Transcription
Curr Cardiovasc Imaging Rep (2010) 3:162–170DOI 10.1007/s12410-010-9021-0New Imaging Protocols for New Single Photon EmissionCT TechnologiesPiotr J. Slomka & Daniel S. Berman & Guido GermanoPublished online: 20 April 2010# The Author(s) 2010. This article is published with open access at Springerlink.comAbstract Nuclear cardiology practitioners have severalnew technologies available with which to perform myocardialperfusion single photon emission CT (MPS). These includededicated small-footprint cardiac scanners, new stationary orsemi-stationary three-dimensional detectors, and advancedsoftware algorithms for optimal image reconstruction. Thesenew technologies have been employed to reduce imaging timeand radiation exposure. They require less technologist andcamera time and offer improved patient comfort. They havepotential for the overall cost reduction of MPS and at the sametime for improved accuracy by increased resolution, oraccurate attenuation correction. Furthermore, these newtechnologies offer potential for new protocols such assimultaneous dual isotope, new combinations of isotopes,stress only MPS, or dynamic first-pass imaging. In addition,new imaging technologies in coronary CT angiography(CCTA) allow novel hybrid stress only MPS/CCTA protocolswith reduced radiation burden. Additional developmentsfurther improving efficiency and diagnostic accuracy of MPSare on the horizon.Keywords Myocardial perfusion SPECT . Solid statedetectors . Stress-only protocol . Hybrid imaging . Cardiacfusion . Simultaneous dual isotope . Fast cardiac SPECT .Dynamic imagingIntroductionMyocardial perfusion single photon emission CT (MPS) isa widely used clinical test, with approximately 9 millionP. J. Slomka (*) : D. S. Berman : G. Germano8700 Beverly Boulevard, Suite A047,Los Angeles, CA 90048, USAe-mail: SlomkaP@cshs.orgstudies being performed annually in the United States [1].Until recently, typical scans were long procedures, requiring15 to 20 min for each stress and rest MPS acquisition, to allowadequate imaging statistics. Additional consequences of longimaging times were frequent motion artifacts caused bypatient motion during the scan and compromised patientcomfort. Recent advances in new detector designs allowdramatic reduction of imaging times to less than 2 min in somecases, or alternatively, dramatic reductions in the radiationdose to the patient. Cameras now available from manyvendors have increased photon sensitivity achieved by meansof custom detector geometry and innovative designs ofcollimation (including multiple pinhole or slit hole collimators), focusing of the field of view on the heart and using solidstate detectors. The optimized geometry for cardiac imagingallows significantly reducing or totally eliminating the motionof the detector, with simultaneous collections of counts fromthe whole heart. The new cameras have often reducedfootprint and allow easier patient positioning, and in manycases upright imaging. Faster imaging and more comfortablepatient position results in reduced patient motion duringacquisition. Additionally, three-dimensional (3D) character ofthe acquisition reduces the effect of patient motion on imagequality.These new camera designs are coupled with novelmethods of image reconstruction. Improvements in reconstruction algorithms allow accurate resolution recovery andcorrections of physical effects via iterative reconstructionalgorithms. These new methods of image reconstructioncan be implemented on standard cameras. Combination ofthe new hardware and the new reconstruction modelsallows simultaneous improvements in photon sensitivityand image resolution. Furthermore, list mode acquisitioncapabilities are now available, allowing arbitrary timereformatting of the data after the scan. Consequently, firstpass 3D dynamic imaging and kinetic modeling with
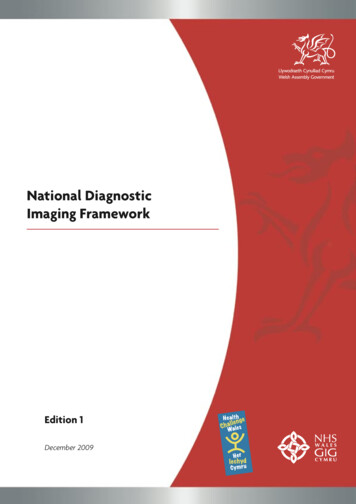
Curr Cardiovasc Imaging Rep (2010) 3:162–170stationary or semi-stationary single photon emission CT(SPECT) detectors is now possible, similar to what hasbeen available in positron emission tomography (PET).Additionally, increased photon sensitivity can be utilized topursue novel imaging protocols such as simultaneous dualisotope, or new combinations of isotopes allowing rapidstress/rest assessment. Recently we reviewed new hardwareand software developments from a technical perspective[2 ]. In this review article, we summarize current clinicalapplications and trials with emphasis on novel imagingprotocols that are possible with the new generation ofdevices, including hybrid imaging protocols.New Cardiac SPECT TechnologiesSeveral vendors have developed hardware and softwaretechnologies allowing reduced imaging or dose time,improved patient comfort, and improved image quality.Digirad Inc. (Poway, CA) has developed a cardiac CardiusXPO camera, which is coupled with new reconstructiontechnology (n-speed). For imaging, the patient sits on achair with his or her arms placed on an armrest above thedetectors [3]. Digirad has also incorporated a low-costapproach to obtain x-ray transmission scans for attenuationcorrection that can be implemented with the XPO camera.Another dedicated cardiac camera was developed byCardiArc (Canton, MI), optimized specifically for cardiacimaging and upright patient position [4]. Spectrum Dynamics(Haifa, Israel) has manufactured a solid-state dedicatedcardiac system called D-SPECT with semi-stationary detectors,high-sensitivity collimation, and reconstruction optimizedspecifically for cardiac imaging. The patient is imaged in asemi-upright position with the left arm placed on top of thecamera or in the supine position. General Electric Healthcarehas developed a stationary imaging camera based on the multipinhole design, an alternative technique for photon collimation[5–7], and an array of cadmium zinc telluride pixilateddetectors [8]. Patients are imaged in a supine position withtheir arms placed over their heads. Two examples of studiesobtained with D-SPECT and GE Discovery NM 530c withcomparable acquisition times and doses are shown in Fig. 1.Siemens has combined an astigmatic collimator, an optimizedorgan-of-interest centered acquisition, and iterative reconstruction in their IQ SPECT system with CT-based attenuationcorrection (on Symbia platform) and energy window-basedscatter correction [9]. This system allows hybrid MPS-CTimaging.In parallel, efforts have been undertaken to improveimage contrast and reduce noise levels by reconstructionalgorithms that incorporate physical modeling of thedetectors based on ordered subsets expectation maximization(OSEM) [10] and applied to data acquired on standard163scanners. Philips (San Jose, CA) has developed a fast SPECTreconstruction algorithm (Astonish) that includes correctionsfor photon scatter, photon attenuation, and variations in spatialresolution and allows reduced imaging time. UltraSpect Inc.(Haifa, Israel) has developed a standalone workstation thatutilizes the patented Wide Beam Reconstruction (WBR)algorithm [11, 12].Fast Imaging and Dose Reduction in Clinical StudiesIn the past 2 years, these new hardware systems andreconstruction techniques have been utilized clinically toreduce patient imaging time and radiation dose. Typically,these studies have been validated by comparing to studiesperformed with the same injected dose during the samepatient visit on a conventional dual head SPECT camera.Data were analyzed by blinded visual or by quantitativeanalysis. Several of these studies combined data frommultiple centers. Herzog et al. [13] performed phantom andclinical studies to establish the most optimal imaging timefor the solid-state multi-pinhole Discovery NM 530cdetectors and found that scan as short as 2 min with327 MBq mean dose and 3-minute rest scan with 915 MBqprovide equivalent images to 15-minute acquisitions withthe standard camera. A similar protocol was followed in 75patients by the same group, and excellent correlation forper-vessel and per-patient perfusion defects was found withconventional SPECT [14]. In the United States, theDiscovery NM 530c system was evaluated by the EmoryUniversity group [15 ]. Similarly high correlations withconventional SPECT were found for perfusion defects andfor left ventricular ejection fractions (LVEFs).The D-SPECT camera was compared with a standarddual detector in 44 patients and reported shorter imagingtimes and higher MPS quality for the new camera, withhigh correlations in visual perfusion scores [16]. In anotherstudy, a novel stress Tl-201/rest Technetium-99m protocol,with total stress/rest imaging time reduced to less than20 min, including additional supine views, was describedand compared to a standard Tc/Tc protocol on the same fastcamera (Fig. 2) [17 ]. They concluded that Tl/Tc protocoloffers similar image quality and dosimetry (11.9 mSv vs11.2 mSv; P not significant), but results in much shortertotal imaging time and offers potential for better depictionof stress lesions with physiologically superior Tl-201 agent(Fig. 3). Furthermore, this study demonstrated possibility ofdual-position imaging for these new cameras with patientimaged in upright and supine positions. Two-positionimaging allows improved diagnostic accuracy by resolvingof subtle attenuation artifacts or patient motion as demonstrated in prone-supine conventional SPECT imaging [18].In another large study of D-SPECT data from four US
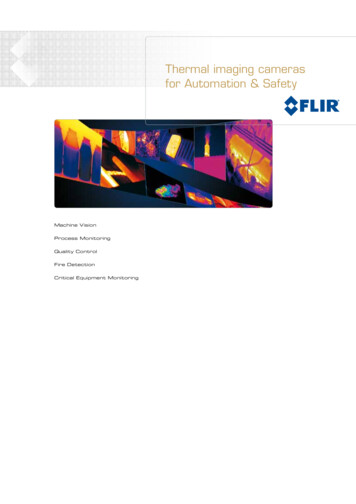
164Curr Cardiovasc Imaging Rep (2010) 3:162–170Fig. 1 Examples of two patientstudies obtained with DiscoveryNM 530c (system 1; imagescourtesy of Dr. Ernest Garcia)and D-SPECT (system 2;images courtesy of Dr. JackZiffer), showing good-qualitystudies with comparableacquisition protocols(2-minute stress, 4-minute rest)centers, Sharir et al. [19 ] used fully automated quantitative software with normal limits developed for the newcamera for their data analysis. They demonstrated that thequantitative total perfusion deficit [20] obtained with the fastprotocol correlated linearly with stress and rest conventionalSPECT (r 0.95 and r 0.97, respectively; P 0.0001), andthat the average amount of ischemia was higher in the highlikelihood patients, as compared to conventional SPECT.Similarly, LVEFs and LV volumes obtained with fullyquantitative analysis [21] were highly correlated.Fast imaging protocol for the Digirad cardiac system(majority with dual or triple head configuration) withoptimized image reconstruction has been evaluated in amulticenter trial (11 centers) by Maddahi et al. [22]. Theyfound that images from fast protocols were diagnosticallyFig. 2 Fast Tl-201stress/Tc-99m rest protocolfor adenosine (top) and exercise(bottom) myocardial perfusionSPECT protocol. At peak stress,patients were injected withTl-201. After a 5-minutepost-stress monitoring period,supine and semi-upright (sitting)acquisitions were performedsequentially. Subsequently,Tc-99m sestamibi (mibi) ortetrofosmin (tetro) was injected,and a single 4-minute sittingrest acquisition was performed.(Modified from Berman etal. [17 ])equivalent in 444/448 (99%) of the patients as determinedby blinded visual analysis. Functional parameters ejectionfraction, diastolic, and systolic volume were also highlycorrelated. With a conventional camera, fast imaging bymeans of optimized WBR reconstruction with imageresolution recovery and novel approach to noise controlwas also evaluated [12]. This reconstruction was applied todata obtained on a conventional dual-head system (GE,Ventri) with high-resolution parallel-hole camera. DePueyet al. [23] reported equivalent summed stress and restperfusion scores with similar image quality at rest andsuperior at stress for the in ¼ time WBR imaging ascompared to full-time standard OSEM reconstruction.Similar to the other studies, functional parameters were alsohighly correlated.
Curr Cardiovasc Imaging Rep (2010) 3:162–170165Fig. 3 Images of a 53-year-old man with no known coronary arterydisease and hypertension, diabetes, hypercholesterolemia, and shortnessof breath, acquired with fast 201T1 exercise stress/99mTc rest protocolshowing large severe reversible defects in the anterior and lateral walls.Coronary angiography revealed 70% stenosis in the mid left anteriordescending artery and the second diagonal branch. Percutaneous coronaryintervention and stent implantation were subsequently performed in thesetwo vesselsIn other clinical reports, some preliminary results havebeen presented for the SPECT IQ system, with imagingtimes as short as 4 min. The Symbia T series systems alsoallow for obtaining of CT calcium scan in as little as 30 sduring the same imaging session [24]. Preliminary study offast 3-minute gated imaging with multi-pinhole system onconventional detectors has been also been presented byKoss et al. [25], which facilitates the study of segmental LVperfusion and contractile performance during infuseddobutamine stress and during the recovery period followingstress.interpretive certainty, with equivalent summed perfusionscores obtained by blinded visual analysis. Importantly, inthis study 92 of 118 cases had available correlating angiography and the diagnostic performance for the stress-only halftime AC MPS imaging was equivalent to standard full-timeFBP studies. Therefore, the authors concluded that the stressonly AC MPS approach with optimized reconstruction has thepotential to significantly improve MPS efficiency withoutreducing test accuracy. Additionally, stress-only scan reducesthe patient radiation dose to less than 8 mSv, which could befurther reduced by using standard rather than half-timeacquisition times.Recent peer-reviewed clinical studies referenced above,which utilize the new technology in order to reduceimaging time, are summarized in Table 1.Stress-Only MPSThe effective imaging time and patient dose reductioncould also be accomplished by means of eliminating theresting MPS scan. Stress-only MPS protocols withattenuation correction (AC) have been advocated in thepast [26]. The stress-only approach increases laboratoryefficiency, decreases cost, and improves patient convenience, while reducing radiation dose [27]. The PhilipsAstonish approach to reducing scan time allows simultaneous AC and MPS acquisition, reducing potential for anymisregistration artifacts associated with CT AC. It hasbeen demonstrated that half-time acquisitions, whencompared to standard (filtered back-projection) FBPprocessing, have equivalent diagnostic accuracy with bothAstonish [28] and GE Evolution systems [29]. Bateman etal. [30 ] conducted a study to determine the clinicalfeasibility of stress-only protocol with reduced scan timeand simultaneous acquisition of AC scan. They found thatsimulated half-time scans (obtained by reconstructionsampling from full-time scans) when compared to standardFBP reconstruction without AC had similar quality andNovel MPS ProtocolsBeyond simply reducing the acquisition time or patientradiation dose, there are several reports of novel MPSprotocols, which take advantage of superior imaging characteristics of new devices or availability of new modalities forhybrid imaging. These include techniques for simultaneousdual isotope imaging, dynamic imaging, and hybrid coronaryCT angiography (CCTA)/MPS imaging.Simultaneous Dual IsotopeRoutine simultaneous dual isotope would reduce theimaging time in half compared to the separate stress andrest study. The superior energy resolution of the newdetectors can allow better separation of photons fromdifferent isotopes, which can result in much improvedcross-talk correction [32]. In addition, stationary detector
166Curr Cardiovasc Imaging Rep (2010) 3:162–170Table 1 Recent clinical studies demonstrating possibility of shortened imaging times with MPSStudySystemNHerzog et al. [13]Discovery NM 530c20Buechel et al. [14]Discovery NM 530c75Maddahi et al. [22]Digirad 2/3-headEsteves et al. [15 ]Discovery NM 530c189239168Sharir et al. [16]D-SPECT44Berman et al. [17 ]D-SPECTSharir et al. [19 ]D-SPECT374262238Gambhir et al. [31]D-SPECT18DePuey et al. [23]UltraSPECT Widebeam 209ReconstructionBateman et al. [30 ] Stress only Astonish110Protocol1-day 99mTc-tetrofosminadenosine stress-rest1-day 99mTc-tetrofosminadenosine stress-rest3-head Rest/stress 99mTc2-head1-day 99mTc-tetrofosminrest/stress1-day 99mTc stress/restsestamibiStress Tl/rest 99mTcRest/stress Tc/TcRest/stress tetrofosmin/sestamibi 99mTc1-day 99mTc-sestamibistress/restRest/stress 99mTc-sestamibiStress only99mInjected doseAcquisition timeStress/rest 8.8/25.1 mCi3 min/2 minoptimal3 min/2 minStress/rest 9.1/25.6 mCiRest/Stress 7–10 mCi/20–30 mCi 4.8 min/4.3 min6.5 min/4.3 minRest/stress 10–15/30–45 mCi4 min/2 minStress/rest 11/28 mCi4 min/2 minStress/rest Tl/Tc 2–2.5/8–10 mCi; 6 min/4 minTc/Tc 8–10/25–40 mCi4 min/2 minRest/stress 10/30 mCi4 min/2 minStress/rest 11/28 mCi4 min/2 minRest/stress 9/32 mCi4.5 min/4 minTc-sestamibi Stress 25–35 mCi6 min/–MPS myocardial perfusion SPECT, SPECT single photon emission CTsystem design eliminates the projection consistencies thatwould further confound the simultaneous dual isotopeimaging. The improved statistical content of new scannersis also a key factor in supporting the ability to imagemultiple isotopes simultaneously. A natural application is tosimultaneously image 99mTc and 201Tl in a combined rest/stress protocol as originally proposed for standard cameras[33], but never implemented clinically due to technicaldifficulties.A proof-of-concept of simultaneous dual-isotope imagingon a multi-pinhole system was recently demonstrated bySteele et al. [34], who used 222 MBq of 99mTc injected at restand 148 MBq of 201Tl injected 1 min before the end ofexercise and performed simultaneous dual-isotope imagingof 201Tl (stress) and 99mTc (rest) immediately after completion of exercise, by the three-detector 18-pinhole system,during a single 20-minute imaging session. Ben-Haim et al.[35] reported the feasibility of simultaneous dual-isotopeapplication with the solid-state D-SPECT camera. Theystudied 24 patients with simultaneous dual-isotope imagingwith 80 MBq of 201Tl injected at rest and 250 MBq of 99mTcsestamibi injected during adenosine infusion. Images werecollected in a 15-minute list mode simultaneous dualradionuclide (rest/stress) gated acquisition with a spilloverand scatter correction method, specifically designed forsolid-state camera. Comparable diagnostic performance andimage quality to conventional SPECT with a separate rest201Tl acquisition on D-SPECT has been demonstrated. Theproposed imaging protocol for this application is shown inFig. 4.Dynamic ImagingThe potential for absolute measurement of flow and flowreserve has remained the key advantage of PET over SPECT[36]. The new SPECT camera designs, however, withstationary detectors such as the multi-pinhole systems [8,37], or systems with semi-stationary detectors such as DSPECT design, where the whole 3D view is captured withlimited detector motion in a few seconds, may allow first-passMPS imaging. The proof-of-concept of such studies for theDiscovery NM 530c platform has been demonstrated byHuang et al. [38] with the NCAT digital phantom simulationsand one-compartment modeling, for 99mTc-teboroxime. Theyconcluded that this stationary MPS system can provide aparametric image of myocardial blood flow for this myocardial perfusion agent. A group at Brigham and Women’sHospital in Boston, MA, in collaboration with our center, iscurrently exploring the quantification of regional and globalestimates of coronary flow reserve on the D-SPECT systemwith 99mTc sestamibi [39]. MPS imaging is performed with10 and 30 mCi of 99mTc sestamibi injected at rest and duringvasodilator stress, respectively, with imaging starting immediately with the intravenous bolus injection of radiotracer.Using list mode capabilities of D-SPECT device, the4-minute stress and rest image data are reconstructed into70 3.5-second frames. Estimates of the myocardial perfusionreserve can be derived with one-compartment model implemented within the Cedars-Sinai kinetic modeling QPETsoftware in a fully automated mode [40]. Estimates ofmyocardial reserve can be obtained on a per-vessel or per-
Curr Cardiovasc Imaging Rep (2010) 3:162–170167Fig. 4 Illustration of thesimultaneous dual isotope (SDI)protocol for the solid statecameraA novel concept in modifying the imaging protocols is toemploy hybrid technology [41] that may include novelsoftware tools for image fusion. Specifically, recentadvances in CCTA allow routine dose reduction inprospective mode to the 2 mSv range [42]. CCTA has beenshown to have a very high negative predictive value indetection of coronary artery disease. These new developments allow a combined CCTA-MPS imaging protocolwith acceptable radiation burden. Exploiting this concept,Fig. 5 Dynamic quantitative analysis of abnormal study obtained onD-SPECT system showing segmental analysis of myocardial perfusionindex with segmental values (top left), dynamic images, myocardialperfusion SPECT images (top left), input curves (bottom left), andoutput stress and rest curves (bottom right). (Data courtesy of MarceloDi Carli, Brigham & Women’s Hospital)segment basis. Example of dynamic MPS images obtainedwith this novel imaging protocol is shown in Fig. 5.Hybrid Imaging
168Husmann et al. [43 ] demonstrated the feasibility of stressonly MPS/CCTA protocol. In the study, 1-day adenosinestress/rest MPS using a dose of 300 and 900 MBq of 99mTctetrofosmin, respectively, for stress and rest, with low-doseCT attenuation correction, was combined with CCTAobtained on a separate GE VCT 64-slice scanner in 100patients. The total patient time scheduled on the hybridCCTA/stress-MPS examination protocol was 130 min,which is shorter than total times during current 1-daystress/rest MPS protocols. It should be noted that thisprotocol could be significantly shortened if rest scans werenot performed. All CCTA examinations in this study wereperformed in the 90 min between the first injection of99mTc-tetrofosmin and stress data acquisition. They haveshown that by using stress-only and prospectively gatedCCTA data the combined dose would be 5.4 0.8 mSv, andsuch hybrid combination offers additional diagnosticinformation as compared to stress/rest study, without increased radiation exposure [43 ]. Furthermore, hybrid cardiacimaging offered a high confidence in image interpretation, asequivocal findings in either of the scans can be resolved bythe complementary modality. The principal drawback of thisapproach is that clinicians usually do not know ahead of timewhich patients will require both CCTA and MPS studies,such that sequential application of the methods, only whenneeded, may prove to be the more cost effective approach.Future DirectionsTo summarize, many novel protocols have been describedrecently taking advantage of new detector design and newalgorithms for software reconstruction. Primarily, the newclinical studies have aimed to reduce the total imaging time andscanning efficiency. However, in view of recent increasedawareness of potential radiation exposure risks, it is possiblethat these protocols will be modified to reduce the radiationdose instead. It is conceivable that this can be customizedbased on the patient age, for example [44], since the radiationrisk models assume that risk is inversely proportional topatient age. Similarly, to date, stress-only protocols have beendemonstrated with conventional patient dosing. It is feasiblethat an aggressive dose-reducing protocol could involve fulltime stress-only scan with reduced dose. Similarly, the hybridCCTA/stress MPS protocol could be performed with the useof the new efficient detectors, allowing a further dosereduction. The CCTA technology is also advancing rapidly,and recently excellent image quality was reported for newhigh-pitch spiral CCTA at a consistent dose below 1.0 mSv[45]. In addition, it should be possible to selectively eliminatethe stress MPS scan, for example if CCTA was normal [41],reducing the effective radiation burden and procedure cost.Additional improvements in hybrid imaging diagnosticCurr Cardiovasc Imaging Rep (2010) 3:162–170accuracy could be accomplished by accurate image fusionaiding visual [46] or quantitative [47] analysis.As the new efficient MPS hardware and software designsare being evaluated clinically, there are preclinical effortsongoing that demonstrate that even higher sensitivity andefficiency can be achieved in cardiac SPECT. For example,Zeng and Stevens [48] theoretically demonstrated that multidivergent-beam collimators could be used for stationarycardiac SPECT and that this design has the potential to besuperior to currently available multi-pinhole systems interms of sensitivity by a factor of 2, maintaining the sameimage resolution. In another report, theoretical calculationsfor multi-pinhole designs with curved detectors fitted topinholes demonstrated potential of close to 50% improvement [49] as compared to the latest multi-pinhole designsclinically available.ConclusionsNuclear cardiology equipment and associated software haveundergone very significant advances in the recent years. Thesenew developments have been employed to test new imagingprotocols with improved patient comfort, reduced imagingtime, and reduced radiation dose. Novel protocols such assimultaneous dual-isotope, stress-only acquisitions, dynamicimaging, and hybrid multimodality protocols are beingexplored to further reduce imaging time and also improve thediagnostic information. Additional improvements in efficiency of cardiac SPECT technologies are possible, allowingfurther reductions in imaging time and radiation dose.Disclosure Dr. Berman has equity position in Spectrum DynamicsInc., and all of the authors participate in software royalties fromCedars-Sinai Medical Center.Open Access This article is distributed under the terms of theCreative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in anymedium, provided the original author(s) and source are credited.ReferencesPapers of particular interest, published recently,have been highlighted as: Of importance Of major importance1. Dilsizian V, Narula J: Atlas of Nuclear Cardiology, edn 3.Springer; Philadelphia, PA: 2009.2. Slomka PJ, Patton JA, Berman DS, Germano G: Advances intechnical aspects of myocardial perfusion SPECT imaging. J NuclCardiol 2009, 16:255–276. This is a comprehensive review of thetechnical aspects of the new systems and software.
Curr Cardiovasc Imaging Rep (2010) 3:162–1703. Lewin HC, Hyun MC: A clinical comparison of an upright triplehead digital detector system to a standard supine dual-headgamma camera [abstract]. J Nucl Cardiol 2005, 12:113.4. www.CardiArc.com. Accessed May 30, 2008.5. Jaszczak RJ, Li J, Wang H, et al.: Pinhole collimation for ultrahigh-resolution, small-field-of-view SPECT. Phys Med Biol 1994,39:425–437.6. Schramm NU, Ebel G, Engeland U, et al.: High-resolution SPECTusing multipinhole collimation. IEEE Transactions on NuclearScience 2003, 50:315–320.7. Beekman FJ, Vastenhouw B: Design and simulation of a highresolution stationary SPECT system for small animals. Phys MedBiol 2004, 49:4579–4592.8. Volokh L, Hugg J, Blevis I, et al.: Effect of detector energyresponse on image quality of myocardial perfusion SPECT. Paperpresented at IEEE Nuclear Science Symposium and MedicalImaging Conference. Dresden, Germany; October 19–26, 2008.9. Vija H, Chapman J, Ray M: IQ SPECT technology White Paper.Siemens Medical Solutions USA Molecular Imaging; 2008:1–7.10. Hudson HM, Larkin RS: Accelerated image reconstruction usingordered subsets of projection data. IEEE Transactions on MedicalImaging 1994, 13:601–609.11. Ultraspect. www.UltraSPECT.com. Accessed September 6, 2008.12. Borges-Neto S, Pagnanelli RA, Shaw LK, et al.: Clinical results ofa novel wide beam reconstruction method for shortening scan timeof Tc-99m cardiac SPECT perfusion studies. J Nucl Cardiol 2007,14:555–565.13. Herzog BA, Buechel RR, Katz R, et al.: Nuclear myocardial perfusionimaging with a cadmium-zinc-telluride detector technique: optimizedprotocol for scan time reduction. J Nucl Med 2010, 51:46–51.14. Buechel RR, Herzog BA, Husmann L, et al.: Ultrafast nuclearmyocardial perfusion imaging on a new gamma camera withsemiconductor detector technique: first clinical validation. Eur JNucl Med Mol Imaging 2009, In press.15. Esteves FP, Raggi P, Folks RD, et al.: Novel solid-state-detectordedicated cardiac camera for fast myocardial perfusion imaging:multicenter comparison with standard dual detector cameras. JNucl Cardiol 2009, 16:927–934. This is the first clinical US studyof the new multi-pinhole detector system.16. Sharir T, Ben-Haim S, Merzon K, et al.: High-speed myocardialperfusion imaging: initial clinical comparison with conventionaldual detector anger camera imaging. JACC Cardiovasc Imaging2008, 1:156–163.17. Berman DS, Kang X, Tamarappoo B, et al.: Stress thallium-201/resttechnetium-99m sequential dual isotope high-speed myocardialperfusion imaging. JACC Cardiovasc Imaging 2009, 2:273–282.This is a novel Tl/Tc protocol for dose-efficient fast stress and restMPS scanning.18. Nishina H, Slomka PJ, Abidov A, et al.: Combined supine andprone quantitative myocardial perfusion SPECT: method development and clinical validation in patients with no known coronaryartery disease. J Nucl Med 2006, 47:51–58.19. Sharir T, Slomka P, Hayes S, et al.: Multicenter trial of high-speedvs. conventional SPECT imaging: quantitative results of myocardialperfusion and left ventricular function. J Am Coll Cardiol 2010, Inpress. This article includes a comparison of fully automatedperfusion quantification for conventional and fast SPECT.20. Slomka PJ, Nishina H, Berman DS, et al.: Automated quantificationof myocardial perfusion SPECT using simplified normal limits. JNucl Cardiol 2005, 12:66–77.21. Germano G, Kiat H, Kavanagh PB, et al.: Automatic quantificationof ejection fraction from ga
Fig. 2 Fast Tl-201 stress/Tc-99m rest protocol for adenosine (top) and exercise (bottom) myocardial perfusion SPECT protocol. At peak stress, patients were injected with Tl-201. After a 5-minute post-stress monitoring period, supine and semi-upright (sitting) acquisitions were performed sequentially. Subsequently, Tc-99m sestamibi (mibi) or