Transcription
SAN ANTONIO BRAC 2005GROWTH MANAGEMENT PLANTASK 6a REPORTREDISTRIBUTION OF HEALTHCAREAS A RESULT OF THEWILFORD HALL MEDICAL CENTER (WHMC)REALIGNMENTPREPARED FORCITY OF SAN ANTONIOOFFICE OF MILITARY AFFAIRSBYTHE DILUZIO GROUP, LLCSAN ANTONIO, TXSEPTEMBER 20081
SAN ANTONIO BRAC 2005 GROWTH MANAGEMENT PLANTASK 6a REPORTREDISTRIBUTION OF HEALTHCAREAS A RESULT OF THEWILFORD HALL MEDICAL CENTER (WHMC) REALIGNMENTTABLE OF CONTENTSSUBJECTPAGEAcronyms and Glossary of Terms .Introduction .Findings and Conclusions .Population Growth .Healthcare Redistribution.Trauma .Introduction .ii123388The Relationship of Trauma to Emergency Medicine.9San Antonio as a Trauma Center for the Region .9Trauma and Hospitals . 10Military/Civilian Trauma Care Relationships . 11Analysis of BRAC Impacts . 12Growth in Service Needs. 12Travel Time . 13University Hospital Expansion . 14Contingency Plans. 16Appendix A: Supporting InformationSan Antonio Military Medical Center Services Diagram. A-1TRICARE Program Definitions. A-2AHA 2007 Hospital Guide Data for Hospitals in San Antonio . A-3Map of Hospitals in and Around San Antonio, Texas. A-5Map of State Trauma Service Area P. A-6Emergency Transports to Area Hospitals in 2007 . A-6STRAC Hospital Listing. A-7STRAC Contingency Planning Task Force for Military Mobilization Diagram A-9STRAC CPTF Operational Guidelines . A-10MTTF Trauma & Healthcare Delivery Working Group Members . A-11iSan Antonio BRAC 2005 Growth Management Plan – Task 6a Report
Acronyms and Glossary of Terms59th Medical Wing – Wilford Hall Medical CenterAHA – American Hospital AssociationAir Life – San Antonio regional air ambulance serviceAMR – The regional ambulance systemBAMC – Brooke Army Medical CenterBRAC – Base Realignment and ClosureCatchment area – A defined geographical area from which a hospital’s patients are drawnCode 3 – An Emergency Medical Services trauma severity code. Most severely injuredCPTF – Contingency Planning Task ForceDoD – The United States Department of DefenseDesign beds – The number of beds a hospital was designed to accommodateStaffed beds – The number of beds for which the facility has nurses and support staffEMS – Emergency Medical ServicesER – Emergency RoomFEDS-HEAL – Federal Strategic AllianceGIS map – Geographic Information System mapGMP – Growth Management PlanGSAHC – Greater San Antonio Hospital CouncilGWOT – Global War on TerrorICU – Intensive Care UnitJTTR – Joint Theater Trauma RegistryJTTS – Joint Theater Trauma SystemLevel I Trauma Center – Highest level trauma care capability. In-house specialty careLevel II Trauma Center – Same as Level 1 except there is no research capabilityLevel III Trauma Center – Comprehensive care where specialists are available within 30 min.Level IV Trauma Center – Basic trauma stabilization and transportMHS – Military Health SystemMTF – Military Treatment Facility. A medical facility (hospital, clinic, etc.) owned and operated bythe uniformed services—usually located on or near a military base.MTTF – Military Transformation Task ForceMEDCOM – Medical Communications clearinghouse for patient transfersMFP – Master Facility PlanMRR – Medical Readiness ReviewOM&MFR – Operational Medicine and Medical Force ReadinessOR – Operating roomPDHA – Post Deployment Health AssessmentPDHRA – Post Deployment Health Re-AssessmentSAIO – San Antonio Integration OfficeSAMBIO – San Antonio Medical BRAC Integration OfficeSAMMC – San Antonio Military Medical CenterSAMMC- N – San Antonio Military Medical Center North – formerly Brooke Army Medical Center SAMMC-S –San Antonio Military Medical Center South, formerly Willford Hall Medical CenterSTRAC – Southwest Texas Regional Advisory CouncilTBI – Traumatic Brain InjuryTRICARE – The health care program serving active duty service members, National Guardand Reserve members, retirees, their families, survivors and certain former spouses.(See Appendix A for a definition of Alternative TRICARE Programs)UHS – University Health System, including University Hospital at the South Texas Medical CenterWHMC – Wilford Hall Medical Center, SAMMC SouthWT – Warrior in Transition (Returning from deployment)iiSan Antonio BRAC 2005 Growth Management Plan – Task 6a Report
SAN ANTONIO BRAC 2005 GROWTH MANAGEMENT PLANREDISTRIBUTION OF HEALTH CARE AS A RESULT OF REALIGNMENT OF WILFORD HALL MEDICAL CENTERTASK 6A REPORTINTRODUCTIONThe Growth ManagementTask 1: BRAC Community and Economic Impacts Analysisplanning process includesTask 2: San Antonio Military Medical Center Publiceight mandatory tasks,Transportationshown in the figure at theright. This report responds toTask 3: Fort Sam Houston Off-Post and On-PostTask 6a. It builds on theTransportation Infrastructureplanning documentTask 4: Fort Sam Houston Commercial Revitalization and"Conceptual Plan forReuse of Army Surplus PropertyAdjusting to Change inTask 5: Fort Sam Houston Sustainable NeighborhoodMilitary Medicine in SanRevitalization and Redevelopment PlanningAntonio" dated May 13,2005, and generated by theTask 6a: Redistribution of Health Care as a Result ofCity of San Antonio throughRealignment of Wilford Hall Medical Center (WHMC)an advance planning effortTask 6b Military Clinical Trainingfunded by the Office ofTask 7: Regional Coordination and CommunicationsEconomic Assistance withinthe Department of Defense.Task 8: Integrate Work Accomplished for Tasks 1- 7 into aIn addition, the study hasGrowth Management Planinvolved coordination withFort Sam Houston andWilford Hall Medical Center. The City works in cooperation with a Military TransformationTask Force that includes Bexar County and the Greater San Antonio Chamber ofCommerce. The task force has seven standing committees that correspond to assignedtasks outlined above. All work on this task has been accomplished in coordination with theMilitary Transformation Task Force – Health Care Services Delivery and MedicalPartnership Committee, which includes military representatives.In accordance with 2005 BRAC recommendations the city’s two big military medicalplatforms, Brooke Army Medical Center (BAMC) at Fort Sam Houston and portions of the59th Medical Wing's Wilford Hall Medical Center (WHMC) at Lackland Air Force Base areto be consolidated at Fort Sam Houston, to become the jointly staffed 425-bed SanAntonio Regional Medical Center North (SAMMC-N). Trauma care at Wilford Hall will beclosed. Wilford Hall will become a world-class outpatient and ambulatory surgery centerwhich will be designated as San Antonio Military Medical Center South (SAMMC-S).The San Antonio Military Medical Center (SAMMC), which includes SAMMC-N andSAMMC-S, will provide the full spectrum of medical care and support five separateCenters of Excellence, including the Cardio-Vascular Center, the Battlefield Health &Trauma Center, the Eye Center; the Maternal Child Care Center and the Amputee Center.(Source: San Antonio Integration Office {SAIO} briefing on Medical Integration).1San Antonio BRAC 2005 Growth Management Plan – Task 6a Report
FINDINGS AND CONCLUSIONSThis task has addressed possible implications of BRAC decisions on civilian hospitals.Specific questions that the plan was to address include:1. Possible displacement of patient load from military to civilian hospitals2. Possible implications of realignment of Level 1 Trauma and in-patient careThe GMP also addresses certain civilian health care needs seemingly related to BRAC.In summary, the findings in each of the foregoing study areas are:1. The military hospitals are handling an ever growing caseload. However, there is stilla small movement of patient load from military health care providers to civilianhealth care providers. That movement has nothing to do with BRAC. It stems,instead, from a variety of factors, principally a priority need for military hospitals totreat casualties. A secondary factor is the continued gradual increase in the generalmilitary health care beneficiary population. These and other factors are leading to aminor displacement of care to the civilian system. The civilian system is addingcapacity, and can easily handle this small incremental case load.2. Overall impacts of BRAC on medicine in San Antonio will be small, and to the extentthat there are such impacts, they areexpected to increase capability.The overall study conclusion is3. BRAC will have no significant impact onthat closure of the WHMC ERtrauma care relationships in the City.will have no significant longThe military fully expects to continue theterm impact on patient care oncooperative relationship which exists,the southwest side of theand BRAC improvements are expectedto more than off-set a slight increase inmetropolitan area.travel distance for the small number ofLevel 1 trauma cases that arise in thevicinity of Wilford Hall and are currently seen there.4. A general review of health care needs was clearly beyond the scope of the GMP,however some needs were or are apparent, and those are reported here.a. The primary civilian health care question the GMP addressed was the needfor the expansion of University Hospital. There was a clear need at the startof the study period. While there were many causes, this need had nothing todo with BRAC. The principal concern, in terms of inclusion as an area ofinquiry for the GMP, was an extremely heavy case load, which could havemeant that the University Hospital would have had difficulty handling evensmall BRAC-related impacts. During the course of the study, the UniversityHospital System has announced a major expansion program. This expansionprogram is expected to fully address concerns that prompted inclusion ofsuch tasking in the GMP study (For details, acility-plan/default.shtml).b. There is an expressed need for more ambulances to respond to the everincreasing number of emergency calls. Staging of such ambulances couldreduce the response time for patients from the vicinity of WHMC who mighthave been taken there prior to closure of their Level One Trauma Center.2San Antonio BRAC 2005 Growth Management Plan – Task 6a Report
This is a small number, and the need arises principally from populationgrowth and traffic growth in the expanding metropolitan area.c. There is a similar need for expansion of Air Life Services.POPULATION GROWTHConsideration of the impacts of BRAC is complicated by the rapidly changing San Antoniolandscape. Population growth in the Greater San Antonio area is impressive.The greater San Antonio area is now one of the fastest growing cities in the nation. BexarCounty is growing at a rate of more than 2% per year. In addition, the five most populatedadjoining counties continue to grow even faster. The population needing health care andcontributing to the trauma load is expected to exceed two million people by 2011. This isthe equivalent of adding another city the size of Amarillo or Lubbock to the currentworkload. (Source: U. S. CensusBureau).HEALTHCAREREDISTRIBUTIONThere is every intention andevery expectation that SAMMCwill continue to provide thecurrent level of care for themilitary beneficiary populationin San Antonio.At the beginning of the study, someconcerns were expressed that BRACchanges might displace care into thecivilian health care system. As the studyhas progressed, these concerns havebeen put to rest. The principal conclusion ofthe study is that some displacement of careBy 2011, growth will have theinto the civilian system has occurred, but theimpact of adding another city thecauses are not related to BRAC. Primarysize of Amarillo or Lubbock tofactors are growth in the population ofSan Antonio.persons eligible for care and growth in thewar related “Warriors in Transition” (WT)who have priority for care within the military system. However, at present over 90% of thecare for the military beneficiary population is provided in military treatment facilities andless than 10% is provided by the civilian TRICARE Provider, Humana Military. BRACrelated changes in military healthcare will benefit both the military and the cooperativemilitary-civilian relationships that exist within the San Antonio health care system. As suchBRAC changes occur, deliberative documentation of the Medical Joint Cross ServicesWorking Group states that change will not result in a reduction in overall clinicalproductivity or capability. A modest reduction in personnel has been planned as “BRACsavings” but this will be off-set by facility enhancements and productivity increases.To understand the findings and conclusions of the report, it is necessary to consider thesystem for providing military health care. America’s Military Health System (MHS) is aunique partnership of medical educators, medical researchers, and healthcare providersand their support personnel worldwide. MHS delivers world-class healthcare to servicemembers, retirees, and their families while maintaining capability to respond withcomprehensive medical capability to military operations; natural disasters and3San Antonio BRAC 2005 Growth Management Plan – Task 6a Report
humanitarian crises around the globe. TheMHS is also a source of innovativeeducation, medical training, research,technology and policy. Two operationalcomponents of the MHS System include:(1) Operational Medicine and MedicalForce Readiness (OM&MFR); and, (2)TRICARE.OM&MFR maintains and projects thecontinuum of healthcare resourcesrequired to provide for the health of theforce. The OM&MFR capability areas are: Medical Force Readiness Programso Medical Readiness Review(MRR) Medical Logistics Theater Trauma Managemento Joint Theater Trauma System (JTTS)o Joint Theater Trauma Registry (JTTR)o Enroute Care Policies and Programso Blast Injury Managemento Traumatic Brain Injury (TBI) Managemento Forward Resuscitative Care Theater Medical Records Deployment Health Follow-upo Post Deployment Health Assessment (PDHA)o Post Deployment Health Re-Assessment (PDHRA) Combat Operational Stress Rehabilitative CareEligible Beneficiaries Federal Strategic Alliance (FEDS-HEAL)(Source: http://fhp.osd.mil)TRICARE is the health care program serving activeduty service members, National Guard and Reservemembers, retirees, their families, survivors and certainformer spouses worldwide. As a major component ofthe Military Health System, TRICARE brings togetherthe health care resources of the uniformed servicesand supplements them with networks of civilian healthcare professionals, institutions, pharmacies andsuppliers to provide access to high-quality health careservices while maintaining the capability to supportmilitary operations. TRICARE offers several healthplan options to meet the needs of the beneficiarypopulation. (Source: http://www.tricare.mil)Approximately 9.2 millionMilitary Facilities Worldwide63 military hospitals413 medical clinics413 dental clinicsSan Antonio EligibleBeneficiariesApproximately 214 thousandSan Antonio Military Facilities2 military hospitals3 medical clinics4San Antonio BRAC 2005 Growth Management Plan – Task 6a Report
Wilford Hall and Brooke Army Medical Center are flagship facilities in Air Force and Armymedicine. Thus, the hospitals play a major role in Operational Medicine, providing care forthe Military Force and serving as both teaching and research hospitals. They also serve asmajor resource centers for provision of care under TRICARE. The BRAC change willconsolidate certain functions of these two hospitals, as shown in Appendix A. However,compared to the existing hospitals, capacity to provide both OM&MFR and TRICAREservices in the joint system will be maintained and service delivery will be enhanced. Threeother factors, all of which must be considered in an analysis of impacts, have occurredsimultaneously: (1) There has been a continual increase in efficiency and productivity; (2)There has been deployment of personnel to support the war effort; and, (3) There hasbeen an increased need to provide care for the Warriors in Transition. The net effect hasbeen a modest transition of patient load to the private sector care providers, with theexpectation that most will go to hospitals which are part of the TRICARE support system.Thus, with regard to the BRAC related displacement of persons to private sector, thestudy conclusions are:1. No additional displacement is anticipated;2. Displacement occurring as a result of other factors is small in comparison to growthin the TRICARE population; and3. The TRICARE System includes provision to accommodate small shifts in patientcare.Information that supports such conclusions follows.Almost all of the patients of the two military hospitals are within the TRICARE populationwhich includes active duty, active duty Family Members, retirees and their FamilyMembers. In 2004, just prior to the 2005 BRAC announcements, the total admissions atBAMC were 15,858 and clinic visits were 645,003. By the end of 2007 that number hadincreased to 18,174 admissions and 791,582 clinic visits. Increases were in all categoriesexcept for Retired/Retired Family members older than sixty five. These numbers fell from5085/126,440 to 4755/120,087. The change in provision of care to this demographic groupis due to the effect of the Global War on Terror (GWOT) and the priority given to Warriorsin Transit (WT) at Military Treatment Facilities.Total admissions at WHMC fell between 2004 and 2007, while clinic visits increased. In2004 admissions were 17,457 and clinic visits were 683,014. In 2007 the patientadmissions had fallen to 15,614 while clinic visits had risen to 734,846. The decrease ininpatient care is explained by deployment of WHMC personnel, especially the critical careprofessionals, to staff Theatre Hospitals in Balad, Iraq and Bagram, Afghanistan.Clinic visits for the combined facilities rose from 1,328,017 to 1,526,428. This increase wasacross all categories except for active duty dependents and those retired over age 65.These two categories fell from 253,321 to 119,415. The decrease in such care was due,again, to priority given to care for the WT. This Medicare eligible population was referred tocivilian facilities accepting TRICARE for Life.By the time BRAC has been fully implemented, demand for care will have increased inmost categories. The incoming BRAC population and other movements into the SanAntonio area are predicted to increase the patient population by about 18,000. BRAC5San Antonio BRAC 2005 Growth Management Plan – Task 6a Report
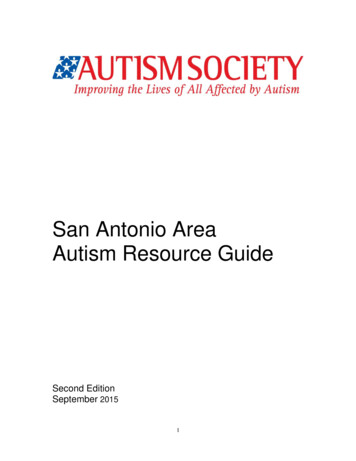
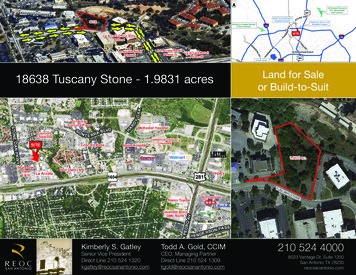
movements are not expected to have an influence on the over-age 65 population. Theover-age 65 population is predicted to slowly grow in concert with general growth andaging of the population. The military health care system will have the capacity to care forthe active duty, active duty Family Members, retiree, and retiree Family Memberpopulations, with care for the over-age-65 population expected to remain at current levels.Should demand in that category increase, care can easily be accomplished in civilianTRICARE support facilities.At the time of BRAC 2005, the total number of TRICARE eligible beneficiaries in the SanAntonio area was reported to be over 210,000. The data on TRICARE eligible personnelsince the 2005 BRAC announcement varies with the source, probably as the result of thegeographic area being surveyed by that source. Based on the numbers from the SAMBIOand the Fort Sam Houston BRAC Transformation Office, the estimate is that the number ofTRICARE eligiblepersons will increaseTable 1: Dispersion of TRICARE in the San Antonio Regionfrom about 214,000 inMilitaryTRICARE2005 to over 230,000 byTotalNetworkTreatmentStandard or2012. Of the knownEligibleProviderFacilityExtra214,000 TRI-CAREeligible beneficiaries in2005214,000114,0569,21990,725the area in 2005, records2008149,056show that 144,056 were2012230,000enrolled to one of theData Source: TRICARE (Date: October 2008)Military TreatmentFacilities, 9,291 wereenrolled to a networkprovider, and the remainder was in TRICARE Standard. These various categories of careare described in Appendix A. At the present time (three years post BRAC) the numberenrolled to the Military Treatment Facilities is now 149,056 (TRICARE office data).Demand for care at both WHMC and BAMC has been significantly increased andinfluenced by ongoing hostilities. Not only have the warriors in transition (WT) returningfrom the theatre demanded complex immediate medical care, they have also requiredongoing and sometimes intensive care for physical and mental disabilities. In addition tofulfilling the mission of providing care to the WT, the staffs of both WHMC and BAMC havedeployed extensively tosupport the hospitals in Iraqand Afghanistan. The impactThe military health care system will havehas been significant in criticalthe capacity to care for the active duty,care; the staff that providesactive duty dependent, retiree, and retireesupports intensive care unitsdependent populations.and the Operating Rooms.Also directly affected havebeen specialties with only a few providers. Loss of any of these few providers createsvacancies which are difficult to fill. While deployments are of limited duration, onespecialist often rotates out as another returns, creating an ongoing specialty shortage.6San Antonio BRAC 2005 Growth Management Plan – Task 6a Report
Where possible, both WHMC and BAMC have hired contract health care providers to fill infor deployed personnel.As mentioned, despite numerousdeployments over the past few years totalhealthcare delivery at military hospitals hasactually increased. Concurrently, there hasbeen an increase in the number of warrelated disabilities and rehabilitation patientswho require continued care.Despite numerous deploymentsover the past few years overallproductivity at military hospitalshas actually increased.In addition to SAMMC, military health care facilities include the clinic at Randolph Air ForceBase, a new Air Force/Veterans Administration military health care clinic on the north sideof town and a new facility at Camp Bullis. These clinics provide primary care and somespecialty services. Two of these clinics are expected to function at the same level of carepost-BRAC, while the Camp Bullis clinic will increase in size, allowing an increasedprimary care enrollment of approximately 7,000 military beneficiaries.At the time of BRAC 2005, while Wilford Hall Medical Center and BAMC were seeing over1.5 million outpatients per year, the clinics at Brooks and Randolph AFB saw an additional20,575 outpatients per year. At the present time, despite reduced resources fromdeployments, the combined outpatient visits and admissions of these facilities for 2007were 1,547,003 outpatients and 33,788 admissions. (SAMBIO Figures)As mentioned above, the number of retirees and their dependents receiving care in thecivilian sector is gradually increasing, as is the number of patients who are over age 65.The reasons for increases in the care provided in the civilian sector are care of thereturning wounded WT and the continued gradual increase in the general beneficiarypopulation. The overflow, reflecting an increase in demand within the non-military systemwill occur throughout the geographical areas in which retired and active duty military live.This will be predominantly inside Loop 1604 and shift further north as future retirees movetoward those areas. Anticipation of this demographic shift has resulted in the recentincrease in medical facilities by several major civilian hospital systems and the VA hospitalsystem with its new Polytrauma Hospital and the Camp Bullis clinic.Based on the current plans for SAMMC North and projected staffing of that facility, closureof WHMC to inpatient care will have little or no effect on civilian hospitals. All plans projecta shift in workload between military facilitiesbut no requirement for civilian hospitals toThe military expects that BRACassume any additional workload other thanchanges will actually improvethat which may come from new TRICAREeligible (usually over 65 TRICARE-for Life)the availability of care in thepatients who have voluntarily elected to seekregioncare in the civilian sector. Projected civilianpopulation growth on the north and west sidesis substantial and will be largely accommodated by the four or five new hospitals and freestanding clinics that are opening in these areas.7San Antonio BRAC 2005 Growth Management Plan – Task 6a Report
Appendix A includes a map with the location of hospitals in the San Antonio metropolitanarea, showing the population within the census districts around each hospital.TRAUMAINTRODUCTIONTrauma is any wound; blunt, such as produced by a fall or physical impact from a vehicularaccident, or penetrating as by a bullet or knife wound. Trauma patients usually requirespecialized care, including surgery and often blood transfusions. It is important for patientsto receive care within the “golden hour” or the first sixty minutes following the trauma. This“golden hour” concept recognizes that many deaths, which could be prevented by timelycare, occur a relatively short time after injury. (Source: http://en.wikipedia.org/wiki/Physical trauma). There are currently three Level I trauma centers in San Antonio. Theseare University Hospital, Wilford Hall Medical Center or WHMC, and Brooke Army MedicalCenter or BAMC. Level I centers are those best able to treat the most serious traumaticinjuries.BRAC involves relocation of WHMC trauma capability into a new San Antonio MilitaryMedical Center at Fort Sam Houston, built around the existing Brooke Army MedicalCenter. Thus, after BRAC, the three Level I trauma centers will have been reduced to two.At the outset of the study there were two potential concerns about such a change. One ofthese was that the availability of trauma care provided by the military might be diminished.This concern has been put to rest. The level of support is expected to be maintained. Asecond potential concern was that there might be a negative impact, due to the longertransit time to a more remote hospital, on seriously injured patients whose injuriesoccurred in the area immediately around WHMC. This concern has also been put to rest.Important factors to consider in analyzing the relationship of BRAC to trauma are: (1) Theproximity of trauma patients to emergency medicine services; (2) The relationship of SanAntonio trauma facilities within the Region; (3) The system for characterizing the severityof trauma and determining which hospitals are equipped to receive patients withincreasingly serious trauma; and (4) The relationships between Military and CivilianTrauma Facilities.Additional considerations include: (1) The actual number of patients with extremely serioustrauma injury that arise within the area near WHMC is very small; (2) There are now plansto increase the number of ambulances and to position them so that service is maintainedin the sector; and (3) Improvements in the landing configuration at SAMMC will reducetimes for air-ambulance transport, more than off-setting any small increase in air-flight timefor helicopter transported patients. These factors together, mitigate or entirely off-set thepotential increase in travel time that might have otherwise been experienced by a postBRAC Level I trauma patient whose injury occurred in proximity to WHMC. However, theplanning team recommends that the planned additions and improvements to the surfaceand air emergency transport systems should be supported.8San Antonio BRAC 2005 Growth Management Plan – Task 6a Report
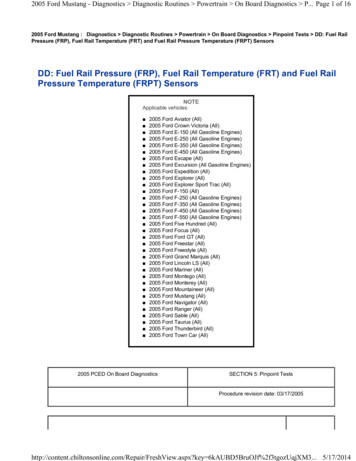
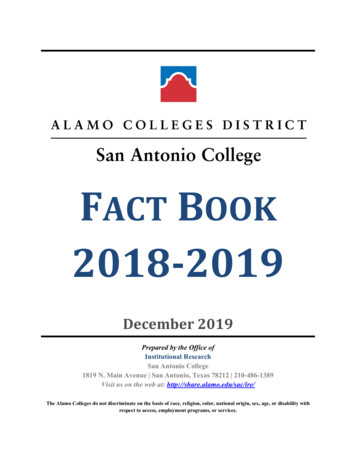
THE RELATIONSHIP OF TRAUMA TO EMERGENCY MEDICINEThe emergency response system is depicted conceptually in the diagram at the right. Asthe bottom of the diagram indicates, there are different levels of care that are related to theseriousness of theFigure 1: Emergency Pyramidpatient’s trauma. Adefinition of the fourlevels is provided in theTrauma and HospitalsSection which follows.When a call comes in, anambulance may bedispatched and there areguidelines which help todetermine where thepatient will be taken.Many complexcircumstances explaindecreases as one movesdown the pyramiddepicted in the figure. Acomplete review of thereasons for the decreaseis not pos
1 san antonio brac 2005 growth management plan task 6a report redistribution of healthcare as a result of the wilford hall medical center (whmc) realignment prepared for city of san antonio office of military affairs by the diluzio group, llc san antonio, tx september 2008