.Important background information: Locate existing national and international healthsystem data sets and recent health systemperformance assessments Review national and/or local health str
The diagnostic process is organized into five phases, with each phase consisting of a few steps that lead to the completion of a key output. The final result is a diagnostic that should be the starting point that health system stakeholders and their partners use to design their HSS strategy. The steps to this process are outlined