Transcription
Feeding Clinic: A MultidisciplinaryApproach to Pediatric Feeding DisordersBrenda Sitzmann, MA, CCC-SLPSarah Edwards, DOLaura Slosky, PhDJamie Wilkins, RD, LD, CNSCElizabeth Schroeder, OTR/L The Children's Mercy Hospital, 2017
Feeding Services at Children’s Mercy2 The Children's Mercy Hospital, 2014. 03/14
Feeding Servicesat Children’s MercyInterdisciplinary Pediatric Feeding &Swallowing Program Multidisciplinary Feeding Clinic at Adele Hall Focus of today’s presentation GI, psychology, nutrition, speech and OT Multidisciplinary Feeding Clinic at CMK GI NP, pediatrician, psychology, nutrition, OT Similar to MDFC but no SLP services3 The Children's Mercy Hospital, 2014. 03/14
Multidisciplinary Feeding Clinic (MDFC) Adele Hall Team Members Gastroenterologist: Sarah Edwards, DO Psychology: Laura Slosky, PhD Nutrition: Jamie Wilkins, RD, LD, CNSC & April Escobar, MS,RD, CSP, LD Speech: Brenda Sitzmann, MA, CCC-SLP, CLC OT: Elizabeth Schroeder, MOT, OTR/L & Rebecca Pearson, MOT,OTR/L Social work is available as needed4
Patient Population Birth to 18 years of age Oral feeders or potential to be oral feeders Children with g-tubes who are unableto be oral feeders are followed by gtube clinic Benefit from at least 3 of the 5 disciplines5
Feeding Disorders Pediatric Feeding Disorders are Common– 25% of children 3-10% of children have severefeeding problems– 80% in developmentally delayedpopulation Feeding difficulties are often multifactorial Combination of medical, psychosocial,nutrition and skills/ability factorsManikam R and Perman JA. Pediatric Feeding Disorders. Journal of Clinical Gastroenterology. 2000. 30;1, 34-46.6
Common Diagnoses/Reason for Referrals Oral aversion EoE Aspiration Sensory concerns Extremely selective eaters Reflux Limited oral intake Constipation Vomiting/feedingintolerance Difficulty gaining weight Non-oral feedings Behaviors are impactingoral intake Using liquids to meetnutritional needs Weaning from g-tube feedings7
Typical Team Visit Family completes a packet before they are scheduled Birth history, medical history, development, currentmedications, current therapy services, food log 1 1/2 to 2 hour visit Height and weight Caregiver interview with the entire team Feeding assessment May use the observation window8
Typical Team Visit Physical exam Team meeting Team leaves the exam room to formulate a plan Recommendations Personalized written recommendations/homeprogram “Depart Summary”9
GastroenterologySarah Edwards, DO10
History Illness Prematurity Development and acquisition of oral motorskills11
History Medications Bowel Habits Detailed diet andfeeding history12
Feeding History Choking or Gagging Changes in respiration Regurgitation or VomitingCohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92.13
Reflux or Vomiting? Is it reflux or vomiting– Reflux is the EFFORTLESS return of gastric contentsinto the esophagus and/or out of the mouth– Vomiting is the forceful return of gastric contents outof the mouth, often accompanied by nausea andretching14
Feeding History Feeding refusal Meal duration Current Diet, texturesCohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92.15
Feeding History Stage at which choking/gagging,regurgitation occurs is important Later in feeding: greater correlation withmedical issuesCohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92.16
Feeding History Problems early in feeding: may relate to positioning parent-child interaction oral defensivenessCohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92.17
Feeding History Meal duration beyond 30 min– Healthy child: behavioral feeding problem– Medical disorder: ineffective mechanicsCohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92.18
Physical Exam Assessment of Growth Abdomen for constipation Spine for kyphoscoliosis, sacral anomaliesCohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92.19
Physical Exam Neurologic for tone and level of function Oral for gag, swallow, seal, drooling,mucosal problemsCohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92.20
Physical ExamSigns of deficiency or chronicillnesshttp://en.wikipedia.org/wiki/Nail clubbingCohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92.21
Assessing Growth Account for prematurity– Correct until age 2 years Adequate growth is themost important goal.22
Oral Motor Competency23
Oral Motor CompetencyMcSweeney ME, Kerr J, Amirault J, et al. Oral Feeding Reduces Hospitalizations Compared with Gastrostomy Feeding in Infants and Children24who Aspirate. The Journal of Pediatrics. 2016;170:79-84.
Further Investigation Labs Imaging Procedures25
Laboratory CBC Electrolytes Vitamin and Mineral levels Metabolic26
Imaging Bone age MRI of the head Upper GI x-ray27
Imaging Videofluoroscopic SwallowStudy Gastric emptying study28
Procedures pH study with impedance Esophagogastroduodenoscopy (EGD) Fiberoptic Endoscopic Evaluation ofSwallowing (FEES)29
30
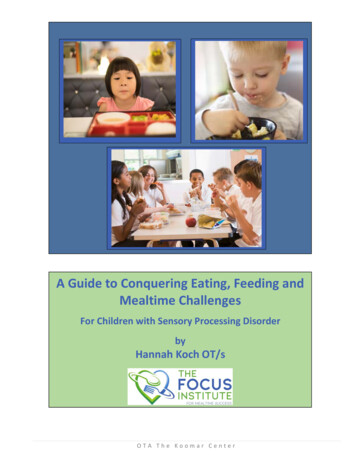
Findings 86% medical disorder 61% oropharyngeal dysfunction 18.1% behavioral problemConditions occurred both alone and in combination.31
Findings32
33 The Children's Mercy Hospital, 2014. 03/14
Findings: Medical Conditions Prematurity significant risk factor for developingfeeding problems– Medical feeding problems were related to birth weightfor GA but not to GA alone– GI pathology related to GA 34 weeks– Medical interventions strongly related to GARommel N, Meyer AMD, Feenstra L, et al. The complexity of Feeding Problems in 700 Infants and Young ChildrenPresenting to a Tertiary Care Institution. Journal of Pediatric Gastroenterology and Nutrition. 2003; 37:75-84.34
Summary Multidisciplinary approach Thorough history and physical Diagnostic testing is sometimes needed Many different causes for feeding problems35
PsychologyLaura Slosky, PhD36
Approximately ½ to ⅔ of children with feeding disorderspresent with mixed etiology that includes behavioral,physiological, and developmental factors (Budd, et al.,1992; Rommel, et al., 2003). A psychologist is uniquely equipped to evaluate and treatthese contributory factors.37
The Pediatric Psychologist:– provides a behavioral perspective on the feeding problem– assesses for comorbid behavioral or psychiatric conditions impacting thechild or the broader family system– provides referrals as appropriate– Addressing feeding behavior38
Behavioral Perspective Missed or delayed stages of feeding development Learned avoidance secondary to aversive conditioning Frequency and severity of challenging mealtime interactions Behavioral refusals that have been inadvertently reinforced by caregivers Inappropriate family or cultural expectations for feeding39
Comorbidities Child:– Inattention– Hyperactivity– Anxiety– Developmental Complexities– Oppositionality– Many others as feeding is a highly heterogeneous population40
Comorbidities Caregivers:–Caregiver stress!–Parent mental health***These all impact caregiver ability to adhere to treatment plansand to follow through with their child on a consistent basis.***41
Referrals Often need to build basic behavioral skills– Hard time getting child to do something that is hard for them when a basicrequest results in a tantrum! Outpatient behavioral therapy Psychiatry Parent Supports– This is stressful!42
Behavioral Feeding Interventions Implementation of mealtime structure!! Structured feeding schedule Appetite Manipulation Behavior Management– Differential Attention– Reinforcement Strategies– Extinction of negative feeding behaviors– Consistent Contingency Management43
Behavioral Feeding Interventions Parent Training– Train the parent to become the child’s therapist– Changing Parent-Child Interaction Pattern– Changing the Feeding Behaviors of both parent and child– Consistency!!!44
NutritionJamie Wilkins, RD45
Speech-Language PathologyBrenda Sitzmann, MA, CCC-SLP, CLC52
Speech-Language Pathology Assess for oral and pharyngeal dysphagia Overlap with OT Collect history as a team Current and past therapy services Clinical signs of aspiration Preferred and non-preferred foods Helpful strategies53
Speech-Language Pathology Complete feeding assessment Observe a typical feeding with caregivers Ideally with preferred and non-preferred foods Evaluating oral motor feeding skills Assessing for aspiration Trial therapy techniques54
Speech-Language Pathology Recommendations Work with team members Feeding therapy Home programming Mealtime structure Therapy techniques55
Speech-Language Pathology Recommendations (continued) Additional evaluations Videofluoroscopic swallow study FEES Nutritional needs Prioritize foods to add Safe for chewable vitamin?56
Occupational TherapyFeeding Skills: Posture & Tone,Sensory-motor, Oral-motorElizabeth Schroeder, MOT, OTR/L57
Observation prior to feeding Motor milestones– Are they developmentally appropriate? Why not? Tone driven posturing– Do they have spasticity or hypotonia negatively effecting self-feeding andposture– Asymmetry – torticollis Breathing differences– Do they have mobility in chest and shoulders for breathing58
Posture & Tone Fine movements of the jaw and tongue needed forfeeding are dependent on – Head control, which is influenced by Trunk alignment, which depends upon – The stability of the pelvic area. All that to say: seating is so important!59
Postural Goal Neutral pelvis with slight anteriortilt Thighs should be parallel and hips bent to 90 degreesSymmetry through shoulders not elevated or rotated Knees should be bent to 90 degrees with toes pointing forwardPlacement of tray at nippleheight Feet in contact with surface Symmetrical elongated trunknot leaning60-
Sensory Processing“The ability to take in information from all ofthe senses, process that information andthen produce an adaptive response”- JeanAyres61
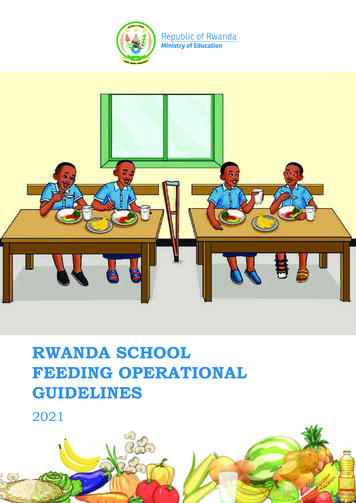
Sensory ProcessingLike itDislike itActiveSeeker-prefer big flavors-over fillingAvoider-gag/vomit-push away from tablePassiveBystander-pockets food-loses food in mouthSensor-difficult to engage-inconsistent preferences62
External Sensations Sight– looks away from food; tray is overwhelming Sound– Covers ears; startles to noise; distractible Smell– Covers nose; prefer bland food Touch– Frequent hand wiping; finger splaying63
Oral-Sensory Texture– Gagging, scraping off tongue, predictable pattern Taste– Grimacing, shuddering Proprioception– Over filling, looses food in mouth, swallows food whole Praxis– Difficulty learning oral movements, unpredictable motor skills64
References Cohen SA and Navathe AS. Nutrition and Feeding For Children with Developmental Disabilities. In: Wyllie Rand Hyams JS, ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 92. Grossman AB Liacouras CA. Gastroesophageal Reflux. In: Bell LM, ed. Pediatric Gastroenterology: TheRequisites in Pediatrics. Philadelphia: Mosby; 2008:74-85. Harding C, Faiman A, Wright J. Evaluation of an intensive desensitisation, oral tolerance therapy and hungerprovocation program for children who have had prolonged periods of tube feeds. Int J Evid Based Healthc2010;8(4):268-276. Ishizaki A, Hironaka S, Tatsuno M, et al. Characteristics of and weaning strategies in tube-dependent children.Pediatr Int 2013;55(2):208-213. Markowitz JE and Liacouras CA. Allergic and Eosinophilic Gastrointestinal Disease. In: Wyllie R and Hyams JS,ed. Pediatric Gastrointestinal and Liver Disease. Philadelphia: Saunders; 2011: Ch. 38. Manikam R and Perman JA. Pediatric Feeding Disorders. Journal of Clinical Gastroenterology. 2000. 30;1,34-46. Mukkada VA, Haas A, Maune NC, et al. Feeding Dysfunction in Children with Eosinophilic GastrointestinalDiseases. Pediatrics. 2010; 126:e672-677.65
References McSweeney ME, Kerr J, Amirault J, et al. Oral Feeding Reduces HospitalizationsCompared with Gastrostomy Feeding in Infants and Children who Aspirate. The Journalof Pediatrics. 2016;170:79-84. Pentiuk S, O'Flaherty T, Santoro K, et al. Pureed by gastrostomy tube diet improvesgagging and retching in children with fundoplication. JPEN J Parenter Enteral Nutr2011;35(3):375-379. Rommel N, Meyer AMD, Feenstra L, et al. The complexity of Feeding Problems in 700Infants and Young Children Presenting to a Tertiary Care Institution. Journal of PediatricGastroenterology and Nutrition. 2003; 37:75-84. Sherman PM, Hassall E, Fagundes-Neto U, et al. A Global, Evidence-based Consensuson the Definition of Gastroesophageal Reflux Disease in the Pediatric Population. TheAmerican Journal of Gastroenterology. 2009; 104:1278-1295.66
THANK YOUGI Multidisciplinary Feeding Clinic(816) 302-8037* All numbers Fiscal 201667
Interdisciplinary Pediatric Feeding & Swallowing Program Multidisciplinary Feeding Clinic at Adele Hall Focus of today's presentation GI, psychology, nutrition, speech and OT Multidisciplinary Feeding Clinic at CMK GI NP, pediatrician, psychology, nutrition, OT Similar to MDFC but no SLP services