Transcription
CLINICAL ARTICLEJ Neurosurg Spine 31:508–518, 2019Two-level cervical disc arthroplasty versus anteriorcervical discectomy and fusion: 10-year outcomes of aprospective, randomized investigational device exemptionclinical trialMatthew F. Gornet, MD,1 Todd H. Lanman, MD,2 J. Kenneth Burkus, MD,3 Randall F. Dryer, MD,4Jeffrey R. McConnell, MD,5 Scott D. Hodges, DO,6 and Francine W. Schranck, BSN7The Orthopedic Center of St. Louis, St. Louis, Missouri; 2Institute for Spinal Disorders, Cedars-Sinai Medical Center, LosAngeles, California; 3Wilderness Spine Services, Columbus, Georgia; 4Central Texas Spine Institute, Austin, Texas; 5OrthopedicSpecialists, Allentown, Pennsylvania; 6Center for Sports Medicine & Orthopaedics, Chattanooga, Tennessee; and 7SPIRITTResearch, St. Louis, Missouri1OBJECTIVE The authors assessed the 10-year clinical safety and effectiveness of cervical disc arthroplasty (CDA)to treat degenerative cervical spine disease at 2 adjacent levels compared to anterior cervical discectomy and fusion(ACDF).METHODS A prospective, randomized, controlled, multicenter FDA-approved clinical trial was conducted comparingthe low-profile titanium ceramic composite–based Prestige LP Cervical Disc (n 209) at two levels with ACDF (n 188).Ten-year follow-up data from a postapproval study were available on 148 CDA and 118 ACDF patients and are reportedhere. Clinical and radiographic evaluations were completed preoperatively, intraoperatively, and at regular postoperativefollow-up intervals for up to 10 years. The primary endpoint was overall success, a composite variable that included keysafety and efficacy considerations. Ten-year follow-up rates were 86.0% for CDA and 84.9% for ACDF.RESULTS From 2 to 10 years, CDA demonstrated statistical superiority over ACDF for overall success, with rates at10 years of 80.4% versus 62.2%, respectively (posterior probability of superiority [PPS] 99.9%). Neck Disability Index(NDI) success was also superior, with rates at 10 years of 88.4% versus 76.5% (PPS 99.5%), as was neurological success (92.6% vs 86.1%; PPS 95.6%). Improvements from preoperative results in NDI and neck pain scores were consistently statistically superior for CDA compared to ACDF. All other study effectiveness measures were at least noninferiorfor CDA compared to ACDF through the 10-year follow-up period, including disc height. Mean angular ranges of motionat treated levels were maintained in the CDA group for up to 10 years. The rates of grade IV heterotopic ossification (HO)at the superior and inferior levels were 8.2% and 10.3%, respectively. The rate of severe HO (grade III or IV) did notincrease significantly from 7 years (42.4%) to 10 years (39.0%). The CDA group had fewer serious (grade 3–4) implantrelated or implant/surgical procedure–related adverse events (3.8% vs 8.1%; posterior mean 95% Bayesian credibleinterval [BCI] of the log hazard ratio [LHR] -0.92 [-1.88, -0.01]). The CDA group also had statistically fewer secondarysurgical procedures at the index levels (4.7%) than the ACDF group (17.6%) (LHR [95% BCI] -1.39 [-2.15, -0.61]) as wellas at adjacent levels (9.0% vs 17.9%).CONCLUSIONS The Prestige LP Cervical Disc, implanted at two adjacent levels, maintains improved clinical outcomesand segmental motion 10 years after surgery and is a safe and effective alternative to fusion.Clinical trial registration no.: NCT00637156 3171/2019.4.SPINE19157KEYWORDS cervical degenerative disc disease; cervical disc arthroplasty; Prestige LP disc replacement; artificialcervical disc; radiculopathy; myelopathy; two-level disc disease; anterior cervical discectomy and fusion; ACDFABBREVIATIONS ACDF anterior cervical discectomy and fusion; AE adverse event; BCI Bayesian credible interval; CDA cervical disc arthroplasty; cTDR cervical TDR; DDD degenerative disc disease; FSU functional spinal unit; HO heterotopic ossification; HPD highest posterior density; IDE investigational deviceexemption; LHR log hazard ratio; MCS Mental Component Summary of SF-36; NDI Neck Disability Index; PAS postapproval study; PCS Physical ComponentSummary of SF-36; PPS posterior probability of superiority; ROM range of motion; TDR total disc replacement.SUBMITTED February 9, 2019. ACCEPTED April 9, 2019.INCLUDE WHEN CITING Published online June 21, 2019; DOI: 10.3171/2019.4.SPINE19157.508J Neurosurg Spine Volume 31 October 2019 AANS 2019, except where prohibited by US copyright lawUnauthenticated Downloaded 08/24/22 10:04 PM UTC
Although anterior cervical discectomy and fusion(ACDF) is the standard surgical treatment for cervical degenerative disc disease (DDD) associatedwith radiculopathy and myelopathy, clinical studies havedemonstrated the safety and efficacy of total cervical discreplacements, variously referred to as total disc replacement (TDR), cervical total disc replacement (cTDR), cervical disc replacement (CDR), cervical disc arthroplasty(CDA), and artificial disc replacement (ADR), for bothone- and two-level disease.2–5,7,10–12,15,20,21,24,25,27 These studies used ACDF as the control group/standard treatmentagainst which to assess noninferiority and potential superiority of CDA.ACDF affects segmental motion at adjacent vertebrae, altering spinal biomechanics and creating abnormalloads,6,32 which may place additional stress on adjacentdiscs that could accelerate their degeneration.9,26,32 Manypatients have multilevel disease, and two-level ACDF mayresult in even greater stresses to adjacent discs.17 Multilevel ACDF also has higher rates of pseudarthrosis, revisions, complications, and reoperations than single-levelACDF.28,30 CDA was designed as a motion-preserving alternative to ACDF for treating DDD at one or more levels.The Prestige LP Cervical Disc (Medtronic, Inc.) wasapproved by the FDA in 2014 for treating single-levelDDD and intractable radiculopathy or myelopathy.10 Aclinical trial began in 2006 to evaluate the safety and efficacy of Prestige LP at two adjacent levels compared toACDF. The primary outcome measure was overall success 24 months following surgery. Overall success rateswere 81.4% and 69.4% for the CDA and ACDF groups,respectively.11 Both noninferiority and superiority in overall success were established for CDA compared to ACDF,and the FDA granted marketing approval for the use of thePrestige LP Cervical Disc in the treatment of two-level degenerative disc disease with intractable radiculopathy and/or myelopathy in 2016. A postapproval study (PAS) withpatient follow-up to 10 years was required by the FDA, and7-year follow-up results have been reported.15 Those resultscontinued to show the noninferiority of CDA compared toACDF as well as superiority in overall success and othermeasures.This report assesses long-term effectiveness and safetyof the Prestige LP Cervical Disc at two contiguous levels,comparing outcomes at 10 years postoperatively to thosefor ACDF. To our knowledge, this is the first randomizedstudy with 10-year follow-up data for a two-level use of aspinal device.MethodsSurgeries for this clinical trial occurred betweenJune 2006 and November 2007 (clinicaltrials.gov,NCT00637156). The study protocol and informed consentform received IRB approval (Western Investigational Review Board, protocol no. 20060636, study no. 1078218).The prospective, randomized, multicenter, controlledstudy was designed to assess the safety and efficacy oftwo-level cervical disc arthroplasty with the Prestige LPCervical Disc compared with the control treatment (a twolevel anterior cervical fusion procedure involving corticalGornet et al.ring allograft and the ATLANTIS Cervical Plate System,Medtronic, Inc.) in patients with intractable radiculopathyand/or myelopathy at two adjacent levels of the cervicalspine. Informed consent was obtained from all patients.The specific methods and procedures for this clinical trialhave been described in detail elsewhere, including inclusion and exclusion criteria and detailed definitions of alloutcome measures.11,15 Key components of the researchprotocol are summarized below.PatientsPatients were randomized to receive either PrestigeLP CDA or the fusion control treatment. In total, 397 patients (209 CDA and 188 ACDF) were treated with theassigned treatment. Characteristics of the CDA patientsincluded mean (SD) age of 47.1 (8.3) years, 56.0% female,and 93.3% Caucasian. The treatment groups were similardemographically, with no statistical differences (p 0.05)except preoperative work status (not considered a clinically important difference).11 The groups did not differ inrelevant preoperative medical conditions or medication usage, including time from symptom onset to surgery, previous neck surgery, or pain medication usage. Radiculopathywas the presenting complaint in 71.8% and 72.9% of theCDA and ACDF groups, respectively, with another 25.8%and 23.9%, respectively, presenting with both radiculopathy and myelopathy. Finally, there were no significant preoperative differences between groups in any of the clinicalmeasures. Treatment levels were C5–6 or C6–7 in 78% ofCDA and 75% of ACDF patients.At 10 years postoperatively, 148 patients in the CDAgroup and 118 in the ACDF group had evaluations (Table1), yielding follow-up rates of 86.0% for CDA and 84.9%for ACDF after excluding patients at sites not participating in the PAS study, deaths, and withdrawals. Nearly allwithdrawals were initiated by patients after surgery, mostcommonly because they found the study requirements toodemanding (e.g., too much time, too many visits), theywere feeling better and did not feel they needed to see thedoctor, or they were moving from the area. For patients lostto follow-up over time, the most frequent reasons were lackof contact information after moving out of the area or unwillingness to undergo further evaluations; some patientsdied. Patient demographics and preoperative medical status and medication usage were compared between groupsfor just patients included in this 10-year follow-up study.No significant differences were found. The mean patientage preoperatively was 47.1 years for CDA patients and47.6 years for ACDF patients.MaterialsInvestigational DeviceThe Prestige LP Cervical Disc is a dynamic device madeof a titanium alloy/titanium carbide composite (also referred to as titanium ceramic composite). It contains smallamounts of vanadium and aluminum and does not containnickel or chrome. It is implanted through an anterior approach following a discectomy and is available in varioussizes to accommodate the intervertebral disc space and toengage adjacent vertebral bodies. Device components areJ Neurosurg Spine Volume 31 October 2019509Unauthenticated Downloaded 08/24/22 10:04 PM UTC
Gornet et al.TABLE 1. Patient accountability for long-term follow-up5 Yrs7 Yrs10 YrsPatient StatusCDAACDFCDAACDFCDAACDFEnrolledAt sites not participating at 10 yrsTheoretical follow-upCumulative withdrawalsCumulative deathsPatients to be expectedEvaluated expected patientsFollow-up 018828*160183139*118*84.9Values are presented as number of patients unless otherwise indicated.* One ACDF patient who was at one of the nonparticipating sites, and thus was not included in the numbers of expected or evaluated patients,had a serious implant-related AE at 6 weeks postoperatively and by definition the results for this patient were considered a failure for overallsuccess at all subsequent time points. Therefore, there were 119 patients in total who had overall success results at 10 years.placed into the vertebral bodies through impaction at surgery and maintained via bony ingrowth over time.Outcome MeasuresThe primary endpoint was “overall success,” a composite of safety and efficacy endpoints. Overall success wasachieved if the postoperative score improvement in theNeck Disability Index (NDI)31 was 15 points, neurological status did not worsen, and no serious implant-associated or implant/surgical procedure–associated adverse event(AE), or second surgery, which was deemed “failure,”occurred. Definitions of “success” for individual efficacymeasures have been previously described.15Other outcome measures included neck and arm painnumerical rating scales adapted from a previously definedscale,18 yielding a total pain score based on both intensityand frequency; the Medical Outcomes Study SF-3633 Physical Component Summary (PCS) and Mental ComponentSummary (MCS); radiographic assessments of 3 types(disc height assessed using functional spinal units [FSUs],heterotopic ossification [HO] assessed only in the CDAgroup and graded from 0 to IV according to the methodreported by Mehren et al.,19 and implant condition); patient satisfaction (3 questions answered numerically witha 5-point scale from “definitely true” to “definitely false”);patient global perceived effect (7-point scale from “completely recovered” to “vastly worsened”); foraminal compression test; physician’s perception of results (“excellent,”“good,” “fair,” or “poor”); AE including severity (grades1–4) and possible association with implant and/or surgicalprocedure assessed by an independent Clinical Adjudication Committee; neurological status; and secondary surgical procedures classified as revision, removal, supplemental fixation, reoperation, or other. A secondary surgicalprocedure at the index level(s) caused the patient’s surgicaloutcome to be classified as a study failure with respect tooverall success if it required supplemental fixation, implant removal, or revision.ProceduresPatient evaluations occurred preoperatively (within 6510months of surgery), at surgery, and postoperatively at approximately 6 weeks, 3 months, 6 months, and 1, 2, 3, 5, 7,and 10 years. The clinical trial endpoint for the investigational device exemption (IDE) study was 24 months, butPAS follow-ups have continued, and the 10-year findingsare the subject of this report.Radiographic MeasurementsImages obtained at study sites were sent to a centralcore laboratory (Biomedical Systems, St. Louis, MO) forindependent review by two primary reviewers using aproprietary imaging archival system and software-basedmeasurement tools for quantitative measurements (e.g., intervertebral angle, horizontal translation, FSU height, etc.).A third reviewer was used for adjudications.Statistical MethodsThe primary objective of the IDE study was to demonstrate that the overall success rate in the CDA group wasstatistically noninferior to the overall success rate in theACDF group at 24 months following surgery, with a prespecified noninferiority margin of 0.10 (i.e., a minimumclinically important difference in success rate of 10%). Ifnoninferiority in overall success was established for CDAcompared to ACDF, the CDA treatment was considered tobe safe and effective, and then superiority was evaluated.Success rates for individual effectiveness endpoints werecompared between the two treatment groups; when noninferiority of CDA was established, superiority was evaluated. This same analysis strategy was used for the PASevaluations, including the 10-year results presented here.Bayesian statistical methods were used for comparingdifferences in success rates between groups. The criterionfor noninferiority and for superiority of CDA compared toACDF was a posterior probability of at least 95%. Becausenoninferiority for overall success and individual endpointswas, in fact, established, only posterior probability of superiority (PPS) results are presented here. Improvementsfrom preoperative results in continuous measures such asNDI scores, SF-36 scores, and neck and arm pain scoresJ Neurosurg Spine Volume 31 October 2019Unauthenticated Downloaded 08/24/22 10:04 PM UTC
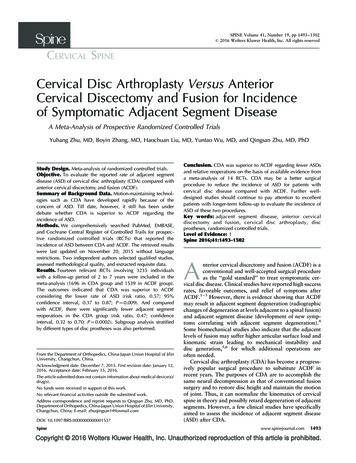
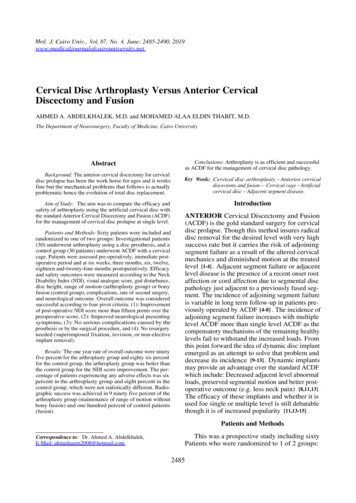
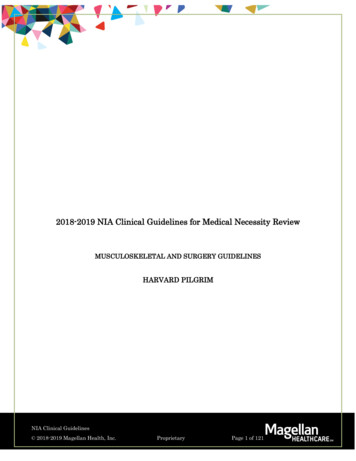
Gornet et al.were also compared between treatment groups by usingBayesian methods.For all adverse events and secondary surgical procedures, including secondary surgeries involved with adjacent level(s), usual hypotheses were used to assess statistical differences between treatment groups. Log hazard ratios (LHRs) of rates of occurrence between groups and the95% Bayesian credible interval (BCI) of highest posteriordensity (HPD) were computed to determine whether ratesdiffered statistically between groups. Noninformative priors were used for all Bayesian analyses.For patients who had additional (“secondary”) surgicalprocedures/interventions (supplemental fixation, implantremoval, or revision), their results were deemed failuresfor overall success. Because these additional surgical procedures/interventions had potential to alter the originalstudy treatment outcomes, for all neurological status andindividual effectiveness variables the last observation obtained before additional surgery was carried forward forsubsequent observation periods.An independent statistical analysis using the sameprotocol approved by the FDA was performed for the24-month and 60-month data by the Vanderbilt UniversityMedical Center Biostatistics Collaboration Center. Results for both intervals were consistent with the sponsorMedtronic’s analyses and thus independent analyses werenot performed for other intervals and were not requiredby FDA.ResultsEfficacy Success RatesFigure 1 shows success rates and posterior probabilities of superiority for overall success, NDI success, andneurological success over time. Superiority was established for CDA compared to ACDF for overall successand NDI success at all postoperative intervals. Observedoverall success rates for CDA and ACDF at 10 years were80.4% and 62.2%, respectively (PPS 99.9%), yielding adifference in Bayesian success probabilities (95% BCI)between CDA and ACDF of 18.0% (7.3%, 28.7%). At 10years, 88.4% of CDA patients met criteria for NDI successcompared to 76.5% of ACDF patients (PPS 99.5%), witha difference in Bayesian success probabilities (95% BCI)of 11.9% (2.7%, 21.3%). Neurological success rates tendedto be higher for CDA over time and were statistically superior at 7 and 10 years compared to ACDF. At 10 years, theneurological success rate was 92.6% for CDA compared to86.1% for ACDF (PPS 95.6%).Individual Effectiveness VariablesObserved mean scores over time for some individual effectiveness variables, including NDI, neck pain, arm pain,and SF-36 PCS, are shown in Fig. 2. In both groups theresults showed significant improvement over preoperativeresults for all of these measures (all p 0.001), with CDAshowing superiority at all intervals for improvements inNDI score (PPS 99.9% at 10 years) and neck pain score(PPS approximately 100.0% at 10 years). Mean improvements from preoperative results in arm pain score and SF36 PCS were numerically better for CDA than ACDF at alllong-term intervals, but did not consistently show statistical superiority.Radiographic MeasurementsDisc (FSU) height was maintained in both groups. FSUsuccess was defined as a 2-mm decrease either anteriorly or posteriorly from 6 weeks postoperatively. Therewere no statistical differences in FSU success betweentreatment groups for any long-term follow-up interval.FSU success rates at 10 years were 93.3% and 91.6% forCDA and ACDF, respectively (Fig. 3A). Angular range ofmotion (ROM) values at superior and inferior target levels on average were maintained in the CDA group, withno statistically significant changes from the preoperativeto 10-year results (Fig. 3B). Fusion success rates for theACDF group at 10 years were 95.2% at the superior level,97.9% at the inferior level, and 93.8% overall. Five of the6 patients with fusion failures had undergone secondarysurgeries before the 10-year evaluation.Patient and Physician PerceptionsAt 10 years postoperatively, 93.2% of CDA and 92.2%of ACDF patients reported that they were “definitely” or“mostly” satisfied; 92.5% and 87.8%, respectively, saidthey were helped as much as expected; and 93.2% and87.8%, respectively, said they would have the surgeryagain for the same condition. Patients rated the perceivedeffect of their surgical treatment from “completely recovered” to “vastly worsened.” At 10 years, 95.9% of the CDAgroup and 93.9% of the ACDF group perceived their resultas at least improved. The rates of physician perceptionsof results as successful based on a nonvalidated questionnaire were 98.0% and 80.0% for the two treatments, respectively.SafetyTable 2 summarizes cumulative rates (life-table estimations) of any type of AE through 10 years postoperativelyand comparisons between treatment groups by time-toevent analysis. The CDA group had a statistically lowerrate of any type of serious AE and a lower rate of possibly implant- or implant/procedure-related serious AEs.Cumulative rates of serious AEs (grade 3 or 4) that wereclassified as associated with implant or implant/surgicalprocedure were 3.8% in CDA and 8.1% in ACDF patientsthrough 10 years postoperatively (LHR [95% BCI] -0.92[-1.88, -0.01]), and the prevalence of specific serious implant or implant/surgical procedure–associated adverseevents is detailed in Table 3.The cumulative rates of any secondary surgery at treated levels through 10 years (Table 2) were 4.7% and 17.6%for the CDA and ACDF groups, respectively, a statistically significant difference (LHR [95% BCI] -1.39 [-2.15,-0.61]) favoring CDA. In CDA patients, the 6 removals alloccurred prior to the 5-year follow-up and have been previously described.15 In the ACDF group, “elective removals”occurred in 9 patients and were typically performed at thediscretion of the investigator while performing a surgicalprocedure on adjacent or other cervical levels requiringremoval of the plate and placement of a new plate. If weJ Neurosurg Spine Volume 31 October 2019511Unauthenticated Downloaded 08/24/22 10:04 PM UTC
Gornet et al.FIG. 1. Success rates over time for both the CDA and ACDF groups for the efficacy measures overall success (A), NDI success(B), and neurological success (C). PPS 95% considered statistically superior. Y years.exclude the 9 elective removals in the ACDF group fromthe statistical comparison, the rate of secondary surgeriesat index levels in the ACDF group (11.8% cumulative) isstill statistically greater than that for the CDA group (LHR[95% BCI] -1.00 [-1.85, -0.22]).Cumulative rates of second surgeries involving adjacentlevels through 10 years were 9.0% and 17.9% for CDA andACDF, respectively, a statistically significant difference(LHR [95% BCI] -0.66 [-1.29, -0.01]) in favor of CDA(Table 2). Figure 4 shows the Kaplan-Meier curves for timeto secondary surgeries at adjacent levels, indicating theconsistently lower rate in the CDA group over time, which512was statistically different by 10 years postoperatively (PPS 98.0%).Grading of heterotopic ossification (HO) was assessedby independent radiologists. The presence of any grade IIIor IV HO in the CDA group over time is summarized inTable 4. Although no serious HO AEs that were classifiedas likely to be implant related or clinically significant werereported by any investigators as part of their AE documentation (Table 3), there was radiographic evidence, reportedseparately by the independent radiologist reviewers, ofgrade IV HO at the superior (8.2%) and inferior (10.3%)treatment levels. The rate of HO of either grade III or IVJ Neurosurg Spine Volume 31 October 2019Unauthenticated Downloaded 08/24/22 10:04 PM UTC
Gornet et al.FIG. 2. Mean scores over time for both the CDA and ACDF groups for efficacy measures NDI score (A), neck pain score (B), armpain score (C), and SF-36 PCS score (D). For NDI, neck pain, and arm pain, a lower score indicates less disability or pain. For SF36 PCS, a higher score means better functioning. PPS based on the between-treatment comparisons of score improvements frompreoperative; PPS 95% considered statistically superior. M months; WK weeks.at either or both levels was 39.0% at 10 years postoperatively, not an increase from 7 years (42.4%). An additionalanalysis compared overall success rates at each follow-upinterval, including 10 years, between those with severe HO(grade III or IV) and those with nonsevere HO (grades 0–II) as measured at 2 and at 10 years (data not shown). Therewas no statistically significant difference in overall successrates between the HO severity subgroups at any follow-upinterval.DiscussionThis long-term follow-up study continues to show thenoninferiority of the Prestige LP Cervical Disc comparedto ACDF at two levels for symptomatic cervical DDD. At10 years postoperatively, CDA was noninferior comparedto ACDF on all effectiveness outcome measures. TheCDA group had statistically superior results compared toACDF in overall success rate (80.4% vs 62.2%), NDI success (88.4% vs 76.5%), and neurological success (92.6% vs86.1%). FSU height was maintained in both groups. Therate of clinically significant AEs (grade 3 or 4) that wereconsidered to possibly be associated with the implant orimplant/surgical procedure were significantly lower in theCDA group (3.8% vs 8.1%), as was the rate of secondarysurgeries (4.7% vs 17.6%). Finally, rates of secondary surgery involving an adjacent level up to 10 years after theclinical study treatment were significantly lower in theCDA group than the ACDF group (9.0% vs 17.9%, respectively).Presently, at least 7 CDA devices in the US have received FDA approval at either one or two cervical levels.Long-term results (4–7 years postoperatively) have beenpublished on several of these devices, primarily for singlelevel treatment.2,7,15,24,25,29 One 10-year single-level studyhas also been reported.16 These studies consistently shownoninferiority of CDA compared to ACDF, and most showsuperiority in overall success rates, lower rates of secondary surgeries, and low rates of serious AEs.There have been a number of reviews and meta-analyses of the CDA literature. Nunley et al. recently summarized the current state of evidence both in and outsidethe US regarding cervical disc arthroplasty.23 They notethat the US literature, consisting of predominantly level Ievidence from FDA-approved clinical trials, supports theuse of cTDR at one and two surgical levels in comparison to ACDF. They further conclude that the “volume oflevel I and II evidence supporting the efficacy of cTDR isunparalleled in the field of spine surgery.” Badve et al., reviewing the literature on one-level devices in an “expertreview,” also concluded that CDA resulted in favorablerates of long-term functional recovery, AEs, developmentof adjacent segment degeneration, and secondary surgeriesin comparison to ACDF.1 Both Nunley et al. and Badve etal. provide extensive referencing of the literature on CDAversus ACDF and related topics.J Neurosurg Spine Volume 31 October 2019513Unauthenticated Downloaded 08/24/22 10:04 PM UTC
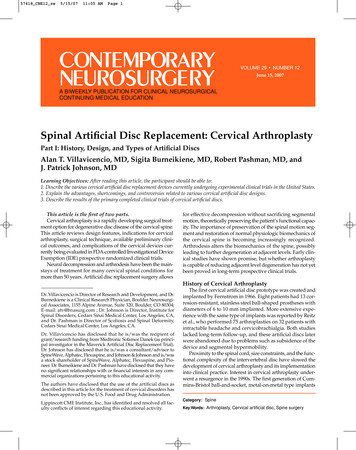
Gornet et al.FIG. 3. Radiographic outcomes. FSU success rates for the CDA and ACDF groups over time (A), with no statistical difference atany point of long-term follow-ups, and mean ROM over time at superior and inferior levels of the CDA patients (B). deg. degrees.TABLE 2. Patients who reported AEs and who underwent secondary surgeries through 10 years postoperatively,based on the life-table estimationAE Type*CDA,n 209AEAt least 1 of any AE type206 (99.1%)Any serious AE124 (66.7%)Possibly implant- or implant/procedure-related AE¶55 (31.7%)Serious, possibly implant- or implant/procedure-related AE7 (3.8%)Secondary surgerySecondary surgery at either index level**9 (4.7%)Revision0 (0.0%)Removal6 (3.1%)Elective removal0 (0.0%)Supplemental fixation2 (1.2%)Reoperation3 (1.6%)Supplemental fixation w/ bone growth stimulator0 (0.0%)Secondary surgery involving adjacent level(s)**16 (9.0%)ACDF,n 188LHR, Posterior Mean (95% BCI)†179 (97.3%)120 (70.9%)44 (25.0%)14 (8.1%)0.02 ( 0.18, 0.23)‡ 0.31 ( 0.57, 0.06)§0.04 ( 0.35, 0.45)‡ 0.92 ( 1.88, 0.01)§27 (17.6%)2 (1.4%)7 (4.1%)9 (6.4%)8 (5.4%)5 (3.0%)5 (2.8%)24 (17.9%) 1.39 ( 2.15, 0.61)§ 798.11 ( 1956.24, 0.60)‡ 0.35 ( 1.48, 0.80)‡ 802.74 ( 1959.04, 1.53) 1.81 ( 3.58, 0.17) 0.78 ( 2.32, 0.75)‡ 799.85 ( 1961.63, 1.23) 0.66 ( 1.29, 0.01)§Values are presented as number of patients (cumulative percentage) unless otherwise indicated.* WHO grade 3 or 4 AEs considered serious.† BCI in the HPD.‡ Not statistically different.§ CDA statistically less frequent than ACDF over the time period.¶ AE deemed to be associated with device or device/surgical procedure.** Some patients had more than one secondary surgery; some secondary surgeries involved both index and adjacent levels.514J Neurosurg Spine Volume 31 October 2019Unauthenticated Downloaded 08/24/22 10:04 PM UTC
Gornet et al.TABLE 3. Patients with grade 3 or 4 implant- or implant/surgical procedure–related AEs through 10 years, based on thelife-table estimationGrade 3 or 4 AEsDysphagia/dysphoniaHOImplant eventsNeck &/or arm painNeurologicalNonunionOtherOther painSpinal eventTraumaVascularWound (noninfectious)CDAACDFLHR, Posterior Mean (95% BCI)*7 (3.8)1 (0.6)0 (0.0)2 (1.0)3 (1.7)1 (0.7)0 (0.0)1 (0.5)1 (0.5)4 (2.0)0 (0.0)1 (0.5)0 (0.0)14 (8.1)1 (0.7)3 (1.6)3 (1.6)7 (4.6)2 (1.2)9 (5.0)0 (0.0)2 (1.6)5 (2.7)1 (0.6)0 (0.0)1 (0.5) 0.92 ( 1.88, 0.01) 0.23 ( 3.90, 3.35)† 798.33 ( 1957.40, 0.77)† 0.66 ( 2.70, 1.32)† 1.16 ( 2.63, 0.27)† 1.18 ( 4.23, 1.67)† 800.60 ( 1967.56, 1.75)797.35 ( 1.52, 1961.63)† 1.20 ( 4.28, 1.60)† 0.41 ( 1.82, 0.97)† 797.62 ( 1958.28, 1.34)†797.35 ( 1.52, 1961.63)† 795.68 ( 1959.00, 1.30)†Values are presented as number of patients (cumulative percentage) unless otherwise indicated.* BCI in the HPD.† Not statistically different.Recent meta-analyses that compare CDA to ACDF arebased on the large amount of published clinical trial datanow available, although few focus specifically on two-levelstudies.14,34–36,38 One meta-analysis included 19 randomizedcontrolled trials involving 4516 cases, the majority singlelevel, with short- and midterm follow
CLINICAL ARTICLE J Neurosurg Spine 31:508-518, 2019 ABBREVIATIONS ACDF anterior cervical discectomy and fusion; AE adverse event; BCI Bayesian credible interval; CDA cervical disc arthroplasty; cTDR cervical TDR; DDD degenerative disc disease; FSU functional spinal unit; HO heterotopic ossification; HPD highest posterior density; IDE investigational device