Transcription
Qualification Form InstructionsCongratulations on taking steps toward maintaining or improving your health!The Blue Cross Blue Shield of Michigan qualification form is enclosed for you and yourphysician to complete. Be sure to submit the form in time to meet your employer’sdeadline. Do not submit any other versions of the qualification form; only the enclosedform will be accepted. The enclosed example shows how to fill out the form.Here’s how to fill out the qualification form:1. Complete the Member Information section with either blue or black pen. If yourform has prepopulated information, please do not modify those fields. If theinformation is not correct, please contact the BlueHealthConnection program at1-800-775-Blue (2583).2. Make an appointment with your doctor as soon as possible to complete the restof the form. An illegible entry or leaving a field blank will make your form invalid.We can process your form only if all sections are complete and your physicianhas signed the form.3. After your qualification form is completed by your physician, fax it to Blue CrossBlue Shield of Michigan at 1-866-392-6496 before the deadline. It is yourresponsibility to ensure the form is faxed to the Blues. Keep your form and yourfax confirmation in a safe place, in case you need to resend it.DF 12055 AUG 11Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee of the Blue Cross and Blue Shield Association.
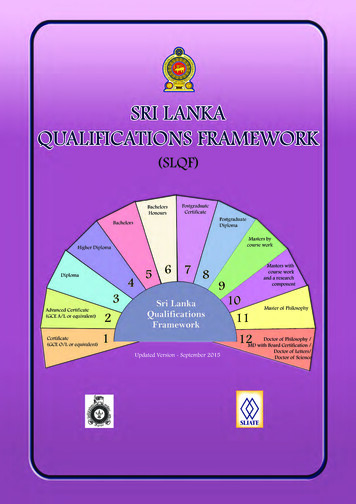
Sample forms and instructionsSample of member ID card:121. Location of theEnrollee ID orContract number— do not enter thefirst three letters ofyour Enrollee ID onthe qualificationform2. Location of theGroup NumberSample: front of qualification form(Please use the official form enclosed.)Member instructionsfor front of form:Complete boxes 2through 10 that havenot been filled in foryou. Have your doctorcomplete boxes 1 and11 through 29. If yourform has prepopulatedfields, please do notmodify them.For boxes 4 and 5,see the sample IDcard for the location ofthe Enrollee ID andGroup Numbers. Donot include the firstthree letters in yourEnrollee ID number.Make an appointmentwith your physician.Take the form for thephysician to complete.Physicianinstructions for frontof form:Complete boxes 1 and11 through 29.
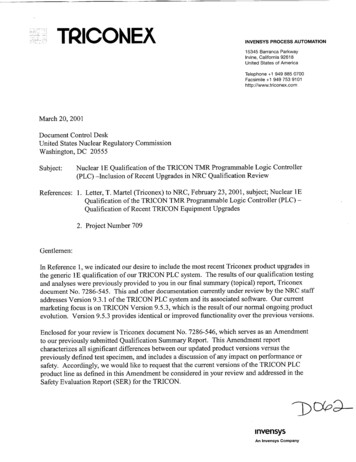
Sample back of form:Physicianinstructionscontinued:Complete boxes 30through 48.Member instructionscontinued:Complete boxes 49through 52.Fax the completedform to the fax numberon the form.
2011.Jun.v1Member sectionQualification FormMember instructions:Complete the top section of this form and take it to your physician tocomplete the bottom part of the form.Fax your completed form to 1-866-392-6496Member last nameMember first nameBCBSM use onlyExam date (mm/dd/yyyy)Contract or enrollee ID number (example: 123456789)Group number (five- or nine-digit number)Daytime telephone numberDate of birth (MM/DD/YYYY)Member signatureMember email addressGender (Check one) Male FemalePhysician instructions:Complete all the fields below, and sign this form. Return the form to the member to fax it to Blue Cross Blue Shield ofMichigan. Do not forward this form through the Provider Secured Services websites on bcbsm.com or mibcn.com.For Healthy Blue Outcomes only:If it is unreasonably difficult or medically inadvisable for the member to achieve the health measure criteria below due toa medical condition, complete the medical waiver form available on web-DENIS or the Provider Secured Services.Health measure criteria(Do not write in this column)Patient’s measurements(Write measure in this column)Physician sectionTobacco Nontobacco user (never used or quit 1 mo.)Tobacco user:WeightHeight feet:Height inches:Weight:BMI:Systolic:Diastolic:LDL:HDL:Total cholesterol:FBS: report for patientswithout diabetes.Triglyceride:A1C: report for patients withdiabetes.Nontobacco user:Body mass index 30Blood pressure 140/90CholesterolLDL 160HDL 40Total Cholesterol 200Triglycerides 150Blood sugarPatients without diabetes, normal fastingblood sugar orPatients with diabetes, A1C 8%Physician signature: I verify the information supplied is complete and accurate.Physician last namePhysician first nameNational provider identifierPhysician signaturePhysician telephone numberDate (mm/dd/yyyy)Fax form to 1-866-392-6496Questions? Call toll-free, 1-800-775-Blue (2583)WF 11947 JUN 11
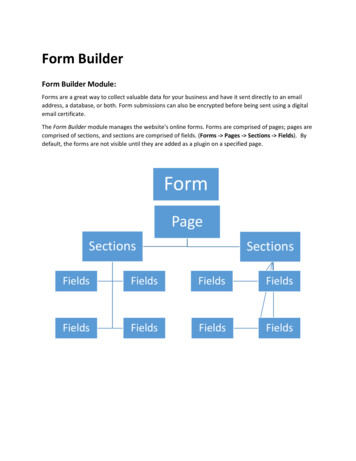
Physician instructions:If the member does not meet one or more of the health measure criteria listed on the front page, document the member healthimprovement plan below. The plan is between the health care provider and member. This is not a medical waiver form for Healthy BlueOutcomes.The member health improvement plan must include: Goal of the plan Patient actions to modify behavior, lifestyle or adherences to medical recommendations Follow up visit plan established in accordance with physician recommendationsSelect health risksHealth measure criteriaGoals metTobacco useNo tobacco use 1 monthYesNoWeightBMI 30YesNoBlood pressure 140/90 (both systolic and diastolic)YesNoCholesterolLDL 160Normal fasting blood sugar or patients withdiabetes A1C 8%YesNoYesNoBlood sugarGoals:Patient actions (document the plan in the member’s record):Frequency of follow up visits:weeksmonthsPhysician last namePhysician first namePhysician signatureDate (mm/dd/yyyy)Member last nameMember first nameMember signatureDate (mm/dd/yyyy)
a medical condition, complete the medical waiver form available on web-DENIS or the Provider Secured Services. Health measure criteria (Do not write in this column) Patient's measurements (Write measure in this column) Tobacco Nontobacco user (never used or quit 1 mo.) Tobacco user: Nontobacco user: Height feet: Height inches: Weight