Transcription
Review of Bacteriology &Clinical MicrobiologyProf. Md. Akram HossainApril, 2011
Aetiology of diarrhoea in BangladeshAgentE. coliRotavirusAll ages34.9%23.7 % 5 yrs43.6%37.9%V. Cholerae O1Campylobacter jejuniShigella spp.SalmonellaE. histolytica22.9 %9.5%6.0%2.0%1.2 %12.7%11.0%5.6%1.6%0.3%Giardia lamblia1.6%0.8%CryptosporidiumNo Pathogen0.7%19.6%1.1%17.5%Mixed pathogen31.6%36.0%Prof. Akram, Review Systemic Microbiology2
Bacterial aetiologySlAgentSl.Agent1.2Shigella spp.3.Esch coli(ETEC, EPEC, EHEC.)Salmonella spp.4.Vibrio cholerae5.Campylobacter jejuni6.Yersinia Enterocolitica7.Staphylococcus aureus8.Bacilus cereus9.Clostridum perfringens10.Clostridum difficileProf. Akram, Review Systemic Microbiology3
Viral Etiology of diarrhoeae Sl no.AgentComment1.Rota virusCommonest,Watery, among children2.Norwalk virus3.Calici virus4.Adenovirus5.AstrovirusProf. Akram, Review Systemic Microbiology4
Protozoal aetiology of diarrhoea Sl no.AgentComment1.E. histolyticaInvasive2.Giardia lambliaNon invasive3.CryptosporidiumparvumBalantidium coliImmunosuppressed4.ImmunosuppressedProf. Akram, Review Systemic Microbiology5
Mechanisms involved in diarrhoeaInvasion of GITSalmonella, Shigella, Campylobacter, Escherichiacoli, and Entamoeba histolytica.histolytica.Non invasiveToxin productionVibrio cholerae, ETECDecreased absorptionrotavirus, norwalk agent, giardia lambliaProf. Akram, Review SystemicMicrobiology6
14. Name the causative agents causing14meningitis according to different agegroup. Briefly describe the pathogenesis ofgroupgonorrhoea.Prof. Akram, Review SystemicMicrobiology7
Aetiology of meningitis -1BacteriaStreptococcus Gr.BEsch. ColiListeria monocytogenesH. InfluenzaeS. PneumoniaeN. MeningitidisStaphylococciAge groupNewbornNewbornNewbornChildren 6 monthsYoung adultAdultAdultOther GNBAdultProf. Akram, Review SystemicMicrobiology8
Aetiology of meningitis -2ProtozoaAge groupAcanthamoebaAny ageNaegleria fowleriAdultPlasmodium falciparumAny agefungiCryptococcus neoformansImmunocompromisedVirusAdultPolioAny ageArbovirusesMeningo encephalitisProf. Akram, Review SystemicMicrobiology9
Lab Dx of MeningitisPrinciple: is based on Cytology & biochemical test of CSF(Sugar & Protein), demonstration of the CA from CSF by M/E andculture ( cell culture in case of virus) and also by Ag detection.Steps: Specimen : CSF & Blood M/E : TC & DC of WBC of uncentrifuged & Gram stainedsmear of centrifuged smear. Isolation & identification (Culture): In BA, CA,MA370C aerobically for 24-48 hrs, cell culture for viral infections. Immunological test : Detection of bacterial antigens & Agof C.neoformans from CSF by LAT or other tests. Special tests: CSF sugar & protein, India Ink for C. neoformans.Prof. Akram, Review Systemic Microbiology10
Name the causative agents ofnongonococcal urethritis.urethritis. Write downthe mechanism of action of choleratoxin.toxin15.15Prof. Akram, Review SystemicMicrobiology11
Aetiology of NGU1.2.3.4.5.6.Chlamydia trachomatisMycoplasma hominisMycoplasma genitaliumUreaplasma urealyticumTrichomonas vaginalisCandida albicansProf. Akram, Review SystemicMicrobiology12
Mechanism of action of Cholera toxinCholera toxinBinds with intestinal epithelial cells by B subunitA subunit enters into cells & activates adenyl cyclaseIncreases concentration of cAMP within cellsHypersecretion of water & chlorides and inhibition of reabsorptionof sodium.Intestinal lumen is distended with fluid & there is hypermotilityleading to profuse diarrhea.Prof. Akram, Review SystemicMicrobiology13
1.Enumerate important toxins andenzymes of Streptococcus pyogenes.pyogenes.Give the pathogenesis of Rheumaticfever.feverProf. Akram, Review SystemicMicrobiology14
Toxins of Streptococcus pyogenesStreptolysin ‘O’ –Oxygen labile, hasantigenicity. Destructs RBCs, ASO rises followingantigenicitystreptococcal sore thora but not skin infectionsinfections.Streptolysin ‘S’ – Oxygen stable, Not antigenicantigenic.Pyrogenic toxin (Erythogrnic toxin) A –Present in few strains which are lyosogenic andresponsible for scarlet fever.fever.Pyrogenic toxin (Erythogrnic toxin) B Rapidly destroys tissue and responsible for necrotizingfascitisProf. Akram, Review SystemicMicrobiology15
Enzymes of Streptococcus pyogenes1.2.3.4.Hyaluronidase (Spreading factor)factor)-- Breaksdown proteoglycans of Connective tissuetissue.Streptokinase (Fibrinolysin) – activatesplasminogen to plasmin that breaks fibrin clotclot.DNase (Streptodornase) – depolymerizesDNA in exudates or necrotic tissue.tissue. Antigenic.Antigenic.C5-a peptidase - degrades complement component ofC5a, which attracts phagocytes to the sites of complementdeposition.depositionPrevents chemotaxis of neutrophils andmononuclear phagocytes.phagocytes.Prof. Akram, Review SystemicMicrobiology16
Other Virulence Factors1.2.3.4.Capsule - antiphagocyticFc Binding Protein - antiphagocyticM Protein - antiphagocytic, adhesionPlasmin Binding ProteinProf. Akram, Review SystemicMicrobiology17
Pathogenesis of Acute Rheumatic FeverNonsuppurative inflammatory lesions involving the:HeartJointsSubcutaneous TissuesCentral Nervous SystemUsually follows an upper respiratory infection withGroup A streptococci of certain M proteinserotypes 1, 3, 5, 6, 14, 18, 19, 24Latency 11-5 weeks (Average 19 days)Risk after untreated pharyngitis 3%Prof. Akram,ReviewleadSystemicCutaneous infectionsdo notto ARFMicrobiology18
Pathogenesis of Acute Rheumatic Fever Role of M protein in the pathogenesis isunclear. Two hypothesis:1.2.Due to structural features, M protein elicits theproduction of antibodies cross reactive with hostmyosin, where type II hypersensitivity reaction isresponsible for tissue damage.damage.Due to its superantigenic properties, M proteinstimulates many Th cells thereby releasing largeamount of interleukins and thereby causing tissuedamage.damageProf. Akram, Review SystemicMicrobiology19
2.Classify EnterobacteriaceaeEnterobacteriaceae. Writedown the pathogenesis of Entericfever.feverProf. Akram, Review SystemicMicrobiology20
Classification of EnterobacteriaceaeClinical classificationPrimarily intestinal pathogenPrimarily extraextra-intestinal pathogenBoth intestinal and extraextra-intestinalClassification based on lactose fermentationLactose fermentersLactose non fermentersLate fermentersProf. Akram, Review SystemicMicrobiology21
Clinical classificationPrimarily Intestinal Pathogen1. Shigella 2. Y. enterocoliticaIntestinal & Extraintestinal Pathogen1. Salmonella 2. Esch. coliExtra Intestinal pathogenpathogenKlebsiella 2. Proteus 3.Enterobacter4. Citrobacter 5. Y. pestis etc.1.Prof. Akram, Review SystemicMicrobiology22
Classification based on lactose fermentationLactose fermenters1. Esch coli 2. Klebsiella, 3. Enterobacter4. Citrobacter5. SerratiaLactose non fermenters1. Salmonella 2. Shigella except Sh.sonni 3. ProteusLate lactose ferments –1. Sh.sonni 2. Citrobacter 3.Providencia 4. SerratiaProf. Akram, Review SystemicMicrobiology23
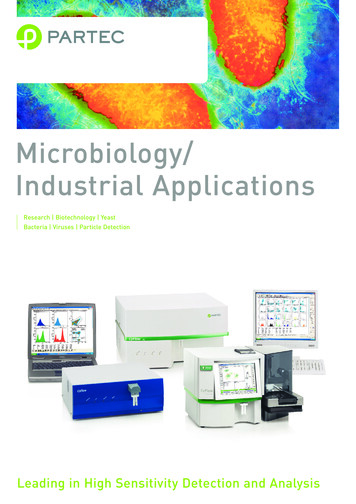
Pathogenesis of enteric feverSalmonella typhi, paratyphi A, B, CSmall intestineAttach, invade epithelial cells & engulfed by MPS where they multiplyReleased into blood via thoracic duct– Primary bacterimia7 -10 daysCleared from blood by MPS and will lodge in liver, spleen, lung, Lymph nodeParasitized cells undergoes necrosis & bacilli heavily reinvade bloodSecondary heavy bacterimiaLocalized to gall bladder, liver, spleen etcClinical illnessOccurs at 14th daysof infectionProf. Akram,Systemic MicrobiologyFrom gallbladder to payers patchesof Reviewintestine-hemorrhage,ulcer24
First time2nd timePathogenesis of typhoid feverProf. Akram, Review Systemic Microbiology25
3. Write down the virulence factors of Neisseriagonorrhoeae with their role in pathogenesispathogenesis. Howcan you diagnose acute gonococcal urethritis inthe laboratory?Prof. Akram, Review SystemicMicrobiology26
Virulence factors of N. gonorrhoeaePilli – the most important virulence factor whichmediate attachment to the mucosal cell surfaceand antiphagocyatic.Ig A proteaseprotease- destroy secretory IgALipooligosaccharide (LOS) of cell wall – likeendotoxinOuter membrane proteins (OMP)–(OMP)–/antigenic variation in pilli and OMPs Prof. Akram, Review SystemicMicrobiology27
What are the virulence factors of N. gonorrhoeae?Virulence factors of N.gonorrhoeaeN.gonorrhoeae-1.Pilli –Adherence to target epithelial cellsResistance to phagocytosis2.Lipooligosaccharides ––3.Outer membrane proteins (OMPs 1&2)––4.OMP 1 - Adherence to target epithelial cellsOMP--2 – porinesOMPIgA1 protease–5.endotoxincleaves IgA1 that defends mucosal surface.Fbp (iron binding protein)Prof. Akram, Review Systemic Microbiology28
Lab diagnosis of gonococcal urethritisPrinciple: Diagnosis of gonococcal urethritis is based onPrinciple:Gram staining and culture of the dischage.dischage.Immunological test are not helpful because of antigenicvariation, NA based tests are usefulStepsSpecimen : Urethral dischargeM/E : Gram Stained smear is very sensitive and specific isadequate for diagnosis in male.male.Culture: Chocolate agar or Thayer –Martin media isCulture:needed to be incubated at 370C for 2424--48 hrs.hrs. Immediate inoculation ofdischarge in media is neededneeded.PCR : of urine samples are widely used as screening test.test.Prof. Akram, Review SystemicMicrobiology29
4.Classify MycobacteriumMycobacterium. Write downthe interpretation of tuberculin testtest.Prof. Akram, Review SystemicMicrobiology30
How can you classify Mycobacteria?1.Mycobacterium tuberculosis complex which can causetuberculosis::tuberculosis1. M. tuberculosis,2.3.4.2.3.M. bovis,bovis,M. africanumafricanum,,M. microti and M. canetti.canetti.M. leprae which causes Hansen's disease or leprosy.leprosy.Nontuberculous mycobacteria (NTM(NTM)) also known asatypical mycobacteria or opportunistic mycobacteriaare all the other mycobacteria which can denitis, skinProf.disease,or disseminated disease.disease.Akram, Review SystemicMicrobiology31
Classification of Mycobacterium .Runyon classification - Ernest Runyon in 1959 classified in 4groupsPhotochromogens, which develop pigments in or after being exposed tolight. M. kansasii,lightkansasii, and M. marinum.marinum.Scotochromogens, which become pigmented (orange to yellow) inScotochromogens,darkness / lightlight. M. scrofulaceumNon-chromogens,Nonchromogens, which includes a group of prevalent opportunisticpathogens called M. avium complex (MAC) M. ulcerans,ulcerans, M. xenopi,xenopi, M.malmoense,, , M. haemophilum and M. genavense.malmoensegenavense.Rapid growers rapidly growing nonnon-chromogenic speciesspecies:: M. chelonae,chelonae, M.abscessus,, M. fortuitumabscessusNo. of NTM rises from about 50 in 1997 to over 125 by JanuaryNo.2007Prof. Akram, Review SystemicMicrobiology32
Mantoux test100 years old test.test. Used to see whether aperson is exposed to M.tuberculosis naturally orartificially . It does not indicate a person issuffering from disease or immune to disease.disease.5 TU PPD is injected into upper skin layerof the patient's arm.arm.The arm is examined 48 to 72 hoursAny swelling that can be felt around the siteof the injection, also known as induration, ismeasuredInterpretation-InterpretationPositive - 10 mmmm- due to disease, or BCGNegative - 10 mm – No exposureFalse positive – Positive without disease dueto atyptical mycobacteriaFalse negativenegative- Negative with disease e.g.Milliary TB, Immunosuppressiondue toProf. Akram, Review SystemicAIDS, cytotoxic drugs etcetc. Microbiology33
Lab Diagnosis of TuberculosisPrinciple:Lab diagnosis of TB is based on demonstration of AFBby microscopy (LM & FM), isolation by culture,culture,Immunological tests ( Ab & Cell mediated), Nucleidacid based techniques (PCR & Probes)Probes).Prof. Akram, Review SystemicMicrobiology34
Lab diagnosis of TB MicroscopyMicroscopy - Microscopy is the easiest and most rapiddiagnostic procedure that detect the acid fast bacilli in clinicalspecimen.specimenIt is less sensitive than culture and requires high bacillary load5,000 to 1010,,000000/ml/ml.its sensitivity varies from 3030%% to 7070%%. Its sensitivity can beincreased up to 74 – 7878%% when centrifuged concentrateddeposited are usedThree type of staining are used (i) ZiehlZiehl-Neelsen stain (ii)(ii)Fluorochrome stain and (iii) Kinyoun stainProf. Akram, Review SystemicMicrobiology35
Lab diagnosis of TB Cultureculture provides the definitive diagnosis of tuberculosisdefending on the decontamination method and the type ofculture medium used, as few as 10 to 100 viable tuberclebacilli/ml of sample can be detected.detected.EGG-BASED MEDIA -Dorset media (1903EGG1903),), LowensteinLowenstein-Jensin media (1930),1930), Ogawa media (1949)1949)AGAR BASED MEDIUM -Middlebrook 7H – 10 , 7H – 11INCUBATION - at 350 to 370C until growth is observed ordiscarded as negative after 8 weeks.weeks.LIQUID MEDIA – Dubos media, Sula media – 10 daysrequired for growth.MGIT – Mycobactyerial growth indicator tubeRADIOMETRIC METHODBACKTEC 460 TB MethodProf. Akram, Review SystemicMicrobiology36(Beckton Dickinson) 55- 7 days
Lab diagnosis of TB ImmunologicalBoth T Cell based and antibody based immunologicaltests are availableT cell based TUBERCULIN SKIN TEST(1) Mantoux test and(2) Heaf test.Quantiferon--TBQuantiferonAntibody based –ENZYME LINKED IMMUNOSORBENT ASSAY (ELISA) –38 kDa protein, Antigen AA-60,IMMUNOCHROMATOGRAPHY (ICT)Prof. Akram, Review SystemicMicrobiology37
Ques:: How you will you proceed to diagnose a case of pulmonaryQuestuberculosis ?Ans::AnsPrinciple :Diagnosis of PTB is based on demonstration of the AFB by Z-N& Fluorescent stained smear, then isolation & identification of byculture, and detection of Antibody or DTHby immunological tests.tests.detection of genes by NA based techniques are also used.used.Steps::StepsSpecim
Prof. Akram, Review Systemic Microbiology. Lab diagnosis of TB Culture cultureculture provides provides thethe definitivedefinitive diagnosisdiagnosis ooff tuberculosistuberculosis defendingdefending oonn the the decontaminationdecontamination methodmethod andand thethe typetype ooff cultureculture medium medium used,used, aass few few aas 1100 ttoo 100100 viableviable tubercle tubercle .File Size: 1MBPage Count: 128