Transcription
POLICY STATEMENTOrganizational Principles to Guide and Define the Child HealthCare System and/or Improve the Health of all ChildrenRecommended Terminology forSubstance Use Disorders in the Careof Children, Adolescents, YoungAdults, and FamiliesRachel H. Alinsky, MD, MPH, FAAP,a Scott E. Hadland, MD, MPH, MS, FAAP,b Joanna Quigley, MD, FAAP,cStephen W. Patrick, MD, MPH, MS, FAAP,d COMMITTEE ON SUBSTANCE USE AND PREVENTIONPediatricians across the United States encounter infants, children,adolescents, young adults, and families affected by substance usedisorders in their daily practice. For much of history, substance usehas been viewed as a moral failing for which individuals themselves areto blame; however, as addiction became understood as a medicaldisorder, clinical terminology has shifted along with a growingawareness of harm of stigmatizing language in medicine. In issuingthis policy statement, the American Academy of Pediatrics (AAP) joinsother large organizations in providing recommendations regardingmedically accurate, person-first, and nonstigmatizing terminology.As the first pediatric society to offer guidance on preferred languageregarding substance use to be used among pediatricians, media,policymakers, and government agencies and in its own peer-reviewedpublications, the AAP aims to promote child health by highlightingthe specific context of infants, children, adolescents, young adults, andfamilies. In this policy statement, the AAP provides 3 specificrecommendations, accompanied by a table that presents a summaryof problematic language to be avoided, paired with the recommendedmore appropriate language and explanations for each. Pediatricianshave an important role in advocating for the health of childrenand adolescents in the context of families affected by substanceuse and are optimally empowered to do so by avoiding the use ofstigmatizing language in favor of medically accurate terminologythat respects the dignity and personhood of individuals withsubstance use disorders and the children and adolescentsraised in families affected by substance use.PEDIATRICS Volume 149, number 6, June 2022:e2022057529Downloaded from /149/6/e2022057529/1327806/peds 2022057529.pdfby Health Services Research Library userabstractaDivision of Adolescent and Young Adult Medicine, Johns HopkinsSchool of Medicine, Baltimore, Maryland; bDivision of Adolescent andYoung Adult Medicine, Mass General Hospital for Children, Boston,Massachusetts; cDepartment of Psychiatry, University of Michigan, AnnArbor, Michigan; and dDepartments of Pediatrics and Health Policy,Vanderbilt Center for Child Health Policy, Vanderbilt University MedicalCenter, Nashville, TennesseeDr Alinsky conducted an extensive literature review, contributed tothe development of the final recommendations, wrote the first draftof the manuscript, reviewed and revised the manuscript, andedited the final manuscript; Drs Hadland, Patrick, and Quigleycontributed to the development of the final recommendations,reviewed and revised the manuscript, and edited the finalmanuscript; and all authors approved the final manuscript assubmitted and agree to be accountable for all aspects of the work.This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its board of directors. All authors havefiled conflict of interest statements with the American Academy ofPediatrics. Any conflicts have been resolved through a processapproved by the board of directors. The American Academy ofPediatrics has neither solicited nor accepted any commercialinvolvement in the development of the content of this publication.The guidance in this report does not indicate an exclusive courseof treatment or serve as a standard of medical care. Variations,taking into account individual circumstances, may be appropriate.All policy statements from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.Address correspondence to Rachel H. Alinsky, MD, MPH. E-mail:Ralinsk1@jhmi.eduTo cite: Alinsky RH, Hadland SE, Quigley J, et al ; AAPCOMMITTEE ON SUBSTANCE USE AND PREVENTION.Recommended Terminology for Substance Use Disorders inthe Care of Children, Adolescents, Young Adults, and Families.Pediatrics. 2022;149(6):e2022057529FROM THE AMERICAN ACADEMY OF PEDIATRICS
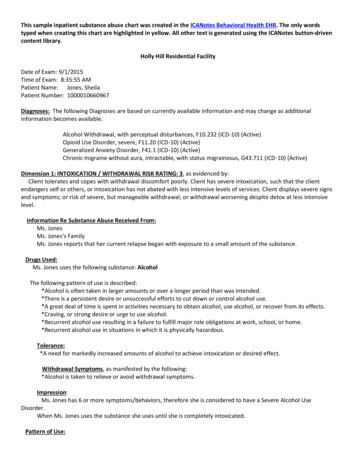
Pediatricians across the UnitedStates encounter infants, children,adolescents, and families affected bysubstance use disorders (SUDs) intheir daily practice. Amid thenational overdose crisis, the rise ofwidespread cannabis and e-cigaretteavailability, and persistently highprevalence of alcohol use, there is arenewed focus on recognition andtreatment of SUDs. In previouspolicy statements, the AmericanAcademy of Pediatrics (AAP)1recognized the unique role ofpediatricians in identifying andresponding to familial substance useand has highlighted the importanceof doing so in an empathetic,respectful, and supportive manner.Fundamental to this practice is anappreciation of the impact of language itself, with particular carepaid to the terminology used ininteractions with patients, family,and the public and in writtenmaterials.A substantial hurdle tocompassionately caring for patientsand families affected by substanceuse is the widespread stigma againstpeople with SUDs. For much ofhistory, substance use has beenviewed as a moral failing for whichindividuals themselves are to blame,particularly individuals of color.2–6Stigmatizing language reflecting thisimplicit bias and moralistic view,such as “substance abuse,” “drugabuser,” and “addict,” have beencommonplace not only in generalconversation and the lay press7 butalso in medical literature.8 Many ofthese pejorative terms have racistconnotations, and derogatory termslike “crack babies” carry with themdecades of legislation targetingcommunities of color with a carceralresponse to substance use, such asthe War on Drugs.5,6 In the face ofthe increasing prevalence of the useof opioids, marijuana, and novelpsychoactive substances, themedical community has recognizeda great deal of scientific evidencerevealing that addiction is a chronicillness that has the potential forrecurrence similar to other medicalconditions and is not a moralfailing.9As addiction became understood asa medical disorder, clinicalterminology shifted, including thatin the Diagnostic and StatisticalManual of Mental Disorders (DSM).Previous versions of the DSM usedthe phrase “substance abuse”;10however, the DSM-5 uses the lessstigmatizing term “substance usedisorder,” recognizing the chronicdisease nature of addiction.11 Thisshift in DSM nomenclature alignedwith a growing awareness of thepower of stigmatizing language inmedicine. The use of derogatoryterms such as “substance abuse” and“substance abuser” has been shownto negatively affect both laycommunity members’ and healthcare providers’ perceptions ofindividuals who usesubstances,3,12–17 resulting in theview that these individuals needpunishment as opposed to help ortreatment. These internalizedperceptions have tangible effects, asevidenced by a systematic reviewthat found that health careproviders’ negatively biased viewsof individuals with SUDs result inworse health care delivery.18 International Society for Addiction Journal Editors25,26 The White House27 National Institutes of Health28 Associated Press29 Columbia Journalism Review30 National Academies of Science,Engineering, and Medicine4,31THE PEDIATRIC CONTEXTAs the first pediatric society to offerguidance on preferred languageregarding substance use to be usedamong pediatricians, media,policymakers, government agencies,and in its own peer-reviewedpublications, the AAP aims topromote child health by highlightingthe specific context of children,adolescents, and families.Pediatricians have an essential rolein the prevention of, treatment of,and advocating for infants, children,adolescents, and young adultsaffected by substance use. They areempowered to do so by activelyworking to dismiss harmfulstereotypes and avoiding the use ofstigmatizing language in favor ofmedically accurate terminology thatrespects the dignity and personhoodof individuals with substance usedisorders and the children andadolescents raised in familiesaffected by substance use.In response to this evidence, the USgovernment, as well as majorscientific and journalismorganizations, continue to issuestatements guiding the use ofappropriate language in thediscussion of substance use andSUDs, including:Table 1 presents a summary ofproblematic language to be avoided,paired with the recommended moreappropriate language and anexplanation. The table is organizedinto 3 main topics. The first topicpertains to terminology regardingsubstance use, specifically coveringthe medically accurate diagnosticterminology for substance usedisorders. The American Society of Addiction Medicine19–21 Association for MultidisciplinaryEducation and Research in Substance Use and Addiction22,23 American Medical Association24The second topic in the table relatesto the use of “person-first” languagethat first and foremostacknowledges the innatepersonhood of an individual, ratherthan defining someone primarily on2Downloaded from /149/6/e2022057529/1327806/peds 2022057529.pdfby Health Services Research Library userFROM THE AMERICAN ACADEMY OF PEDIATRICS
TABLE 1 Recommended Terminology Regarding Substance UseSay This:Not This:Terminology regarding substance useSubstance use disorder; [insertDrug abuse/dependencespecific substance: opioid,Substance abuse/dependencecocaine, alcohol, etc] use disorderAddictionSubstance useHazardous substance useUnhealthy substance useProblematic substance useSubstance abuseDrug habitViceHere’s Why:The diagnostic terms “substance abuse” and “substancedependence” described in the DSM-IV have been combinedin the DSM-5 into “substance use disorder.” “Abuse” and“dependence” should only be used in specific reference toDSM-IV or earlier criteria or when using ICD-10nomenclature, which still use the term “dependence;”“addiction” may also be used in conjunction with a severesubstance use disorder.Substance use exists on a continuum, not all of whichconstitutes a diagnosable substance use disorder;therefore, these terms describe substance use that riskshealth consequences or is in excess of current safe useguidelines, without necessarily referencing or meetingcriteria for a substance use disorder; it is more precisein describing health hazard than simply “misuse.” Of note,any substance use in adolescents is considered unhealthy.Nonmedical prescription opioid use Prescription opioid abuseNonmedical prescription drug use Prescription drug abuseNonmedical prescriptionmedication useRefers to using opioids or other prescription drugs in a wayother than as prescribed or by a person to whom theywere not prescribed.Intoxicated or in withdrawalStrung out, tweaking, high, drunk (and othercolloquial substance-specific terms)Uses medically accurate language to describe the state ofintoxication or withdrawal from a substance.UsingGetting highLess stigmatizing way to describe the act of using asubstance to reach intoxication.DrinkingGetting drunkTerminology regarding personsPerson with a substance usedisorderPerson who uses [insert specificsubstance: opioid, cocaine,alcohol, etc]Person who injects drugs (PWID)Uses person-first language, as individuals are not definedSubstance/drug abuser, addict, junkie,solely by their substance use. If unsure of whether thedruggie, stoner, alcoholic, drunk (and otherindividual has a diagnosed disorder, then the descriptioncolloquial substance-specific terms)of “a person who uses [insert specific substance]” isDrug user, heroin user, drinker, crackhead,most appropriate.pothead, drug-seeking (and other colloquialsubstance-specific terms)Injection drug userTreatment was not effectivePatient in need of more support/higher level of treatmentPatient who failed treatmentNoncompliant, nonadherentReferring to the treatment not meeting the needs of thepatient or the patient needing a higher level of treatment,rather than the patient failing.Person with multiple recurrencesPerson with multiple treatmentadmissionsFrequent flyerRecidivistLess stigmatizing way to denote someone with recurrence ofsubstance use disorder, rather than referencing it as acriminal offense or a relapse, which is associated withthe connotation of more blame.Infant/baby with neonatalwithdrawal syndromeInfant/baby born substanceexposedInfant/baby with physiologicdependence/withdrawalAddicted babyBorn addictedDrug endangeredNeonatal abstinence syndrome baby or NASbabyCrack babySubstance use disorders, characterized by repeated usedespite harmful consequences, cannot be diagnosed in aninfant; an infant can develop physiologic dependence to asubstance such as opioids, for which the medical term isneonatal opioid withdrawal syndrome or neonatalwithdrawal.Concerned loved oneEnablerLess stigmatizing way to describe a loved one who supportssomeone with a substance use disorder and at times mayprotect them from the negative consequences of theirsubstance use.Terminology regarding treatmentTreatment, pharmacotherapyMedication-assisted treatment (MAT)Medication for addiction treatment Opioid substitution therapy(MAT)Opioid replacement therapyMedication for opioid use disorder(MOUD)PEDIATRICS Volume 149, number 6, June 2022Downloaded from /149/6/e2022057529/1327806/peds 2022057529.pdfby Health Services Research Library userMedication is treatment and should not be referenced as“assisting” some other treatment, or as simplysubstituting one opioid for another; if use of acronym“MAT” is desired, recommend using it to refer to term“medication for addiction treatment.”3
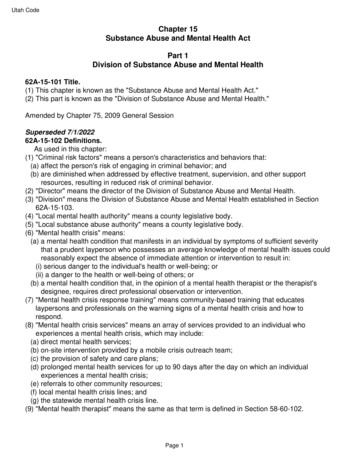
TABLE 1 ContinuedSay This:In early remissionIn sustained remissionIn recoveryEntered recoveryStopped using substancesEngaged in treatmentNot This:CleanGot cleanHere’s Why:People with a history of substance use who are notcurrently using are deemed “in remission” or “inrecovery,” more neutral words than “clean” which impliesthat people actively using substances are “dirty.”Negative versus positive test result Clean versus dirty test/urine[Insert substance] detectedRefer to the actual results of the toxicology test, rather than“clean” and “dirty,” which imply judgment.ICD-10, International Classification of Diseases and Related Health Problems, 10th Edition.the basis of a condition orcharacteristic (in this case,substance use). The use of personfirst (or people-first) language isconsistent with the standard set inprevious AAP policy statements fordescribing individuals with otherchronic medical conditions ordisabilities, such as “a child withdiabetes” rather than “a diabetic.”32A special circumstance to highlightin this section is the problematiclanguage that has been used todescribe infants born substanceexposed who, in the lay press andelsewhere, have commonly andinappropriately been referred to as“born addicted.” This language andthe associated intense stigmasurrounding SUDs in pregnantindividuals can dissuade them fromseeking treatment or cause them toabruptly end treatment, leading toworse outcomes for infants andfamilies. The medically accurateterminology for infants who havewithdrawal after birth is neonatalwithdrawal.33,34 This is in contrastto a substance use disorder, which,by definition, includes “aproblematic pattern of substanceuse leading to clinically significantimpairment or distress, as manifestby at least two [ maladaptivebehaviors].”11 On the basis of thismedical definition, infantsunequivocally cannot display thebehavioral patterns necessary to be“addicted” to drugs, and the use ofthis terminology is highlystigmatizing to families.The last topic in the table coversterminology for use in thediscussion of the treatment of SUDs.Medication for opioid use disorderhas been demonstrated to be safeand effective31,35 and is recognizedby the AAP, the Society forAdolescent Health and Medicine, theAmerican Society of AddictionMedicine, and the American Collegeof Obstetricians and Gynecologistsas the recommended treatment fornot only adults but also adolescentsand pregnant people with an opioiduse disorder.36–40 For this reason, itis most accurate to refer tomedication as treatment in and ofitself, as opposed to “assisting”other treatment or being used as a“substitution” or “replacement”therapy. As of 2022, there are nodata to suggest that the termnicotine replacement therapy isassociated with stigma or that thisterminology dissuades individualsfrom seeking medication treatmentfor nicotine use disorder; futurestudies could examine thisquestion.At times, patients may use some ofthese problematic terms to describetheir own experiences. Whileallowing patients to choose theirown language out of respect fortheir lived experience, pediatriciansthemselves should, nonetheless,continue to use the preferredterminology, because modelingaccurate terminology remainsvaluable even in thesecircumstances so as not to4Downloaded from /149/6/e2022057529/1327806/peds 2022057529.pdfby Health Services Research Library userperpetuate the intense shameoften associated with SUDs.Pediatricians can also use theseopportunities as a catalyst forconversations with patients andparents about reducing stigma andwhy using nonstigmatizing languagematters.Lastly, individuals will undoubtedlyencounter problematic terms in theexisting literature and even in theInternational Classification ofDiseases and Related HealthProblems, 10th Edition;41 whenreferencing or summarizing thisliterature, it is recommended toreplace the problematic terms withthe preferred terminology. If anexact citation is necessary, one canuse quotations and the notation“[sic],” accompanied by anexplanation of the outdatedproblematic terminology.RecommendationsThe AAP recommends the following:1. Pediatricians, policymakers,government agencies, and mediashould use medically accurateterminology as opposed tostigmatizing jargon (see Table 1)in interactions with patients,families, and the public as well asin written materials includingmedical record documentation,correspondence, manuscripts,editorials and opinion articles,and news stories.2. Pediatricians, health care facilityspokespersons, policymakers,FROM THE AMERICAN ACADEMY OF PEDIATRICS
government agencies, and mediashould use person-first languagethat respects the dignity of anindividual first and foremost as aperson (see Table 1) in interactionswith patients, families, and thepublic, as well as in writtenmaterials, including medical recorddocumentation, correspondence,manuscripts, editorials and opinionarticles, and news stories.3. Professional entities shouldencourage authors submittingmanuscripts or materials forpublication in their journals to usemedically accurate and respectfulperson-first language (see Table 1).Lead AuthorsRachel H. Alinsky, MD, MPH, FAAPScott E. Hadland, MD, MPH, MS,FAAPJoanna Quigley, MD, FAAPStephen W. Patrick, MD, MPH, MS,FAAPCommittee on Substance Use andPrevention, 2020–2021Lucien Gonzalez, MD, MS, FAAP,ChairpersonDeepa R. Camenga, MD, MHS, FAAPStacey Engster, MD, MS, FAAPStephen W. Patrick, MD, MPH, MS,FAAPJoanna Quigley, MD, FAAPLeslie Walker-Harding, MD, FAAPLiaisonsJennifer A. Ross, MD, MPH, FAAP –Section on Pediatric TraineesRebecca Ba’Gah, MD, FAAP –American Academy of Child andAdolescent PsychiatryStaffRenee Jarrett, MPHDOI: https://doi.org/10.1542/peds.2022-057529PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).Copyright 2022 by the American Academy of PediatricsCONFLICT OF INTEREST DISCLOSURES: The authors have indicated they have no potential conflicts of interest to disclose.REFERENCES1. Smith VC, Wilson CR; Committee on Substance Use and Prevention. Familiesaffected by parental substance use.Pediatrics. 2016;138(2):e201615752. Botticelli MP, Koh HK. Changing the language of addiction. JAMA. 2016;316(13):1361–13623. Kelly JF, Westerhoff CM. Does it matterhow we refer to individuals with substance-related conditions? A randomizedstudy of two commonly used terms. Int JDrug Policy. 2010;21(3):202–2074. National Academies of Sciences Engineering and Medicine. Ending Discrimination Against People with Mental andSubstance Use Disorders: The Evidencefor Stigma Change. Washington, DC:National Academies Press; 20165. Netherland J, Hansen HB. The war ondrugs that wasn’t: wasted whiteness,“dirty doctors,” and race in media coverage of prescription opioid misuse. CultMed Psychiatry. 2016;40(4):664–686language in news media coverage ofthe opioid epidemic: implications forpublic health. Prev Med.2019;124:110–114isn’t good enough. Alcohol Treat Q.2019;37(2):257–2728. Bailey NA, Diaz-Barbosa M. Effect ofmaternal substance abuse on the fetus,neonate, and child. Pediatr Rev.2018;39(11):550–55914. Ashford RD, Brown AM, McDaniel J,Curtis B. Biased labels: an experimentalstudy of language and stigma amongindividuals in recovery and health professionals. Subst Use Misuse.2019;54(8):1376–13849. U.S. Department of Health and HumanServices, Office of the Surgeon General.Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs,and Health. Washington, DC: CreateSpaceIndependent Publishing Platform; 201715. Barry CL, McGinty EE, Pescosolido, BA,Goldman HH. Stigma, discrimination,treatment effectiveness and policy: public views about drug addiction andmental illness. Psychiatr Serv.2014;65(10):1269–127210. American Psychiatric Association. Diagnostic and Statistical Manual of MentalDisorders. 4th ed. Washington, DC:American Psychiatric Association; 199416. Kelly JF, Dow SJ, Westerhoff C. Does ourchoice of substance-related terms influence perceptions of treatment need?An empirical investigation with twocommonly used terms. J Drug Issues.2010;40(4):805–81811. American Psychiatric Association.Diagnostic and Statistical Manual ofMental Disorders. 5th ed. Arlington, VA:American Psychiatric Association; 20136. James K, Jordan A. The opioid crisis inBlack communities. J Law Med Ethics.2018;46(2):404–42112. Ashford RD, Brown AM, Curtis B. Substance use, recovery, and linguistics:the impact of word choice on explicitand implicit bias. Drug Alcohol Depend.2018;189:131–1387. McGinty EE, Stone EM, KennedyHendricks A, Barry CL. Stigmatizing13. Ashford RD, Brown AM, Curtis B.“Abusing addiction”: our language stillPEDIATRICS Volume 149, number 6, June 2022Downloaded from /149/6/e2022057529/1327806/peds 2022057529.pdfby Health Services Research Library user17. McGinty EE, Goldman HH, Pescosolido B,Barry CL. Portraying mental illness anddrug addiction as treatable health conditions: effects of a randomized experiment on stigma and discrimination.Soc Sci Med. 2015;126:73–8518. van Boekel LC, Brouwers EPM, van Weeghel J, Garretsen HFL. Stigma amonghealth professionals towards patientswith substance use disorders and its5
consequences for healthcare delivery:systematic review. Drug AlcoholDepend. 2013;131(1-2):23–3519. American Society of Addiction Medicine.Terminology related to addiction, treatment, and recovery. Available ddiction-treatment-and-recovery.Accessed November 11, 202120. American Society of Addiction Medicine.Terminology related to the spectrum ofunhealthy substance use. Available thespectrum-of-unhealthy-substance-use.Accessed November 11, 202121. American Society of Addiction Medicine.Language and terminology guidance forJournal of Addiction Medicine (JAM)manuscripts. Available at: terminologyguidance.Accessed November 11, 202122. Association for Multidiscplinary Education and Research in Substance Useand Addiction. Interdisciplinary addiction strategies: discover, prevent, treat,teach. In: Program of the AMERSA 42ndAnnual National Conference; November8–10, 2018; San Francisco, CA.23. Broyles LM, Binswanger IA, Jenkins JA,et al. Confronting inadvertent stigmaand pejorative language in addictionscholarship: a recognition andresponse. Subst Abus. 2014;35(3):217–22124. American Medical Association. Language matters to the AmericanMedical Association. Available loads/2020/07/Language-Matters Template-1.pdf. Accessed June 30, 202133. Hudak ML, Tan RC; Committee on Drugs;Committee on Fetus and Newborn;American Academy of Pediatrics. Neonatal drug withdrawal. Pediatrics.2012;129(2):e540–e56025. Saitz R. International statement recommending against the use of terminologythat can stigmatize people. J AddictMed. 2016;10(1):1–234. Patrick SW, Barfield WD, Poindexter BB;Committee on Fetus and Newborn, Committee on Substance Use and Prevention.Neonatal opioid withdrawal syndrome.Pediatrics. 2020;146(5):e202002907426. Stenius K, Nesvåg S. ISAJE terminologystatement. Nordic Stud Alcohol Drugs.2015;32(5):539–54027. Botticelli M. The White House. Changingthe language of addiction. Available 01/13/changing-languageaddiction. Accessed November 11, 202128. National Institute on Drug Abuse. Wordsmatter: terms to use and avoid whentalking about addiction. Available ult/files/nidamedwordsmatter3 508.pdf. AccessedNovember 11, 202129. The Associated Press. The AssociatedPress Stylebook 2017 and Briefing onMedia Law. 52nd ed. New York, NY:Basic Books; 201730. Feder KA, Krawczyk N. Columbia Journalism Review. Four facts every journalist should know when covering theopioid epidemic. Columbia JournalismReview. Published online August 15,2017 Available at: https://www.cjr.org/united states project/opioid-journalistadvice.php. Accessed October 17, 202031. National Academies of Sciences Engineering and Medicine. Medications forOpioid Use Disorder Save Lives.Washington, DC: National AcademiesPress; 201932. Pont SJ, Puhl R, Cook SR, Slusser W;Section on Obesity; Obesity Society.Stigma experienced by children andadolescents with obesity. Pediatrics.2017;140(6):e201730346Downloaded from /149/6/e2022057529/1327806/peds 2022057529.pdfby Health Services Research Library user35. Murthy VH. Surgeon General’s report onalcohol, drugs, and health. JAMA.2017;317(2):133–13436. Committee on Substance Use and Prevention. Medication-assisted treatment ofadolescents with opioid use disorders.Pediatrics. 2016;138(3):e2016189337. American College of Obstetricians andGynecologists. Opioid use and opioiduse disorder in pregnancy. Obstet Gynecol. 2017;130(2):e81–e9438. American Society of Addiction Medicine.National practice guideline for the treatment of opioid use disorder. Available 20-national-practice-guideline.Accessed November 11, 202139. Patrick SW, Schiff DM; Committee onSubstance Use and Prevention. A publichealth response to opioid use in pregnancy. Pediatrics. 2017;139(3):e2016407040. Society for Adolescent Health and Medicine. Medication for adolescents andyoung adults with opioid use disorder.J Adolesc Health. 2021;68(3):632–63641. World Health Organization. The ICD-10classification of mental and behaviouraldisorders: clinical descriptions and diagnostic guidelines. F10-F19: mental andbehavioral disorders due to psychoactivesubstance use. Available at: https://www.who.int/substance abuse/terminology/ICD10ClinicalDiagnosis.pdf. AccessedNovember 11, 2021FROM THE AMERICAN ACADEMY OF PEDIATRICS
POLICY STATEMENT Organizational Principles to Guide and Define the Child Health Care System and/or Improve the Health of all Children Recommended Terminology for Substance Use Disorders in the Care of Children, Adolescents, Young Adults, and Families Rachel H. Alinsky, MD, MPH, FAAP,a Scott E. Hadland, MD, MPH, MS, FAAP,b Joanna Quigley, MD, FAAP,c