Transcription
DegenerativeCervical Myelopathyand RadiculopathyTreatment Approachesand OptionsMichael G. KaiserRegis W. HaidChristopher I. ShaffreyMichael G. FehlingsEditors123
Degenerative Cervical Myelopathyand Radiculopathy
Michael G. Kaiser Regis W. HaidChristopher I. ShaffreyMichael G. FehlingsEditorsDegenerative CervicalMyelopathy andRadiculopathyTreatment Approaches and Options
EditorsMichael G. KaiserColumbia University Medical CenterNew York, NYUSAChristopher I. ShaffreyDuke University Health SystemDurham, NCUSARegis W. HaidAtlanta Brain and Spine CareAtlanta, GAUSAMichael G. FehlingsToronto Western HospitalUniversity of TorontoToronto, ONCanadaISBN 978-3-319-97951-9 ISBN -97952-6(eBook)Library of Congress Control Number: 2018957703 Springer Nature Switzerland AG 2019This work is subject to copyright. All rights are reserved by the Publisher, whether the whole orpart of the material is concerned, specifically the rights of translation, reprinting, reuse ofillustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way,and transmission or information storage and retrieval, electronic adaptation, computer software,or by similar or dissimilar methodology now known or hereafter developed.The use of general descriptive names, registered names, trademarks, service marks, etc. in thispublication does not imply, even in the absence of a specific statement, that such names areexempt from the relevant protective laws and regulations and therefore free for general use.The publisher, the authors, and the editors are safe to assume that the advice and information inthis book are believed to be true and accurate at the date of publication. Neither the publisher northe authors or the editors give a warranty, express or implied, with respect to the materialcontained herein or for any errors or omissions that may have been made. The publisher remainsneutral with regard to jurisdictional claims in published maps and institutional affiliations.This Springer imprint is published by the registered company Springer Nature Switzerland AGThe registered company address is: Gewerbestrasse 11, 6330 Cham, Switzerland
ContentsPart I The Basics1 Functional Anatomy of the Spinal Cord . . . . . . . . . . . . . . . . . . 3Mario Ganau, Rahel Zewude, and Michael G. Fehlings2 Cervical Spine Biomechanics. . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Bryan S. Lee and Edward C. Benzel3 Cervical Alignment and Sagittal Balance. . . . . . . . . . . . . . . . . . 29Alexander Tuchman and Dominque M. O. Higgins4 Degenerative Cervical Myelopathy: A Spectrumof Degenerative Spondylopathies 37Aria Nouri, Jean-Christophe Murray,and Michael G. Fehlings5 Pathobiology of Cervical Radiculopathyand Myelopathy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53Cory J. Hartman and Daniel J. Hoh6 Natural History of Cervical Degenerative Disorders. . . . . . . . . 67John E. O’Toole and Joseph E. MolendaPart II Evaluation and Diagnosis of CervicalSpondylotic Disorders7 Fundamentals of Cervical Neurological Exam. . . . . . . . . . . . . . 77Meena Thatikunta and Maxwell Boakye8 Clinical Assessment Tools. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89Jian Guan and Zoher Ghogawala9 Radiographic Modalities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 97Ha Son Nguyen and Shekar N. Kurpad10 Alternative Diagnostic Tools. . . . . . . . . . . . . . . . . . . . . . . . . . . .Kurt M. Eichholz109v
ContentsviPart III Surgical Decision-Making11 Failure of Nonoperative Management . . . . . . . . . . . . . . . . . . . .Hamadi Murphy, Scott C. Wagner, Alex Vaccaro,and Stephen Silva12312 Timing of Operative Intervention. . . . . . . . . . . . . . . . . . . . . . . .Alexander M. Tucker, Tianyi Niu, Daniel T. Nagasawa,and Langston T. Holly12913 Surgical Approach Decision-Making. . . . . . . . . . . . . . . . . . . . .Mena G. Kerolus and Vincent C. Traynelis13914 Utility of Intraoperative Neuromonitoring. . . . . . . . . . . . . . . . .Randy S. D’Amico and Peter D. Angevine15315 Factors Predictive of Operative Outcome. . . . . . . . . . . . . . . . . .Jerry Ku and Jefferson R. Wilson16716 The Cost-Effectiveness of Various Surgical Proceduresin the Cervical Spine. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Blake N. Staub and Todd J. Albert17 An Overview of Various Surgical Approaches. . . . . . . . . . . . . .Matthew J. Tormenti and Mark R. McLaughlin177185Part IV Motion Preservation Surgery for CervicalDegenerative Disorders18 Posterior Laminoforaminotomy for Radiculopathy . . . . . . . . .James S. Harrop and John L. Gillick19719 Cervical Laminoplasty. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Lionel N. Metz, Grigoriy Arutyunyan, Deeptee Jain,Lee A. Tan, and K. Daniel Riew20720 Cervical Disc Arthroplasty. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Jau-Ching Wu, Praveen V. Mummaneni, and Regis W. Haid22121 MIS Approaches for Cervical Spondylotic Disease. . . . . . . . . .Mena G. Kerolus and Richard G. Fessler235Part V Fusion Techniques for Cervical Degenerative Disorders22 Anterior Cervical Discectomy and Fusion. . . . . . . . . . . . . . . . .Luis M. Tumialán24923 Anterior Cervical Corpectomy . . . . . . . . . . . . . . . . . . . . . . . . . .Anthony C. Lau and Allan D. Levi27124 Multilevel ACDF Versus Corpectomy. . . . . . . . . . . . . . . . . . . . .Hani R. Malone and Michael G. Kaiser287
Contentsvii25 Options for Interbody Grafting. . . . . . . . . . . . . . . . . . . . . . . . . .Azam Basheer, Mohammed Macki, and Frank La Marca30926 Anterior Fixation Plating. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Harel Deutsch and Mena G. Kerolus31927 Cervical Laminectomy and Fusion. . . . . . . . . . . . . . . . . . . . . . .Jacob Januszewski and Juan S. Uribe32928 Biological Enhancers of Fusion. . . . . . . . . . . . . . . . . . . . . . . . . .Matthew F. Gary and Scott D. Boden341Part VI Challenges of Cervical Fixation29 Occipitocervical Stabilization . . . . . . . . . . . . . . . . . . . . . . . . . . .Robert F. Heary and Nitin Agarwal35130 Alternative Means of Posterior Cervical Stabilization . . . . . . .Hsuan-Kan Chang, David McCarthy, and Michael Y. Wang36131 Atlantoaxial Stabilization. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Avery L. Buchholz, John C. Quinn, Christopher I. Shaffrey,and Justin S. Smith37332 Reconstructive Procedures in the Osteoporotic Patient . . . . . .Jacob Januszewski and Juan S. Uribe38533 The Cervicothoracic Junction. . . . . . . . . . . . . . . . . . . . . . . . . . .Anthony M. DiGiorgio, Michael S. Virk, Ming- Hsiao Hu,Mohanad Alazzeh, Santan Thottempudi,and Praveen V. Mummaneni39534 Osteotomy for Cervical Kyphosis . . . . . . . . . . . . . . . . . . . . . . . .Joseph A. Osorio, Justin K. Scheer, Derek G. Southwell,and Christopher P. Ames409 Index. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .421
ContributorsNitin Agarwal, MD Department of Neurological Surgery, University ofPittsburgh Medical Center, Pittsburgh, PA, USAMohanad Alazzeh, BS University of California, San Francisco, CA, USATodd J. Albert, MD Hospital for Special Surgery, New York, NY, USAChristopher P. Ames, MD Department of Neurological Surgery, Universityof California, San Francisco, CA, USAPeter D. Angevine, MD Department of Neurological Surgery, ColumbiaUniversity Medical Center, New York, NY, USAGrigoriy Arutyunyan, MD Department of Orthopedic Surgery, UCSFMedical Center, San Francisco, CA, USAAzam Basheer, MD Department of Neurosurgery, Neuroscience Institute,Henry Ford Health System, Detroit, MI, USAEdward C. Benzel, MD Department of Neurosurgery, Center for SpineHealth, Neurological Institute, Cleveland Clinic Foundation, Cleveland, OH,USAMaxwell Boakye, MD, MPH, MBA, FACS Department of Neurosurgery,University of Louisville, Louisville, KY, USAScott D. Boden, MD Department of Orthopaedic Surgery, Emory UniversitySchool of Medicine, Atlanta, GA, USAAvery L. Buchholz, MD, MPH Department of Neurological Surgery,Medical University of South Carolina, Charleston, SC, USAHsuan-Kan Chang, MD Department of Neurological Surgery andRehabilitation Medicine, University of Miami Miller School of Medicine,Miami, FL, USARandy S. D’Amico, MD Department of Neurological Surgery, ColumbiaUniversity Medical Center, New York, NY, USAHarel Deutsch, MD Department of Neurologic Surgery, Rush UniversityMedical Center, Chicago, IL, USAAnthony M. DiGiorgio, DO, MHA Department of Neurological Surgery,University of California, San Francisco, CA, USAix
xDepartment of Neurological Surgery, Louisiana State University HealthSciences Center, New Orleans, LA, USAKurt M. Eichholz, MD, FACS, FAANS St. Louis Minimally Invasive SpineCenter, St. Louis, MO, USAMichael G. Fehlings, MD, PhD, FRCSC, FACS Division of Neurosurgeryand Spine Program, Toronto Western Hospital, University of Toronto,Toronto, ON, CanadaRichard G. Fessler, MD Department of Neurosurgery, Rush University,Chicago, IL, USAMario Ganau, MD, PhD Division of Neurosurgery and Spine Program,Toronto Western Hospital, University of Toronto, Toronto, ON, CanadaMatthew F. Gary, MD Department of Orthopaedic Surgery, EmoryUniversity School of Medicine, Atlanta, GA, USAZoher Ghogawala, MD, FACS Department of Neurosurgery, LaheyHospital and Medical Center, Burlington, MA, USADepartment of Neurosurgery, Tufts University School of Medicine, Boston,MA, USAJohn L. Gillick, MD Department of Neurosurgery, Thomas JeffersonUniversity, Philadelphia, PA, USADepartment of Neurosurgery, Rutgers-New Jersey Medical School, Newark,NJ, USAJian Guan, MD Department of Neurosurgery, University of Utah, Salt LakeCity, UT, USAAlan L. and Jacqueline Stuart Spine Center, Department of Neurosurgery,Lahey Hospital and Medical Center, Burlington, MA, USARegis W. Haid, MD Atlanta Brain and Spine Care, Atlanta, GA, USAJames S. Harrop, MD, FACS Department of Neurological and OrthopedicSurgery, Division of Spine and Peripheral Nerve Surgery, Delaware ValleySCI Center, Thomas Jefferson University, Philadelphia, PA, USACory J. Hartman, MD Department of Neurosurgery, University of Florida,Gainesville, FL, USARobert F. Heary, MD Department of Neurological Surgery, Rutgers NewJersey Medical School, Newark, NJ, USADominque M. O. Higgins, MD, PhD Department of Neurological Surgery,Columbia University Medical Center, New York, NY, USADaniel J. Hoh, MD Department of Neurosurgery, University of Florida,Gainesville, FL, USALangston T. Holly, MD Department of Neurosurgery, University ofCalifornia-Los Angeles, Los Angeles, CA, USAContributors
ContributorsxiMing-Hsiao Hu, MD Institute of Biomedical Engineering, College ofMedicine and College of Engineering, National Taiwan University, Taipei,TaiwanDepartment of Orthopedics, National Taiwan University College of Medicineand National Taiwan University Hospital, Taipei, TaiwanDeeptee Jain, MD Department of Orthopedic Surgery, UCSF MedicalCenter, San Francisco, CA, USAJacob Januszewski, MD Department of Neurosurgery and Brain Repair,University of South Florida, Tampa, FL, USAMichael G. Kaiser, MD, FACS, FAANS Department of NeurologicalSurgery, Columbia University Medical Center, New York, NY, USAMena G. Kerolus, MD Department of Neurosurgery, Rush UniversityMedical Center, Chicago, IL, USAJerry Ku, MD Division of Neurosurgery, St. Michael’s Hospital, Universityof Toronto, Toronto, ON, CanadaShekar N. Kurpad, MD, PhD Department of Neurosurgery, MedicalCollege of Wisconsin, Milwaukee, WI, USAFrank LaMarca, MD Department of Neurosurgery, Henry Ford HealthSystem, Detroit, MI, USAAnthony C. Lau, MD Department of Neurological Surgery, University ofMiami Miller School of Medicine, Miami, FL, USABryan S. Lee, MD Department of Neurosurgery, Center for Spine Health,Neurological Institute, Cleveland Clinic Foundation, Cleveland, OH, USAAllan D. Levi, MD Department of Neurological Surgery, University ofMiami Miller School of Medicine, Miami, FL, USAMohammed Macki, MD Department of Neurosurgery, Henry FordHospital, Detroit, MI, USAHani R. Malone, MD Department of Neurological Surgery, ColumbiaUniversity Medical Center, New York, NY, USADavid McCarthy, BS Department of Neurological Surgery andRehabilitation Medicine, University of Miami Miller School of Medicine,Miami, FL, USAMark R. McLaughlin, MD, FACS, FAANS Princeton Brain and SpineCare, LLC, Princeton, NJ, USALionel N. Metz, MD Department of Orthopedic Surgery, UCSF MedicalCenter, San Francisco, CA, USAJoseph E. Molenda, MD Department of Neurosurgery, Rush UniversityMedical Center, Chicago, IL, USAPraveen V. Mummaneni, MD Department of Neurological Surgery,University of California, San Francisco, CA, USA
xiiHamadi Murphy, MD, MS Department of Orthopaedics, Rothman Instituteat Thomas Jefferson University Hospital, Philadelphia, PA, USAJean-Christophe Murray, MD, FRCSC Division of Neurosurgery andSpine Program, Toronto Western Hospital, University of Toronto, Toronto,ON, CanadaDaniel T. Nagasawa, MD Department of Neurosurgery, University ofCalifornia-Los Angeles, Los Angeles, CA, USAHa Son Nguyen, MD Department of Neurosurgery, Medical College ofWisconsin, Milwaukee, WI, USATianyi Niu, MD Department of Neurosurgery, University of California-LosAngeles, Los Angeles, CA, USAAria Nouri, MD, MSc Department of Neurosurgery, Yale University andUniversity of Cincinnati, Cincinnati, OH, USAJohn E. O’Toole, MD Department of Neurosurgery, Rush UniversityMedical Center, Chicago, IL, USAJoseph A. Osorio, MD, PhD Department of Neurological Surgery,University of California, San Francisco, CA, USAJohn C. Quinn, MD Department of Neurosurgery, University of VirginiaHealth System, Charlottesville, VA, USAK. Daniel Riew, MD The Spine Hospital, Columbia University MedicalCenter, New York, NY, USAJustin K. Scheer, MD Department of Neurosurgery, University of Illinois atChicago, Chicago, IL, USAChristopher I. Shaffrey, MD Departments of Orthopaedic and NeurologicalSurgery, Duke University Health System, Durham, NC, USAStephen Silva, BA Department of Orthopaedics, Rothman Institute atThomas Jefferson University Hospital, Philadelphia, PA, USAJustin S. Smith, MD, PhD Department of Neurological Surgery, Universityof Virginia Health System, Charlottesville, VA, USADerek G. Southwell, MD, PhD Department of Neurological Surgery,University of California, San Francisco, CA, USABlake N. Staub, MD Texas Back Institute, Plano, TX, USALee A. Tan, MD The Spine Hospital, Columbia University Medical Center,New York, NY, USAMeena Thatikunta, MD Department of Neurosurgery, University ofLouisville, Louisville, KY, USASantan Thottempudi University of California, San Francisco, CA, USAMatthew J. Tormenti, MD, FACS, FAANS Princeton Brain and Spine,Langhorne, PA, USAContributors
ContributorsxiiiVincent Traynelis, MD Department of Neurosurgery, Rush UniversityMedical Center, Chicago, IL, USAAlexander Tuchman, MD Department of Neurological Surgery, ColumbiaUniversity Medical Center, New York, NY, USAAlexander Tucker, MD Department of Neurosurgery, University ofCalifornia-Los Angeles, Los Angeles, CA, USALuis M. Tumialán, MD Department of Neurosurgery, Barrow NeurologicalInstitute, St. Joseph’s Hospital and Medical Center, Phoenix, AZ, USAJuan S. Uribe, MD Department of Neurosurgery and Brain Repair,University of South Florida, Tampa, FL, USAAlex Vaccaro, MD, PhD, MBA Department of Orthopaedics, RothmanInstitute at Thomas Jefferson University Hospital, Philadelphia, PA, USAMichael S. Virk, MD, PhD Department of Neurosurgery, University ofCalifornia, San Francisco, CA, USAScott C. Wagner, MD Department of Orthopaedics, Rothman Institute atThomas Jefferson University Hospital, Philadelphia, PA, USAMichael Y. Wang, MD, FACS Department of Neurological Surgery andRehabilitation Medicine, University of Miami Miller School of Medicine,Miami, FL, USAJefferson R. Wilson, MD, PhD, FRCSC Division of Neurosurgery, St.Michael’s Hospital, University of Toronto, Toronto, ON, CanadaJau-Ching Wu, MD, PhD Department of Neurosurgery, Taipei Veteran’sGeneral Hospital, Taipei, TaiwanSchool of Medicine, National Yang-Ming University, Taipei, TaiwanRahel Zewude, BSc Division of Neurosurgery and Spine Program,Toronto Western Hospital, University of Toronto, Toronto, ON, Canada
Part IThe Basics
1Functional Anatomy of theSpinal CordMario Ganau, Rahel Zewude,and Michael G. Fehlings Basic Anatomy of the Spinal Cordnumbered after the vertebra just rostral to therespective foramen through which they pass (i.e.,Located in the upper two-thirds of the spinal T12 nerves are caudal to the T12 vertebral body).canal, within the hollow portion of a multiarticu- Conversely, the cervical nerves are numbered forlated flexible structure called the vertebral col- the vertebral body just caudal (i.e., the C1 nerveumn, the SC has a length of approximately 45 cm roots are rostral to the C1 vertebral body, whilein humans. The vertebral column is divided into the C8 nerves are rostral to the body of T1). Thiscervical, thoracic or dorsal, lumbar, and sacro- distribution explains the different lengths and oricoccygeal vertebral segments. Each vertebral entation of each pair of nerve roots: in fact, sincesegment is formed by bony and cartilaginous the SC is shorter than the vertebral column, thecomponents, known as a functional spinal unit lumbar and sacral nerves develop long roots run(FSU). The FSU can be defined as the smallest ning caudally below the conus medullaris in thephysiological motion segment of the vertebral spinal cistern to form the cauda equina.column capable of motion that exhibits biomeThe three meningeal layers surrounding thechanical characteristics similar to those of the SC are a continuation of those found around theentire spine [18]. The SC extends from the fora- brain. The most external layer, the dura mater,men magnum at the base of the skull to a cone- does not adhere to the vertebral bone, contrary toshaped termination, the conus medullaris, which the dura of the brain. The spinal dura terminatesis anchored caudally to the coccyx through a non- with a cul-de-sac at the sacral level (S1–S2)neural filament known as the filum terminale. forming the dural sac. Overlying the dura is theNerve fibers emerge from the SC in an uninter- epidural space, containing fat and vessels, andrupted series of dorsal and ventral roots, which underlying the dura is the arachnoid space, conjoin to form 31 spinal nerves: 8 cervical, 12 tho- taining the cerebrospinal fluid (CSF). The thirdracic or dorsal, 5 lumbar, 5 sacral, and 1 coccy- meningeal layer, the pia mater, follows the congeal. The thoracic, lumbar, and sacral nerves are tours of the SC as well as the arteries and veinssupplying the SC; of note, the pia is firmlyattached to the dura by a series of 22 denticulateligaments. These ligaments begin at the foramenmagnum and are located on each side of the cordM. Ganau · R. Zewude · M. G. Fehlings (*)in the interval between two adjacent spinal nerveDivision of Neurosurgery and Spine Program,roots, being attached to the SC roughly halfwayToronto Western Hospital, University of Toronto,between the dorsal and ventral nerve root entryToronto, ON, Canadae-mail: Michael.Fehlings@uhn.ca Springer Nature Switzerland AG 2019M. G. Kaiser et al. (eds.), Degenerative Cervical Myelopathy and 952-6 13
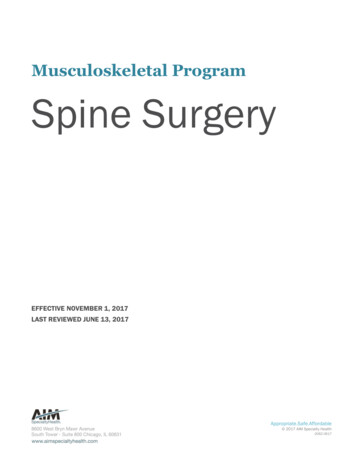
M. Ganau et al.4zones. The meningeal layers and the compartments they create represent important anatomicalregions: the epidural space is where anestheticdrugs are injected to induce local anesthesia during surgical procedures or childbirth; and thearachnoid space in the lumbar cistern, extendingfrom L2 to S2, is the ideal place for CSF collection and injection of drugs or contrast mediumthrough lumbar puncture (ideally performed atthe L3/4, L4/5 or L5/S1 interlaminar spaces). EmbryologyThe neural tube is the primordial structure forthe CNS, with the neural crest appearing atapproximately 20 days of gestation and givingrise to a number of neural and nonneural derivatives (including neurons, meningeal cells, etc.).During the third week of gestation, mesenchymal tissue from the mesoderm differentiates intosegmented somites. The segmented somites arebilateral structures that develop on either side ofthe notochord while distending the overlyingectoderm. These somites differentiate into thesclerotome and myodermatome during the fourthweek of gestation. The genes regulating thedirection and order of the craniocaudal axisdevelopment and differentiation are known asHox genes: spinal congenital anomalies mayresult from their mutations [15]. Adjacent to theneural tube are 31 pairs of somites; those embryonic segmental structures differentiate into muscles as well as bony and connective tissues,which are arranged in sequence from the firstcervical through the coccygeal levels. Each pairof nerves develops in association with each pairof somites. The apparent segmentation of the SCis dependent upon the development of pairedsegmental spinal nerves and radicular vessels onboth sides of the midline. The bilateral neuralcrest in fact becomes segmented into pairedunits, one pair for each future sensory dorsal rootganglion of each spinal nerve.Up to the third fetal month, the SC extendsthroughout the entire length of the developingvertebral column. The growth of the SC over thesubsequent months leads to the elongation of theroots of the spinal nerves between the SC and theintervertebral foramina, so that at birth the caudalend of the SC is located at the level of L3. As aresult of canalization and retrogressive differentiation, an ependymal lined space known as thecentral canal forms at the innermost portion ofthe SC and terminates at the conus medullariswith the ventriculus terminalis, or fifth ventricle[5]. This structure, which is filled with CSF, isdescribed in the literature as a normal developmental phenomenon, especially in newborns andduring childhood, with regression in the adultlife. Persistence of this structure may in fact leadto a pathological condition called dilatation ofthe ventriculus terminalis [9]. Functional Spinal SegmentsEach portion of the SC where the correspondingpairs of ventral and dorsal roots attach is called aspinal segment. As such, each spinal segment(except the upper cervical segments) is locatedslightly higher than the respective FSU. The rootletsforming each nerve root enter the root sleeve afterpassing obliquely, laterally, and caudally within thevertebral canal. The sleeve contains motor and sensory roots separated by the interradicular septum.The dorsal and ventral roots come together andform the spinal nerve root. Before forming the spinal nerve root, the dorsal root contains an ovalenlargement called the dorsal root ganglion.The cell bodies of motor neurons and interneurons are located in an area of gray matterwithin the SC, characterized by a butterfly-likeshape. The white matter surrounding this graymatter structure is made of the nerve fibers andglia of ascending and descending tracts, as shownin Fig. 1.1. As a result, the nerve fibers of the graymatter are oriented in the transverse plane,whereas those of the white matter are oriented inthe longitudinal plane parallel to the neuraxis.The gray matter has been parceled anatomically,primarily on the basis of the microscopic appearance, into nuclei and laminae. This organizationis often referred to as being composed of tenlaminae, named after the anatomist Rexed, resulting in a posterior horn (laminae I through VI), an
15Functional Anatomy of the Spinal Cordintermediate zone (lamina VII), an anterior horn(laminae VIII to IX), and a region surroundingthe central canal (lamina X) [19]. Figure 1.1 andTable 1.1 provide details regarding the anatomical organization of the ten Rexed laminae andtheir specific functions.The horns of the gray matter contain differentclasses of functional neurons: second-orderinterneurons in the dorsal horn process sensoryinformation from the first-order sensory affer-Fig. 1.1 Anatomical distribution of Rexed laminaeents; this may eventually result in di-, tri-, orpolysynaptic pathways [6, 7]. Ventral horns contain motoneurons of various types: fundamentally, α-motoneurons innervating skeletal musclefibers and γ-motoneurons innervating extrafusalmotor fibers in muscle spindles.As the rostrocaudal distribution of motor neurons follows the body scheme, with more rostralsegments innervating muscles of more proximaljoints and vice versa, the SC shows two enlargedsegments innervating the upper (cervical or brachial enlargement; C5–T1) and lower extremities(lumbosacral enlargement; L3–S2). Also, the spatial distribution of motoneurons within the ventralhorn is structurally organized with those innervating axial or proximal muscles located more medially, and those innervating distal muscles in upperand lower extremities located more laterally.Finally, the lateral horn is found at the thoracicand upper lumbar segments only and containspreganglionic sympathetic neurons whose axonsreach the sympathetic ganglia adjacent to thevertebral bodies through white communicatingrami from the ventral roots. PreganglionicTable 1.1 Anatomy and function of Rexed laminaeLaminaIAnatomical locationPosteromarginal nucleusFibersAδIIIIISubstantia gelatinosaNucleus propriusCA-bIVNucleus propriusA-bVNucleus dorsalisAδ, CVINucleus dorsalisVIIIntermediolateral (IML) cellcolumn, intermediate gray,intermediomedial (IMM) cellcolumnVIIIAnterior r tractC8–L3: nucleus dorsalisT1–L2: IMLS2–S4 preganglionic sacralautonomic nucleusDescending tractsIXAnterior hornSomatic α- and γ-motor neuronsXPerimeter of the central canalAnterior commissure tractsFunction of fibersSensation of temperature andfast painSensation of slow painMechanoreceptors for touchand proprioceptionMechanoreceptors for touchand proprioceptionReceives information on painsensation and movementSpinal reflexes, integration ofsomatic motor functionPreganglionic parasympatheticneuronsModulate muscular tone andmovementInnervation of extrafusal fibersof skeletal muscleInnervation of intrafusal fibersof neuromuscular spindlesDecussation of axons
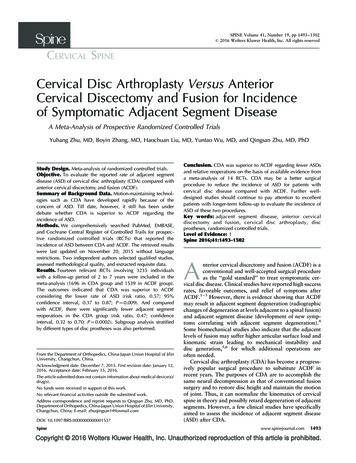
M. Ganau et al.6parasympathetic neurons are located similarly atthe S2–S4 levels for visceral innervations [21].Different classes of spinal interneurons areinvolved in the process of sensory-motor integration, typically being localized in Rexed laminaeVII and VIII. Experimental studies have documented how this integration of motor commandsand sensory feedback signals is used to controlmuscle activity during movement. The sum ofconvergent inputs from sensory neurons and fromthe central pattern generator (CPG), neural networks that produce rhythmic patterned outputswithout sensory feedback, gives rise to the activity of the interneurons. During locomotion, thefiring level of interneurons is modulated via excitation or inhibition depending on the reflex pathways, so that different patterns of interneuronalactivity determine which pathways are open,blocked, or modulated at any given moment [20]. Spinal PathwaysThe white matter is organized within the SC intothe following three columns: posterior, lateral,and anterior. Those fibers form tracts that eventually represent the components of sensory, motor,propriospinal, and autonomic pathways; Fig. 1.2provides further anatomical details of these tracts.The posterior column is found between theposterior horns of the gray matter, and it isdivided by the posterior median septum in themidline. The posterior column contains the fasciculus cuneatus laterally and the fasciculus gracilis medially. These tracts carry ascendinginformation of proprioception, vibration, andlight touch sensation. Fasciculus gracilis carriesinformation from lower limbs while fasciculuscuneatus carries information from upper limbs.The lateral column lies between the dorsal andventral root entry zones. It is composed of the lateral corticospinal tract and the lateral spinothalamic tract. The lateral corticospinal tract carriesdescending information regarding voluntarymotor function. The lateral corticospinal tract,along with the small anterior corticospinal tract,and the very small anterior lateral corticospinaltract make up the cortical spinal system. With theexception of axons from the anterior corticospinal tract, the axons in corticospinal tract crossover at the pyramids of the medulla. The lateralspinothalamic tract carries ascending information for pain and thermal sensation. This tractdecussates upon entry to the spinal cord and as aresult carries the impulses from the contralateralside of the body. In the posterior lateral peripheryof the spinal cord, the posterior spinocerebellartract is found. This tract is an uncrossed tract thatcarries ascending information regarding finecoordination of limb movement and posture.The anterior column of the white matter isfound between the anterior median fissure and theFig. 1.2 Cross-sectional diagram of the spinal cord with details of ascending and descending tracts
1Functional Anatomy of the Spinal Cordanterior root entry zone. This column containsthe anterior corticospinal tract and the anteriorspinothalamic tract. The ascending fibers of theanterior spinothalamic tract convey impulsesassociated with light touch. The anterior corticospinal tract is a descending uncrossed tractresponsible for fine motor skills. Fibers and Spinal NervesThe fibers contained within each spinal nerve canbe responsible for general somatic (innervatingthe outer body and extremities) or general visceral(innervating the internal organs) functions andtherefore can be either afferent or efferent depending on their primarily senso
2 Cervical Spine Biomechanics . Bryan S. Lee and Edward C. Benzel 3 Cervical Alignment and Sagittal Balance. 29 Alexander Tuchman and Dominque M. O. Higgins 4 Degenerative Cervical Myelopathy: A Spectrum . 20 Cervical Disc Arthroplasty. 221 Jau-Ching Wu, Praveen V. Mummaneni, and Regis W. Haid .