Transcription
Course IC22-105 (ID 1238941)Collagen crosslinkingEvolving indications, technology, applications, resultsand complication managementEric D. Donnenfeld, MDGregory J. Pamel, MDDoyle Stulting, MDA. John Kanellopoulos, MDDirector, Laservision.gr Institute, Athens, GreeceClinical Professor NYU Medical School, NYKanellopoulos MD1
1-How many of you currentlyperform CXL?a-YESb-No2
2-Do you understand how CXLworks?a-YESB-no3
3-How long do you think CXLlasts?a:1 yearb:2-3 yearsc:3-5 yearsD: 10 years4
4-What is the worst complicationof CXL?a-Infectious keratitisb-cornea scarringc-cornea meltd-dry eyee recurrence of ectasia5
5-If CXL is offered early enough,can it eradicate clinicalkeratoconus?a-yesb-noc-I do not know6
6-Should CXL’ed women bemonitored closer duringpregnancy for ectasiarecurrence?a-yesb-noc-don't know7
7-Should a 45 year old malerecently diagnosed with KCN beoffered CXL?a-Yesb-noc-I do not know8
8-is this KCN?a-yesb-noc-do not know9
Financial interests Alcon/WavelightBausch & LombRevision OpticsSeros MedicalAvedroOcular Therapeutix
Livestream all our surgeries:http://www.livestream.com/laservision orlivestream.com/laservision A. John Kanellopoulos, MD Director, Laservision.gr Institute, Athens, Greece Clinical Professor NYU Medical School, NYKanellopoulos MD11
12
CXL: a Photooxidative reactioncourtesy E. Spoel, MD photodynamical reaction Typ 2 RF UV 1RF* 3RF* 3O 1O (Singulet-oxygen) 22 production of radicals oxidative disemination
Biochemical reactioncourtesy E. Spoel, MD
Introduction of riboflavin in afemto-pocket15
Decrease of UV-intensitycourtesy E. Spoel MD3.00 mW/cm²1.49 mW/cm²0.74 mW/cm²0.36 mW/cm²0.18 mW/cm²0.09 mW/cm²
Visual rehabilitation of ECTASIA Spectacles, Contacts, INTACS,DALK, PK! CXL Combined technique: CXL tgPRK Implantation of phakic IOLs in cases with high residual myopiaand/or anisometropia CXL prior to a phakic IOL will produce a more stable ground forcalculating the refractive error other
We introduced: Higher fluence CXL:6, 7, 9, 10 and 12mW/cm2AAO 2008:CXL for 15minutesutilizing7mW/cm2fluence18
Introduced Prophylactic CXL inPRK and LASIK
Kanellopoulos,MD20
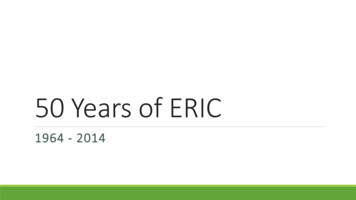
Oxygen Depletion Over 30 MinutesOxygen Concentration, mg / L1010,10,010,010,11Time, min10100Depletion and gradual replenishment of dissolved oxygen below a 100 µmthick corneal flap, saturated with 0.1% RF during 3 mW/cm2 UVA irradiationat 25 0C.21
10 minute postop-Cornea OCT -8 months follow-upNo regression of the flattening effect!Kanellopoulos,MD22
Zurich 2007: CXL for PBK: 2 femtopockets and CXL with 10mW/cm2
Post-LASIK ectasia: -1 -1.75@ 75. Pach 445, Treated withepi-on CXL ( C3R) 3mW/cm2 for 30’.Same case seen 3 years later with ectasia progressionKanellopoulos,MD24
4 years after iLASIK CXL
Variable UVfluence: Avedro1-30mW/cm2
Topo-guided partial PRK1-Topolyzer:Placido disc topography2-Pentacam (Oculyzer)3-Pentacam HD (oculyzer II)-Refractive suite4-Vario (placido disc pupil sensor iris recognition limballandmarks recognition)WaveLight FS200Femtosecond LaserWaveLight EX500Excimer LaserWaveLight Refractive Suite
The Athens Protocol:PTK topoPRK MMC CXL (7mW/cm2 x 15 min)340mOsm 0.1% riboflavinsodium phosphate7mW/cm2 for 15 minutes
29
The AthensProtocol7-years
JRS Sept 2009Kolozsvári et alIOVS 2002;43:2165-2168
In oblique KCN: AveK from 44.6 to just 44.3!Flattest K steeper by 1Drefraction 0.50-3.50@160(20/60) to -1.5D (20/20)Kanellopoulos MD32
2 year follow up in a 15 y/oKanellopoulos MD33
Athens Protocol: safety34
Athens Protocol:Some improvement in UCVA, dramatic improvementin BSCVA: 98% of cases at least 20/40!)35
Combined same-day tgPRK andCXL appear to be superior to therehabilitation of KCN and ectasia One procedureLess PRK-associated scarringBetter riboflavin penetrationLess shielding of UV by Bowman’s wider CXL areaRedistribution of cornea’s strain (biomechanics)No need to remove cross-linked corneaUnderscore refraction
Average K from 48.5 to 44Refraction -2.5-4.5@155 (20/70) to -1-1.5@10 (20/20)Kanellopoulos MD37
26y/o pilot, from UCVA 20/60 to20/15
Little change in keratometryBSCVA 20/50 to 20/20Kanellopoulos MD39
postLASIK ectasia:Difference: pre- and post- treatment
Bilateral LASIK ectasiatreated with topoPRK CXL:ODOS
Short and long term complications of combinedtopography guided PRK and CXL (the AthensProtocol) in 412 keratoconus eyes (2-7 yearsfollow-up)Anastasios John Kanellopoulos, MDDirector, Laservision.gr Institute, Athens, GreeceClinical Professor NYU Medical School, NYFinancial Interests: Alcon. Wavelight
From UDVA 20/20 to 20/40 over 4 yearswith a 2.5D hyperopic shift
Unknown Possible Long Term CXLRisksCataractsConjunctival squamous cell carcinomaLong Term Dry Eyes due to UV A Damageto ocular surfaceProgressive thinningPoor glaucoma management
OCT evaluation
2 months after AP
Late stromal scar
Late stromal scar-resolving
AP15mos
3 months later (lotemax, Autologous)
2 weeks out-delayed epitheliazation
2 weeks later (1 month postop)
Early haze (2 months-gone after 6 months)
Delayed epithelial healing
Delayed epithelial healing with hazeOD simple AP, OS after K scar from CL
2 weeks-delayed healing with heaped-up white margins
2 months-PRK scar
2 months-PRK anterior stromal scar
2 weeks-elevated epi scar
Severe scar of the corneaBCVA 20/200,Lamellar or PK?Kanellopoulos,MD62
Kanellopoulos,MD63
From 20/200 to 20/40!Kanellopoulos,MD64
Conclusions-ectasia management CXL is an effective means of ectasia stabilization We are using: Higher fluence, shorter/pulsed expotime Athens Protocol: topo-guided partial PRK CXLstable with long term follow-up is our standardchoice in ALL cases Prophylactic CXL may become a customisedbiomechanic modulator in LASIK
HFUEpithelial and mapping on normal and keratoconic (non-treated and treated) eyes. Kanellopoulos et 6
Epithelial thickness: nl-KCN-KCNcxl’edEpithelial and mapping on normal and keratoconic (non-treated and treated) eyes. Kanellopoulos et ! !not!treated!KCN! ,&and&at&the&pupil¢er.&67
Epithelial thickness maps May become the earliest prognostic factorfor ectasia We have found that in KCN there is overallINCREASE in average epithelial thickness Following CXL the same eyes showdramatic reduction of epithelial thicknessto slightly below of normal68
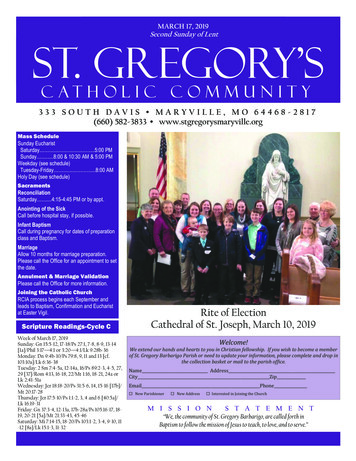
Oxygen Depletion Over 30 MinutesType IIType I TypeI & IIDepletion and gradual replenishment of dissolved oxygen below a 100 µmthick corneal flap, saturated with 0.1% RF during 3 mW/cm2 UVAirradiation at 25 0C.69
ASCRS 2012Crosslinking and Long-Term Hyperopic LASIK StabilityInitial Clinical Findings in ContralateralEye StudyJonathan B. Kahn, M.D.1 and A. John Kanellopoulos, M.D.1,21NewYork University School of Medicine, New York, NY, USA2Laservision.grInstitute, Athens, GreeceAJK is a consultant for Alcon, Wavelight and Avedro.
LASIK flap creation using FS200 femtosecond laser (Alcon, Ft. Worth, TX)9.5mm LASIK flap nasally decentered, adjusted for angle kappaCrosslinking and Long-Term Hyperopic Lasik Stability71Presentation Title Goes Here
Topo-guided LASIK excimer treatment plan centered onvisual axisCrosslinking and Long-Term Hyperopic Lasik Stability72Presentation Title Goes Here
Lifting the femto-created flapCrosslinking and Long-Term Hyperopic Lasik Stability73Presentation Title Goes Here
A drop of 0.1% riboflavinsodium phosphate solution(Leiter’s pharmacy, San Jose, CA)Crosslinking and Long-Term Hyperopic Lasik Stability74Presentation Title Goes Here
Flap repositioned followingstromal soak with riboflavinCrosslinking and Long-Term Hyperopic Lasik Stability75
Corneal OCT (Optovue, CA,USA) in LASIK Xtra groupCrosslinking and Long-Term Hyperopic Lasik Stability76
LASIK CXLGroup1 yearGoesCrosslinking and Long-TermPresentationHyperopic LasikTitleStability77Here
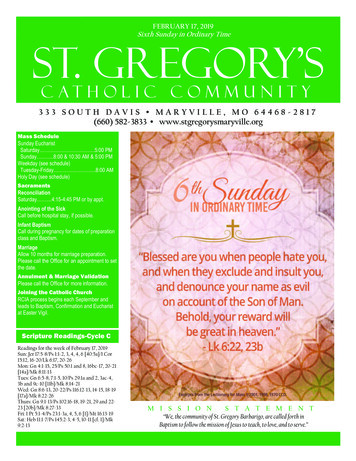
Comparison ofKeratometricStabilityMean Keratometry (D)4746Lasik Xtra45Std Lasik444342Pre op1m3m6m12m24mGoesCrosslinking and Long-TermPresentationHyperopic LasikTitleStability78Here
8mm, 150um femto pocket79
Infusion of the vertiporfin80
Vertiporfin-soaked cornea81
Photodynamic cornea treatment andCXL with monochromatic red light!82
pdt-CXL83
Control-just visudyne84
CXL with veriporfin as thephotosensitizer:1-no uv-light!2-FDA approved for use in human eye3-smaller molecule, better bioavailabilityin cornea4-working on dose-dependence curves85
Conclusions higher fluence CXL Our current protocols1-Athens Protocol: topoPRK 10’x 10mw/cm22-LASIK Xtra: 1’ (60”) 45mW/cm22-PRK Xtra: 1’ (60”) 30mW/cm23-Transepithelial CXL: 0.25% riboflavin 30mW/cm2 X 3’ (180”) 3-Infection: 0.25% riboflavin 45mW/cm2 x 5minutesKanellopoulos MD86
Conclusions higher fluence CXL CXL can sterilize the stroma higher fluence andhigher riboflavin % may be useful The apoptosis of keratocytes may have unknownbenefit to epithelial hyperplasia and risks Potential endothelial toxicity Potential limbal cell cell and/or goblet cell toxicityfrom collateral Rib interaction CXL may prove to be the standard collagenstabilizer and adjunct disinfectant in LASIK, PRKand even cataract surgeryKanellopoulos MD87
Conclusions higher fluence CXL Appears to be more effectve if Type I model of CXLholds true Customised fluence and riboflavin concentrationmay personalize CXL as a biomechanical stromalmodulator for many applications: May prevent regression in hyperopia LASIK Xtra appears to have only potentialadvantages May become the standard of care for PRK (reducescarring, epithelial hyperplasia)Kanellopoulos MD88
Thank youKanellopoulos MD
Gregory J. Pamel, MD Doyle Stulting, MD . 1-How many of you currently perform CXL? a-YES b-No 2 . 2-Do you understand how CXL works? a-YES B-no 3 . 3-How long do you think CXL lasts? a:1 year b:2-3 years c:3-5 years D: 10 years 4 . 4-What is the worst complication of CXL? a-Infectious keratitis