Transcription
Pharmacists Provision of PEP and PrEP:A Primer for Senate Bill-159 (Weiner)Presented by:Jim Scott, PharmDChristina Madison, PharmDJerika Lam, PharmDMonica Donnelley, PharmDJennifer Cocohoba, PharmD
Pharmacist Provision of PEP and PrEP:A Primer for Senate Bill (SB)-159 (Weiner)OUTLINE REVIEW OF HIV BASICS TESTING FOR HIV REVIEW OF ANTIRETROVIRALSCOUNSELING PATIENTS ON SEXUAL HEALTHPEP GUIDELINESPREP GUIDELINESCOUNSELING PATIENTS ON ADHERENCEFINANCIAL AND OTHER RESOURCESACPE ACCREDITEDThis program meets the CA Board ofPharmacy requirements for pharmaciststo furnish PEP/PrEP under Business andProfessions Code 4052.02, 4052.03, andTitle 16 Section 1747Participants must complete this trainingprogram and pass the quiz at the end ofthe program to receive the certificate ofcompletion and CPE credit2
Program Speakers/Faculty James (Jim) D. Scott,PharmD, APh, FCSHP,FASHP, FCCP, AAHIVP Professor Associate Dean Western University of Health Sciences Monica Donnelley PharmD,BCIDP, BCPS AQ-ID, AAHIVP Infectious Diseases Specialist, UC Davis HealthAssistant Clinical Professor Touro University College of Pharmacy Christina M. Madison,PharmD, FCCP, AAHIVP Founder, The Public Health PharmacistAssociate Professor of Pharmacy Practice Roseman University of Health Sciences Jerika T. Lam, PharmD, APh,AAHIVP, FCSHP Associate Professor Chapman University School of Pharmacy Jennifer Cocohoba, PharmD,AAHIVP, BCPS, FCSHP, APh Professor of Clinical Pharmacy UCSF School of Pharmacy3
Disclosures Jim Scott, PharmD I have no conflicts of interest to discloseJennifer Cocohoba, PharmD I am pending receipt of an investigator-initiated research grant from ViivHealthcare Christina M. Madison, PharmD I have the following to disclose: Speaker bureau for Gilead Sciences (HIVPrevention) and Janssen Therapeutics (HIV Treatment) Jerika T. Lam, PharmD I have no conflicts of interest to disclose Monica Donnelley, PharmD I have no conflicts of interest to disclose4
Learning Objectives AT THE END OF THIS SESSION, THE ATTENDEE WILL BE ABLE TO: Explain HIV and its treatment to patientsTake a culturally competent sexual history/risk assessmentManage PEP for a variety of patientsManage PrEP for a variety of patientsExplain the importance of PEP/PrEP adherence to patientsDescribe PEP/PrEP funding and financial assistance5
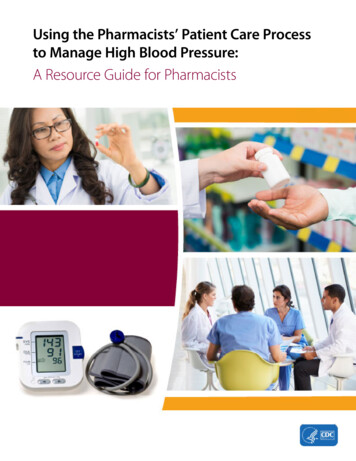
SB 159 (Weiner): HIV Prevention SB 159 authored by Sen. Weiner was signed into law on 10/7/19. CSHP was one of multiple co-sponsors of SB 159The law amended the Business and Professions Code to allowpharmacists to “furnish” PEP and PrEP only after the CA Board ofPharmacy developed “emergency” regulations setting forth thetraining requirements for pharmacists to “furnish”. Effective 4/30/20 - Title 16, CA Code of Regulations, Section 1747 wasadded setting forth the training requirements for pharmacists tofurnish PEP and PrEP.Participants must pass quiz with 70% and maintain record of trainingfor 4 yrs. Senate Bill No. 159, CHAPTER 532: An act to amend Section 4052 of, and to add Sections 4052.02 and4052.03 to, the Business and Professions Code, to add Section 1342.74 to the Health and Safety Code,to add Section 10123.1933 to the Insurance Code, and to amend Section 14132.968 of the Welfare andInstitutions Code, relating to HIV prevention. Title 16 CCR Section 1747:https://pharmacy.ca.gov/laws regs/approved regs.shtml6
SB 159 (Weiner): HIV Prevention A pharmacist must complete training either approved by the CA Board ofPharmacy or is provided by a provider accredited by an approvedaccreditation agency. CSHP is an ACPE accredited provider and this training qualifies a pharmacist tofurnish PEP and PrEP upon successful completion.SB 159 provides authority for a pharmacist to determine if patients meetclinical criteria for PEP or PrEP. Allows them to; furnish 30 or 60 days of PrEP once every 2 years; orfurnish 28 days of PEP; andThey must inform the patients primary care provider or provide the patient with asimilar report that would have gone to their provider.7
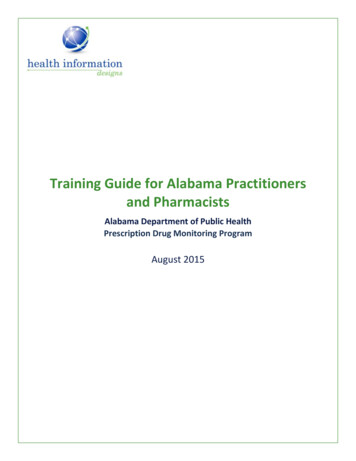
Stage 3 (AIDS) Classifications, Deaths, and Persons Living withDiagnosed HIV Infection Ever Classified as Stage 3 (AIDS),1985–2018—United States and 6 Dependent AreasNote. Deaths of persons with HIV infection, stage 3 (AIDS) may be due to any s/cdc-hiv-infection-trends-stage3-2018.pptx
HIV 101James (Jim) D. Scott, PharmD, APh, FCSHP,FASHP, FCCP, AAHIVP9
HIV Lifecycle,with ARVaction s/fact-sheets/19/73/the-hiv-lifecycle10#. On-slide citation, abbreviated.
HIV Lifecycle,with ARVaction s/fact-sheets/19/73/the-hiv-lifecycle11
Natural History of HIV Infection Stages of Disease Progression Acute infection (early immune depletion) Clinical latency (intermediate immune depletion) AIDS (severe immune .html
ct-sheets/19/46/the-stages-of-hiv-infection13
14
Primary HIV Infection and Seroconversion Initially there is a 2 to 4-week period of intense viralreplication before the onset of an immune response andclinical illness Acute illness lasts about 1-2 weeks and is often notrecognized (flu-like syndrome) Clinical manifestations resolve as antibodies to the virusbecome detectable in serum Patients then enter a stage of asymptomatic infectionlasting months to aids
Acute Retroviral Syndrome Non-specific ‘flu-like’ symptoms FeverFatiguePharyngitisLymphadenopathyRash Burst of viral replication results in intense viremia Window -aids
Window Period The period when infection has just occurred, until the timewhen antibodies are first detectable in the serum Patient is very infectious Virologic measures (NAT/Viral Load) can diagnose thepatient Rapid test is negative ELISA/Antibody is iv-aids
Clinical Latency At CD4 cell counts 500 cells/ml, many complicationsoverlap with conditions found in the general population malaria, bacterial pneumonia, tuberculosis, minor skinconditions They may be more frequent in HIV infected patients At CD4 counts between 200 and 500 cells/ml, otherconditions, or opportunistic infections, begin to appear(Kaposi’s sarcoma, oral or vaginal candidiasis, herpes zoster,etc s
AIDS Manifestations: Adults CD4 cell count 200 cells/ml Wasting syndrome (systemic) Esophageal candidiasis (upper GI tract) Atypical and extrapulmonary TB (pulmonary/other systems) Pneumocystis pneumonia (pulmonary) Recurrent invasive herpes simplex virus infections (skin) CD4 cell count 50 cells/ml Cryptococcal meningitis (CNS) Cryptosporidiosis (GI Tract) Toxoplasmosis (CNS) HIV encephalopathy (or PML or dementia) CMV retinitis (eyes, other v-aids
Complications of HIV by CD4 Count1000CD4Count500200500 Bacterial PneumoniaTuberculosisCervical DysplasiaHerpes Zoster (Shingles) Kaposi’s Sarcoma Thrush/Vaginal Candidiasis Lymphoma Histoplasmosis Pneumocystis Pneumonia Toxoplasmosis Esophageal Candidiasis Cytomegalovirus (CMV) Mycobacterium Avium Complex ds20
Consequence of HIV infection Depletion of CD4 T lymphocytes Depressed cell mediated immune response with impairedkilling of pathogens leading to occurrence of ds
HIV Testing22
HIV TestingThree methods to test for HIV Nucleic Acid Test (HIV Viral Load) Provides an approximate count of the virus per millimeter of blood Minimum level of detection 20copies/mL Can be in the millions of copies/mL Very costly, not commonly performed for routine screening purposes Typically reserved for suspected acute retroviral syndrome (as part of thecare of a prescriber), or as part of the routine care of someone known to beHIV 23https://www.cdc.gov/hiv/basics/testing.html
HIV TestingThree methods to test for HIV Antigen/Antibody test Looks for antigens (sections of viral protein) and antibodies to the virus Common as a confirmatory test for HIV Commonly requires a venous blood draw and a “send-out” lab analysis Results take a few days Not practical for pharmacy and many clinic practices Also available as a rapid test24https://www.cdc.gov/hiv/basics/testing.html
HIV TestingThree methods to test for HIV Antigen/Antibody RAPID test Looks for antigens (sections of viral protein) and antibodies to the virus Finger-prick blood test Results available in 30 ml
HIV TestingThree methods to test for HIV Oral Antibody test Looks for antibodies to the virus that are expressed in saliva Oral swab test Results available in 20-40 minutes Most common for point of care and rapid testing locations Pharmacies High-volume public clinics HIV/STI testing centers (stationary and 26
HIV TestingInterpretation of tests NAT (HIV Viral Load) and Antigen tests If positive – patient is infected If negative – interpretation depends on last high-risk exposure 1 month – most likely negative 1 month – probably not infected, but retest after 1-3 months to ml
HIV TestingInterpretation of tests Antibody tests If positive – patient is infected If negative – interpretation depends on last high-risk exposure 6 months prior – most likely negative 6 month – indeterminate, retest after 3 & 6 months It takes time for the body to develop antibodies Patient counseling regarding sexual history is important in interpretingHIV antibody tests28https://www.cdc.gov/hiv/basics/testing.html
HIV TestingOral Antibody test Oral antibody tests Need a CLIA waiver Use universal precautions (wear gloves, maybe mask, clean afterwards withdisinfectant) even though low risk Swab testing pad between cheek and gum, rub to moisten Place testing pad in buffer Interpret l
ARVs 10130
Available AntiretroviralsNucleoside Reverse Transcriptase Inhibitors (NRTIs)NRTI’s blockreversetranscriptase, anenzyme HIV needsto make copies ofitself.Abacavir(abacavir sulfate, ABC)ZiagenDecember 17, 1998Emtricitabine(FTC)EmtrivaJuly 2, 2003Lamivudine(3TC)EpivirNovember 17,1995Tenofovir disoproxil fumarate(TDF)VireadOctober 26, 2001Tenofovir alafenamide(TAF)VemlidyNovember 10, 2016Zidovudine(AZT, ZDV)RetrovirMarch 19, 1987 NRTIs have been a mainstay of HIV treatment since 1987Older, less-well tolerated options are not commonly s/fact-sheets/19/58/fda-approved-hiv-medicines31
Available AntiretroviralsNon-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs)NNRTIs bind to, andlater alter, reversetranscriptase Doravirine(DOR)PifeltroAugust 20, 2018Efavirenz(EFV)SustivaSeptember 17, 1998Etravirine(ETR)IntelenceJanuary 18,2008Nevirapine(NVP)ViramuneJune 21, 1996Viramune XRMarch 25, 2011Rilpivirine(RPV)EdurantMay 20, 2011NNRTIs were commonly used, but less so nowNot recommended for 32
Available AntiretroviralsProtease Inhibitors (Pis)PIS block HIVprotease, anenzyme HIV needsto make copies ofitself. Atavanavir (ATV)ReyatazJune 20, 2003Darunavir (DRV)PrezistaJune 23, 2006Fosamprenavir (FPV)LexivaOctober 20, 2003Ritonavir (RTV)*NorvirMarch 1, 1996Saquinavir (SQV)InviraseDecember 6, 1995Tipranavir (TPV)AptivusJune22, 2005*Although ritonaviris a PI, it isgenerally used as apharmacokineticenhancer in variousHIV treatmentguidelinesPI’s were an essential part of shifting the treatment curve in HIV careLess commonly used now due to tolerability and efficacy compared to ISTI’sDrug interactions still an area for 3
Available AntiretroviralsIntegrase Strand-Transfer InhibitorsIntegrase inhibitors blockHIV integrase, an enzymeHIV needs to make copiesof itself.Dolutegravir (DTG)TivicayRaltegravir (RAL)Isentress/Isentress HDElvitegravir OBI/FTC/TDF)Bictegravir (BIC) Biktarvy (BIC/FTC/TAF)Preferred agents now due to efficacy and tolerabilityand available once-daily combination 34
Counseling patients onSTIs and Sexual HistoryChristina M. Madison, PharmD, FCCP, AAHIVP35
Taking A Sexual History More than one million people who are at riskfor HIV in the United States could benefit frompre-exposure prophylaxis (PrEP) medications Only a fraction receive HIV preventionservices Taking a sexual history is an essential part ofthe HIV prevention assessment In a survey of 500 men and women 25 andolder 85% of respondents expressed an interest in talkingto their providers about sexual concerns Although 71% thought their provider would likelydismiss their concerns36National LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking Routine Histories ofSexual Health: A System-Wide Approach for Health Centers. Accessed May 10th, 2020Marwick C. Survey says patients expect little physician help on sex. JAMA. 1999;281:2173-4.
Taking A Sexual History Assessing Risk of Sexual Transmission of HIV Assess all sexually active patients for diagnoses of bacterial SexuallyTransmitted Infections (STIs) ChlamydiaGonorrheaSyphilis Routine testing is recommended using 3 site STI testing (including oralpharyngeal and rectal samples) Assess for STIs every 3 months and Test for STIs every 6 months Epidemiologic context of reported sexual practices should be considered Consider the likelihood a sexual partner has HIV infection (geographic location) If sexual partner is HIV positive, are they receiving ART? Are they adherent? Are they your only sex partner?37CDC PrEP Guidelines. 2017
Taking A Sexual History You will be taking histories from diverse patients fromdifferent racial, ethnic, and socioeconomic background Assess all patients for alcohol abuse, especially beforesexual activity, and use of illicit non-injection drugs Refer persons reporting substance abuse to appropriatetreatment or harm-reduction services Consideration should be made for the needs of theLGBTQ community Increased risk for HIV and sexually transmitted infectionsare two of many health disparities that disproportionatelyimpact this communityEspecially women of trans experience and in particulartrans women of color38National LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking Routine Histories ofSexual Health: A System-Wide Approach for Health Centers. Accessed May 10th, 2020
Taking A Sexual History Taking a culturally competent sexualhistory is an essential component of theHIV prevention assessment Knowing the sexual practices and partnersof your patient helps to determine risk andallows you the provider to give effectiveharm reduction strategies Making your patient feel as comfortable aspossible is key to allowing them to disclosesensitivity information confidentially in ajudgement free space39National LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking Routine Histories ofSexual Health: A System-Wide Approach for Health Centers. Accessed May 10th, 2020
SET THE STAGE Bring up the sexual history as part of the overall historyExplain that you ask these questions of all patientsEnsure confidentialityBEGIN WITH THREE SCREENING QUESTIONS1.2.3.Have you been sexually active in the past year?Do you have sex with men, women, or both?How many people have you had sex within the past year?MULTIPLEPARTNERS, NEWPARTNERAsk about STD/HIV protectionPartnersSubstance useHistory of STDsTrauma/violencePregnancy plans/protectionSexual function/satisfactionOther concernsLONG-TERMMONOGAMOUSPARTNERAsk about Pregnancyplans/protection Trauma/violence Sexual function andsatisfaction Other concernsNOT SEXUALLYACTIVEAlgorithm forConducting aSexualHistoryAsk about Past partners (ifpatient is new) Any questions orconcernsFOLLOW-UP AS APPROPRIATE(e.g., STD & HIV testing, counseling & education, ontent/uploads/COM-827-sexual-history toolkit 2015.pdf40 ofNational LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking Routine HistoriesthSexual Health: A System-Wide Approach for Health Centers. Accessed May 10 , 2020
Taking A Sexual History Ensure that your patient knows thatyou ask these questions of all yourpatientsTaking a sexual history is part of thepatient's overall health assessmentConducting a sexual history followedby targeted discussion about ways tostay healthy can enhance the patientprovider relationshipMake sure that you reserve a privatespace in your pharmacy in order toconfidentially conduct your interview41National LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking Routine Histories ofSexual Health: A System-Wide Approach for Health Centers. Accessed May 10th, 2020
Sexual Risk ontent/uploads/COM-827-sexual-history toolkit 2015.pdf42National LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking Routine Histories ofSexual Health: A System-Wide Approach for Health Centers. Accessed May 10th, 2020
CDC –Taking SexualHistory.pdfU.S. Centers for Disease Control and Prevention. A Guide to Taking a Sexual History. Accessed May 10th, 2020.
Taking a Sexual History Aids Education and Training Centers (AETC) SexualHistory Taking Toolkit Developed a comprehensive sexual history template toassess the potential health risk s associated with anindividual’s sexual history and ory-taking-toolkitThis document includes information about Sexual orientation and gender identity (SOGI) dataTypes of partners and encountersRisky sexual behaviors such as exchanging sex for moneyor drugsSubstance use or abuseSexual assault or intimate partner violenceWhere partners are being found (online or in real life)History of STI testing/treatmentHIV status and status of partnersContraception and desire to become pregnant44Aids Education and Training Centers (AETC) Sexual History Taking Toolkit. Comprehensive SexualHistory Template. g-toolkit Accessed May 13th, 2020
Sexual tional LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking RoutineHistories of Sexual Health: A System-Wide Approach for Health Centers. Accessed May 10th, 2020
Sexual tional LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking RoutineHistories of Sexual Health: A System-Wide Approach for Health Centers. Accessed May 10th, 2020
Sexual tional LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking RoutineHistories of Sexual Health: A System-Wide Approach for Health Centers. Accessed May 10th, 2020
Sexual ady, Set, PrEP is a key component of the Ending the HIV Epidemic: A Plan for America (EHE) Accessed May 13th, 2020
Best Practices Taking a culturally competent and comprehensive sexual history is thefoundation to providing optimal HIV prevention care servicesEstablishing a report with you patient and setting the stage toconducting these sensitivity conversations is keyRemember the 5 “P” when taking a sexual historyEmphasizing the need for “good” sexual health and the importance ofknowing the HIV and sexual health status of your sexual partnersHarm Reduction Strategies Encourage safe injection practices and supply clean needles if neededOffer condoms and encourage correct and consistent condom usePrEP and PEP care help decrease your risk of getting HIV Ready, Set, PrEP is a key component of the Ending the HIV Epidemic: A Plan for America (EHE) Accessed May 13th, 2020 National LGBT Health Education Center and National Association of Community Health Centers. (2015). Taking Routine Histories of Sexual Health: A System-Wide Approach for HealthCenters. Accessed May 10th, 2020 Marwick C. Survey says patients expect little physician help on sex. JAMA. 1999;281:2173-4. U.S. Centers for Disease Control and Prevention. A Guide to Taking a Sexual History. Accessed May 10th, 2020. Aids Education and Training Centers (AETC) Sexual History Taking Toolkit. Comprehensive Sexual History Template. g-toolkit Accessed May13th, 202049
Guidelines for PEPJerika T. Lam, PharmD, APh, AAHIVP, FCSHP50
Post-Exposure Prophylaxis (PEP)HIV antiretroviral treatment given after a potentialexposure to HIV Infectious fluid and portal of entryTo PEP or not to PEP Source patient factors (known positive, or high-risk populationmember) Exposed patient’s factors (nature of injury, comorbid conditions)Categories of exposure Occupational and non-occupational (aka nPEP, NonoPEP, sexPEP)51
Types of Exposure: OccupationalTypes Mucous membrane splash PercutaneousPotential increased risk with Deep stick Hollow bore (needle) Visibly bloody Known HIV positive source Viral workers.html
Types of Non-Occupational ExposureExposureRate for HIV acquisition(per 1000 exposures)Receptive anal intercourse13.8Receptive penile-vaginal intercourse0.8Insertive anal intercourse1.1Insertive penile-vaginal intercourse0.4Receptive or insertive oral intercourseLowBiting, spitting, throwing body fluids,sharing sex esources/cdc-hiv-npep-guidelines.pdf53
Timeframe of Exposure Most effective when initiated assoon as possible after exposure Less likely to be effective 72hours (animal models) Impact on decision making Anxiety provoking, time pressure Can also start and discontinue ifinformation is available about thesource54
Assessing The Source PatientKnown source, known statusKnown source, unknown statusUnknown source, unknown statusExample: needlestick when drawingblood from a known HIV patientExample: sex with new partnerExample: needlestick from foundneedle in parkExample: breastmilk splash to eyesfrom post-partum woman who testednegative and has no ongoing riskfactorsExample: Needlestick from patientwhose status is not knownExample: slipped and fell in bloodyvomitusTypically recommend PEP forsignificant exposures to known HIV source patientsObtain history and baseline testing ifpossiblePEP typically not recommended forunknown source unless in a setting thathas high prevalence for HIV (e.g.,needlestick from a needle in HIV clinic)No PEP for known HIV(-) sourceWeigh risk factors (source risk factorsfor acquiring HIV, community riskfactors) for PEP decision55
Preferred HIV PEP Regimen* Adults and adolescents aged 13 yo, including pregnant women Duration 28 daysDrug ADrug BWith normal renal function (CrCl 60 mL/min)Raltegravir (Isentress ) 400 mg PO BID, ORDolutegravir (Tivicay ) 50 mg PO dailyTenofovir DF 300 mg/emtricitabine 200mg (Truvada ) PO dailyWith renal dysfunction (CrCl 59 mL/min)Raltegravir (Isentress ) 400 mg PO BID, ORDolutegravir (Tivicay ) 50 mg PO dailyZidovudine and lamivudine (doseadjusted)*SB 159 allows for new PEP regimens to be included in guidelines in the future.56Lennox JL, et al. Lancet. 2009;74(9692):796-806.Kuhar DT, et al. Infect Control Hosp Epidemiol. 2013;34:875-892.
Safety and Tolerability of Once Daily B/F/TAF for PEPFenway Health – Boston, MAInterim analysis of a prospective open-label trial ofB/F/TAF for 28-day PEP in eligible* patients (N 48)Demographics: Median age 32Race/ethnicity: 79% White, 4% Black, 8%Hispanic/Latinx88% cisgender gay or bi menResults: Most commonly reported AEs:o Nausea /- vomiting (15%)o Fatigue (6%)o Diarrhea (6%) Lab changes did not lead to discontinuation andreverted to normal levels after completion of regimen.There were no HIV seroconversions in the studyRegimen Completion Rates Among B/F/TAF Usersvs. Historical INSTI-based PEP Regimens at Fenway, 2008-2020F/TDF RAL(N 100)%E/C/F/TDF(N 100)%B/F/TAF(N 48)%Completedas prescribed57**71‡85.4Stopped ormodified28†1510.4Lost tofollow-up15‡144.2B/F/TAF for PEP was well-tolerated and resulted in higher completion ratescompared to other INSTI-based PEP regimensB/F/TAF is not FDA approved for PEP indication*Present for PEP within 72 hours of a high-risk exposure per CDC guidelines; **p 0.001; †p 0.01; ‡p 0.05; B/F/TAF, bictegravir/emtricitabine/tenofoviralafenamide; PEP, post-exposure prophylaxis; AEs, adverse events; F/TDF, emtricitabine/tenofovir disoproxil fumarate; RAL, raltegravir; nofovir disoproxil fumarateMayer K, et al. CROI 2020 Boston, MA. 99657
Alternative HIV PEP Regimen Adults and adolescents aged 13 yo, including pregnant women Duration 28 daysDrug ADrug BWith normal renal function (CrCl 60 mL/min)Darunavir (Prezista ) 800 mg POTenofovir DF 300 mg/emtricitabinedaily ritonavir 100 mg PO daily200 mg (Truvada ) PO dailyWith renal dysfunction (CrCl 59 mL/min)Darunavir (Prezista ) 800 mg POdaily ritonavir 100 mg PO dailyLennox JL, et al. Lancet. 2009;74(9692):796-806.Kuhar DT, et al. Infect Control Hosp Epidemiol. 2013;34:875-892.Zidovudine and lamivudine (doseadjusted)58
Baseline EvaluationLaboratory studies HIV testing CBC, renal and hepatic tests If indicated: pregnancy, HBV and HCVCounseling (at the time of exposure and at follow-upappts) Advise patient to use precautions to prevent secondary transmission,especially during the first 6-12 weeks after exposureCounseling when PEP is prescribed Possible drug adverse effects or toxicities Possible drug interactions Adherence to PEP regimen59
TestBaseline4-6 weeks afterexposure3 months afterexposure6 months afterexposureFor all persons considered for or prescribed PEP from any exposureHIV-1/2 Ag/Ab Immunoassay Hepatitis B serology (HBsAg, antiHBs, anti-HBc) ------ *Hepatitis C antibody ------ *For all persons considered for or prescribed PEP from sexual exposureSyphilis serology --- Gonorrhea †------Chlamydia †------Pregnancy ‡ ‡------Complete blood count ------Serum creatinine & transaminases ------For all persons with HIV infection confirmed at any visitHIV RNA level HIV RNA drug resistance *If exposed person susceptible at baseline‡For female persons†If symptomatic at follow-up visit60
DrugMetabolismDDIADRsIntegrase Strand Transfer Inhibitors (INSTI)Raltegravir(Isentress )UGT1A1RifampinDiarrhea, nausea andheadacheDolutegravir(Tivicay )UGT1A1, CYP3A4OCT2 inhibitorRifampin, CYP3A4 inducers;polyvalent cationsHeadache, insomnia,some CNS effectsProtease Inhibitors (PI)Darunavir(Prezista )CYP3A4 substrate;CYP3A4 inhibitorCYP3A4 and 2D6Ritonavir (Norvir ) substrate; CYP3A4inhibitorNausea, diarrhea,headache, rash (rare)CYP3A4 inhibitors andinducersNausea, diarrhea,headache, taste sensealtered, rash (rare)Nucleoside Reverse Transcriptase Inhibitor (NRTI)Tenofovir DF/FTC(Truvada )RenalTDF: substrate of P-gp andBCRP61Nausea, headache
When to Obtain Expert Consultation for PEP? Delay of 72 hours from exposure to evaluationUnknown source (e.g., needle in sharps disposal containeror laundry, source patient declines HIV testing)The source person has known or suspected ARV drugresistanceIndividual exposed to HIV is pregnant or breastfeedingSerious medical illness in the exposed individualDevelopment of toxicity of the initial PEP regimen62
PEP Expert Consultation Resource National Clinician Consultation Center’s Post-ExposureProphylaxis PEPline: (888) 448-4911 Hours: 8 am – 5 pm, 7 days a week Callers need to unblock their phone prior to calling the PEPline Website: http://nccc.ucsf.edu/63
Education Provided The patient may not waive consultation for pharmacistfurnished PEP Adherence to PEP Side effects STI prevention Importance of testing and treatment Availability of PrEP for those who are at substantial risk ofacquiring HIV64
Transitioning from nPEP to PrEP Many individuals who present for nPEP may be excellentcandidates for PrEP, especially if they have ongoing activitiesassociated with increased risk for HIV acquisition Individuals who have completed the 28-day course of nPEPshould be evaluated for transitioning to PrEP if: They have repeatedly sought nPEP They have frequent, recurrent exposures to HIV that would requiresequential or near-continuous courses of nPEP Documentation of HIV-negative status should be obtained beforeadministering PrEP (preferably several days prior to completingthe nPEP course) Transition from nPEP to PrEP should be done immediately65CDC: US DHHS; 2016. US Public Health Service. A Clinical Practice Guideline. March 2018:1-77.
Follow-up After PEPPharmacist must notify the patient’s primarycare provider(PCP) that they complete therequirements for PEP and provided themedicationIf patient has no PCP, or doesnot consent to have PCPnotified: Pharmacist mustprovide a lis
6 SB 159 (Weiner): HIV Prevention SB 159 authored by Sen. Weiner was signed into law on 10/7/19. CSHP was one of multiple co-sponsors of SB 159 The law amended the Business and Professions Code to allow pharmacists to furnish PEP and PrEP only after the A oard of Pharmacy developed emergency regulations setting forth the