Transcription
MEDICAL/PRESCRIPTIONSISC PLAN CHANGES AND REMINDERSEffective 10/1/2022The No Surprises ActOn December2020, the No surprises Act was passed into law. This new legislationprotects patients from surprise medical bills starting in 2022. Surprise medical bills canarise in the following situations: In an emergency when the patient has no ability to select the facility or providerrendering services. When a patient receives planned care at an in-network facility but later finds out that aprovider who treated the patient, such as a radiologist or pathologist, is out-of-network.11th,PPO PlansCHANGES: New Maven Maternity Care Benefit for SISC PPO Member. Maven offers 24/7 virtualaccess to one-on-one maternity and postpartum support. SISC PPO Members whomeet the criteria will get a free 6 month diaper subscription. SISC will be transitioning to digital ID cards at some point next year. HSA – A Family Deductible will change from 2800 to 3000 effective 01/01/2023REMINDERS/NOTES: Effective 10/1/2020, all Non-HSA PPO plans will feature 0 copays for the first threeprimary care visits each calendar year. HINGE Health offers innovate non-surgical digital programs for back, knee, hip, neck,or shoulder pain. See attached flyer. Co-pays may apply to MD Live. Temecula Valley Hospital is now a Blue Distinction Facility for Hip and Kneereplacement surgery. Both medical and prescription deductibles, if satisfied during the last quarter (OctoberDecember), roll over to the new medical deductible year (January-September 30)(excludes the Anchor Bronze plan and HSA plan). Most generic prescriptions are 0 copay at Costco pharmacies. It is your responsibility to make sure your provider and facilities are contractedBEFORE services are rendered. Carrum Health provides PPO members with access to an enhanced benefit with selectedphysicians at Scripps Health in San Diego for hip & knee replacements and severalinpatient spine surgeries. (This is a SISC value added service; call Carrum directly, notAnthem.) Value Based Pricing for Arthroscopy, Cataract Surgery, Colonoscopy, Upper GI WITHand WITHOUT Biopsy. Bariatric/Hip/Knee/Spine surgeries only covered when performed at a Blue Distinction Center for Specialty Care.HMO PlanReminders:
Skilled Nursing Facility and Inpatient Rehabilitation will now have a combined 150 daylimit per benefit period.REMINDERS: Most generic prescriptions are 0 copay at Costco pharmacies.KaiserCHANGES: Starting October 1, 2022. Retiree members enrolled in Kaiser Senior Advantage planwill have access to Medical transportation for Retirees who can’t drive. This new benefitcan provide them with up to 24 annual one-way rides to go to or from lab visits, doctorappointments and pharmacies to pick up medications or medical equipment. Meal delivery – Retirees after an inpatient stay at a hospital or skilled nursing facility,can get healthy more quickly with fresh and nutritious meal deliveries. Calm Meditation and Mindfulness App – All SISC Kaiser members have free access tothe highly acclaimed Calm meditation and mindfulness smart phone application.REMINDERS: Kaiser dual (TVUSD) spouses receive 25% medical only premium discount.Dental PlansREMINDERS: Two Delta dental plans are offered: 1) Delta PPO (NO ORTHO); and, 2) Delta PPO Incentive(includes ortho). The Delta PPO Incentive plan is an incentive-based plan with increasingbenefit by year (year 1 70%; year 2 80%; year 3 90%; year 4 100%). Increasing benefitrequires bi-annual dental exams.Please be reminded to use the Delta Dental web site to ensure your dental service providers arecontracted as Delta PPO providers before you obtain services.CHANGES: Toothpic is an innovative, photo-based teledentistry app that offers a virtual dental screeningfrom a Delta Dental dentist, right from your smartphone.Vision Plan – NO CHANGESREMINDERS: Please be reminded to use the VSP web site to ensure that your vision service providers arecontracted as VSP Signature providers before you obtain services.SISC offers many additional programs for physical and mental health. You can findinformation on the items mentioned on this sheet and much more on the TVUSD websiteunder Risk Management/Health Insurance.PLEASE SEE FLYERS WHICH INCLUDE INFORMATION ABOUT SISC’S VALUEADDED PLANS.
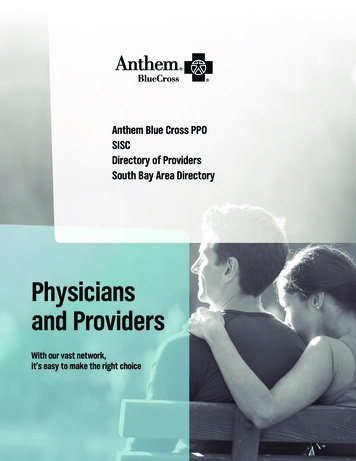
Temecula Valley USDMedical Plan Comparisons1CERTIFICATEDEffective 10/1/2022Whereever you see a percentage,this is what is covered after thedeductible has been met.BC PPO - 40464E (individual)&40464F (Family) HSA CompatibleBC PPO - 40464AProvider Network(s):Hospital & ProfessionalBC PPO - 40464BBC PPO - 40464CALL PLAN CHANGES AND/OR NEW PLANSARE IN RED INK(including notes at the bottom)KAISER 4231876-00117HMO Classic 57AHCA(refer to plan summary for65 retiree plan)2-TIER ANCHOR BRONZE(Medical Only)NO SPOUSES ORREGISTERED DOMESTICPARTNERS7BC PPO - 70466BPrudent BuyerPrudent BuyerPrudent BuyerAnthem Blue CrossAnthem Blue CrossKaiser PermanentePrudent Buyer 300 per individual up to 600 perfamily 3,000 per individual up to 6,000 perfamily 500 per individual up to 1,000 perfamilyIndividual: 1,500* Family: 2,800( 3000)as of 1/1/23 and 3000 FamilyNoneNone 5,000 per individual upto 10,000 per family3 1,000 per individual up to 3,000 perfamily 4,000 per individual up to 8,000 perfamily 2,000 per individual up to 4,000 perfamily 2,000 per individual up to 4,000 perfamily 1,500 per individual up to 3,000 per family 6,350 per individual up to 12,700 per cipatingProvidersParticipatingProvidersDeductible, then 90% 20 copay 30 copay 30 copay; deductible waived 0 copay for first 3 visits to pcp eachcalendar year 40 copay; deductible waived 0 copay for first 3 visits to pcpeach calendar year 30 copay; deductible waived 0 copay for first 3 visits to pcp eachcalendar year90% 20 copay 0 copay90% 40 copay 30 copayInpatient Hospital (prior authorizationrequired)100%80%80%90% 250 copay/admit 0 copay70%Outpatient Hospital100%80%80%90% 125 copay/admit 30 copay70%55580%90% 125 copay/admit 30 copay70%590% 125 copay/admit 30 copay70%5Calendar Year Deductible(s) ²Out-of-Pocket Maximum (Deductible CoInsurance Co-pays) - EXCLUDESPRESCRIPTIONSServicesOffice Visits & Urgent CarePrenatal/postnatal office visit co-paySpecialistsSurgery, Outpatient (performed in SurgeryCenter)5100%80% 3,000 Ind / 6000 Family(Includes medical deductibles,co-insurance and co-pays)ParticipatingProviders70%100%580%580%5 100 Co-pay* Deductible, then paid at100% 100 Co-pay* Deductible, then paidat 80% 100 Co-pay* Deductible, then paid at80%90%, 100 co-pay 100 copay 100 copay 100 copay* Deductible,then paid at 70%100%; deductible waived100%; deductible waived100%; deductible waived100% Ded Waived 0 copayNo charge up to 23 monthsDeductible Waived; 100%100%; deductible waived100%; deductible waived100%; deductible waived0% , Ded Waived 0 copay 0 copayDeductible Waived; 100%Scans: CT, CAT, MRI, PET etc.100%80%80%90% 100 co-pay/test 0 copay70%Diagnostic X-ray & Laboratory Procedures100%80%80%90% 0 copay 0 copay70%Physical & Occupational Therapy - LimitsApply100%80%80%90% 40 copay 30 copay70%Chiropractic (limits apply)100%80%80%90% 10/30 visits combined w/ AcupunctureAcupuncture (limits apply)100%80%80%90% 10/30 visits combined w/ ChiropracticDurable Medical Equipment (DME)100%80%80%90%20% co-insuranceno charge70% 100 Co-pay Deductible, then paid at100% 100 Co-pay Deductible, then paidat 80% 100 Co-pay Deductible, then paid at80%90%, 100 co-pay 100 copay 50 copay 100 Co-pay Deductible,then paid at 70%100%80%80%90%Refer to Benefit SummaryRefer to Benefit Summary70%Deductible co-insurance amounts thatexceed reference price (Arthroscopy 4500; Cataract Surgery 2000;Colonoscopy 1500; Upper GIEndoscopy W/ Biopsy 1250, W/outbiopsy 1000Deductible 20% co-ins amounts thatexceed reference price (Arthroscopy 4500; Cataract Surgery 2000;Colonoscopy 1500; Upper GIEndoscopy W/ Biopsy 1250, W/outbiopsy 1000Deductible 20% co-ins amounts thatexceed reference price (Arthroscopy 4500; Cataract Surgery 2000;Colonoscopy 1500; Upper GIEndoscopy W/ Biopsy 1250, W/outbiopsy 1000N/AN/AN/ADeductible 30% co ins amountsthat exceed reference price(Arthroscopy 4500; CataractSurgery 2000; Colonoscopy 1500; Upper GI Endoscopy W/Biopsy 1250, W/out biopsy 1000Not CoveredNot CoveredNot CoveredNot Covered50% co-insuranceOffice Visit copay orhospitalization copay applyNot coveredSurgery, Outpatient (performed in a Hospital)5Emergency Room (*co-pay waived ifadmitted)Well Baby/Child Preventative CareBirth to age sixPreventative Care (includes physical exams &screenings, age and medical necessity rulesapply))Ambulance (Ground or Air)Hip/Knee/Spine surgery (Subject to utilizationreview; covered only at Blue Distinction Centers for Specialty Care)5Value Based Purchasing Benefit (Effective10/1/2018, PPO plans)Innetwork Ambulatory Surgery Center NO benefitchange; In-network Hospital Outpatientfacility pay deductible co-insurance amountsthat exceed reference price (listed to the right)Infertility (diagnosis/treatment of causes ofinfertility subject to plan benefits) 10/30 visits combined w/Acupuncture 10/30 visits combined w/Chiropractic70%70%
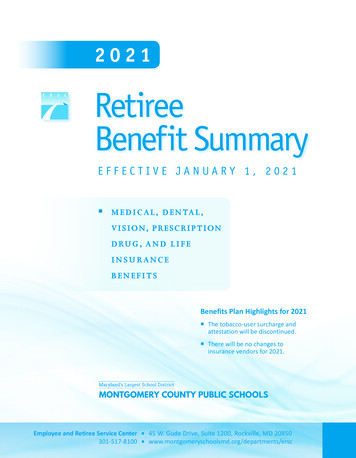
Temecula Valley USDMedical Plan Comparisons1CERTIFICATEDEffective 10/1/2022KAISER 231876-00114HMO Classic 57AHCA(refer to plan summary for65 retiree plan)ParticipatingProvidersParticipatingProviders 500 allowance per device,1 device per ear, 2 devicesper 36 months2-TIER ANCHOR BRONZE70466B (Medical Only)7BC PPO - 40464ABC PPO - 40464BBC PPO - 40464CHSA-A Individual / ParticipatingProviders 700 Benefit Allowance per 24 moperiod 700 Benefit Allowance per 24 moperiod 700 Benefit Allowance per 24 moperiodParticipatingProviders 700 Benefit Allowance per 24 moperiod, 90% and Amount in excessallowance100%80%80%90% 250 copay/admit 0 copay70%100%80%80%90% 0 copay 30 visit70%Individual/Family Brand & Specialty RxDeductibles 200 individual/ 500 family 200 individual/ 500 family 200 individual/ 500 familyIncluded w/Medical Deductible 200 individual/ 500 familyNoneRx Included with MedicalDeductibleIndividual/Family Rx Out-of-Pocket (OOP)Max (Includes Rx deductibles and co-pays) 2500/ 3500 2500/ 3500 2500/ 3500Included w/ Medical OOP Max 2500/ 3500Included w/ Medical OOPMaxIncluded w/ Medical OOPMax 0 at Costco; 10 at Other Network 0 at Costco; 10 at Other Network 0 at Costco; 10 at Other Network 0 at Costco; 10 at Other Network 10 up to 100 day supply 9 after Med Ded is met 35 35 35 35 30 up to 100 day supply 35 after Med Ded is met 35 Must Use Navitus Mail 35 Must Use Navitus Mail 35 Must Use Navitus Mail 35 Must Use Navitus Mail 30 up to 30 day supplyMail 35 after Med Ded is met 0- 90 0- 90 0- 90 0- 90 10- 10/up to 100 daysupply 0- 90 after Med Ded is metServicesHearing Aid BenefitMental Health & Substance AbuseTreatmentInpatient: Facility Based Care (priorauthorization required)Outpatient: Facility Based Care (priorauthorization required):Generic Rx co-pay/30 days supplyBrand Rx co-pay/30 days supplySpecialty co-pay/up to 30 days supplyMail Order (Generic-Brand co-pay/90 dayssupplyDeductible, then 0 at Costco or 9 atOther NetworkDeductible, then 35Deductible, then 35 Must Use NavitusMail50% Benefit allowance/1 device/36 moDeductible, then 0- 90ParticipatingProviders 700 Benefit Allowance per 24mo period6Deductible includes prescription. 4thquarter carryover NO longer applies.Now HSA compliant plan.Premiums shown are for 100% contracts. Please refer to the "monthly costs" sheets for less than 100%.EmployeeOnlyEmployee Child(ren) 1,010.00MedicalDental PPO 100% 1500 (no ortho)/Vision 1,656.00 1,111.00 1,409.00 1,265.00 1,436.00 1,512.00 643.00 108.50 108.50 108.50 108.50 108.50 108.50N/AN/AContribution- 937.25- 937.25- 937.25- 937.25- 937.25- 937.25- 937.25- 937.25PAYROLL DEDUCTION: 827.25 282.25 580.25 436.25 607.25 683.25 0.00 72.75 413.25 20.25 228.00 120.00 248.25 305.25N/AN/AMedicalDental PPO INCENTIVE 1700/ 1500WITH Ortho 3000 Plan / Vision 1,656.00 1,111.00 1,409.00 1,265.00 1,436.00 1,512.00 643.00 1,010.00 140.10 140.10 140.10 140.10 140.10 140.10N/AN/AContribution- 937.25- 937.25- 937.25- 937.25- 937.25- 937.25- 937.25- 937.25PAYROLL DEDUCTION: 858.85 313.85 611.85 467.85 638.85 714.85 0.00 72.75 444.85 36.10 259.60 151.60 279.85 336.85N/AN/ADUAL TVUSD SPOUSES DEDUCTION :DUAL TVUSD SPOUSES DEDUCTION :FOOTNOTES:1This is a brief summary of benefits that is superseded by the Plan Documents and is not all inclusive. This summary is for comparison purposes only. Please refer to the actual benefit booklet for complete benefits.2It is the member's responsibility to verify provider participation in the appropriate PPO network prior to accessing services. Utilizing a non-contracted provider will result in greater out-of-pocket expense for the member. Website links are available from the TVUSD web page. Wherever you see a percentage on the plancomparison, this is what is paud AFTER the deductible is met.3Includes prescription.4No out-of-network benefits; all services must be rendered through Kaiser.5Reminder: Effective 10/1/2018 subject to "Value Based Pricing" for Arthroscopy, Cataract Surgery, Colonoscopy, Upper GI WITH and WITHOUT Biopsy6 Reminder: Medical deductible includes prescriptions. This plan does NOT have a 4th quarter carryover effective 1/1/2018.7HSA compliant plans are subject to legislation and regulation changes throughout the year. Please refer to IRS HSA contribution guidelines – Section 223 and IRS Publication 969 for more specific guidelines for contribution eligibility. When (2) TVUSD Spouses or (2) TVUSD Registered Domestic Partners (RDP) both are enrolled there is a 25% premium discount on both participants' medical policies. Spouses and RDPs must advise at time of enrollment when both employees are enrolled. If member had ortho under a different employers' plans that life time usage would be transferred to the new employer. Thus, the employee would only have coverage if the new lifetime limit was higher than the prior plan. The member would also only have access to the difference between the plans.* Please be reminded that it is your responsibility to check your pay stubs monthly for accuracy. If you change plans during open enrollment it is your responsibility to check your new cards for accuracy.* For Covered Expenses Only: All percentages are based on payments to preferred hospitals, physicians and other network providers. When using Non-PPO & Other Health Care Providers, members are responsible for any difference between the covered expense and actual charges, as well as any deductible & percentage copay.
October 1, 2022 Payroll Healthcare DeductionsCertificated EmployeesDistrict Monthly Contribution 937.25Monthly Deduction by Plan with Vision and Delta Dental PPO 100%BC PPO – 40464ABC PPO – 40464BBC PPO – 40464CBC HAS – AHMO 57AHCAKaiser 827.25 282.25 580.25 436.25 607.25 683.252-Tier Anchor Bronze(Employee Only) 02-Tier Anchor Bronze(Employee children) 72.752-Tier Anchor Bronze(Employee Only)02-Tier Anchor Bronze(Employee children) 72.752-Tier Anchor Bronze(Employee Only)N/A2-Tier Anchor Bronze(Employee children)N/A2-Tier Anchor Bronze(Employee Only)N/A2-Tier Anchor Bronze(Employee children)N/AMonthly Deduction by Plan with Vision and Delta Premier Incentive with OrthoBC PPO – 40464ABC PPO – 40464BBC PPO – 40464CBC HAS – AHMO 57AHCAKaiser 858.85 313.85 611.85 467.85 638.85 714.85Dual Spouse DiscountMonthly Deduction by Plan with Vision and Delta Dental PPO 100%BC PPO – 40464ABC PPO – 40464BBC PPO – 40464CBC HAS – AHMO 57AHCAKaiser 413.25 20.25 228.00 120.00 248.25 305.25Dual Spouse DiscountMonthly Deduction by Plan with Vision and Delta Premier Incentive with OrthoBC PPO – 40464ABC PPO – 40464BBC PPO – 40464CBC HAS – AHMO 57AHCAKaiser 444.85 36.10 259.60 151.60 279.85 336.85
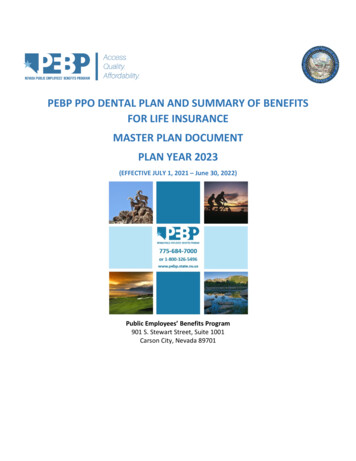
SISC Medical Plan Costs effective October 1st, 2022Premium Costs for Certificated Employees withVision and Dental PPO 100% PlanPART-TIME EMPLOYEEPORTION OF DISTRICTCONTRIBUTION% y-Up 468.63 421.77 374.90 328.04 281.18 234.32 187.45 140.59 93.73 46.87 0.00Anthem BlueCross PPO 40464ATotalMonthlyPremium 1,295.88 1,249.02 1,202.15 1,155.29 1,108.43 1,061.57 1,014.70 967.84 920.98 874.12 827.25Anthem BlueCross PPO 40464BTotalMonthlyPremium 750.88 704.02 657.15 610.29 563.43 516.57 469.70 422.84 375.98 329.12 282.25Anthem BlueCross PPO 40464CTotalMonthlyPremium 1,048.88 1,002.02 955.15 908.29 861.43 814.57 767.70 720.84 673.98 627.12 580.25Anthem BlueCross PPOHSA-ATotalMonthlyPremium 904.88 858.02 811.15 764.29 717.43 670.57 623.70 576.84 529.98 483.12 436.25Anthem BlueCross HMO 57AHCAKaiser 231876-00112-Tier Anchor Bronze70466B **Employee TotalEmployee Only Child(ren) MonthlyTotal Monthly Total MonthlyTotal MonthlyPremiumPremiumPremiumPremium 1,075.88 1,151.88 174.38 541.38 1,029.02 1,105.02 127.52 494.52 982.15 1,058.15 80.65 447.65 935.29 1,011.29 33.79 400.79 888.43 964.43 0.00 353.93 841.57 917.57 0.00 307.07 794.70 870.70 0.00 260.20 747.84 823.84 0.00 213.34 654.12 776.98 0.00 166.48 654.12 730.12 0.00 119.62 607.25 683.25 0.00 72.752-Tier Anchor Bronze Plan - Employee or Employee Child(ren) ONLY; no spouses/registered domestic partners; and no dental and vision.How the chart works: The "buy up" column represents how much more premium is your responsibility to pay if you work less than100% contract. The District contributes 937.25 per month to a 100% contract employee's premium. If you are a 50% contractemployee, you would have to "buy up" 468.63 per month because you only get 50% of the District contribution. FOR EXAMPLE: Ifyou take the 100% contract premium for PPO plan 40464A ( 827.25) and you add the 50% contract "buy up" ( 468.63), yourpremium would be 1295.88 per month.The "buy up" is included in the "total monthly premium" columns.
SISC Medical Plan Costs effective October 1st, 2022Premium Costs for Certificated Employees withVision and Premier Dental with OrthodonticsPART-TIME EMPLOYEEPORTION OF DISTRICTCONTRIBUTION% y-Up 468.63 421.77 374.90 328.04 281.18 234.32 187.45 140.59 93.73 46.87 0.00Anthem BlueCross PPO 40464ATotalMonthlyPremium 1,327.48 1,280.62 1,233.75 1,186.89 1,140.03 1,093.17 1,046.30 999.44 952.58 905.72 858.85Anthem BlueCross PPO 40464BTotalMonthlyPremium 782.48 735.62 688.75 641.89 595.03 548.17 501.30 454.44 407.58 360.72 313.85Anthem BlueCross PPO 40464CTotalMonthlyPremium 1,080.48 1,033.62 986.75 939.89 893.03 846.17 799.30 752.44 705.58 658.72 611.85Anthem BlueCross PPOHSA-ATotalMonthlyPremium 936.48 889.62 842.75 795.89 749.03 702.17 655.30 608.44 561.58 514.72 467.85Anthem BlueCross HMO 57AHCAKaiser 231876-00112-Tier Anchor Bronze70466B **Employee TotalEmployee Only Child(ren) MonthlyTotal Monthly Total MonthlyTotal MonthlyPremiumPremiumPremiumPremium 1,107.48 1,183.48 174.38 541.38 1,060.62 1,136.62 127.52 494.52 1,013.75 1,089.75 80.65 447.65 966.89 1,042.89 33.79 400.79 920.03 996.03 0.00 353.93 873.17 949.17 0.00 307.07 826.30 902.30 0.00 260.20 779.44 855.44 0.00 213.34 732.58 808.58 0.00 166.48 685.72 761.72 0.00 119.62 638.85 714.85 0.00 72.752-Tier Anchor Bronze Plan - Employee or Employee Child(ren) ONLY; no spouses/registered domestic partners; and no dental and vision.How the chart works: The "buy up" column represents how much more premium is your responsibility to pay if you work less than100% contract. The District contributes 937.25 per month to a 100% contract employee's premium. If you are a 50% contractemployee, you would have to "buy up" 468.63 per month because you only get 50% of the District contribution. FOR EXAMPLE: Ifyou take the 100% contract premium for PPO plan 40464A ( 858.85) and you add the 50% contract "buy up" ( 468.63), yourpremium would be 1327.48 per month.The "buy up" is included in the "total monthly premium" columns.
SISC PLAN CHANGES AND REMINDERS Effective 10/1/2022 The No Surprises Act On December 11th, 2020, the No surprises Act was passed into law. This new legislation . BEFORE services are rendered. Carrum Health provides PPO members with access to an enhanced benefit with selected physicians at Scripps Health in San Diego for hip & knee .