Transcription
Key performance indicators in hospital based on balanced scorecard modelHamed Rahimi1, Zahra Kavosi2,*, Payam Shojaei3, Erfan Kharazmi2Received 3 Aug 2016 ; Accepted 25 Nov 2016ABSTRACTIntroduction: Performance measurement is receiving increasing verification all over the world. Nowadays in a lot of organizations,irrespective of their type or size, performance evaluation is the main concern and a key issue for top administrators. The purpose of thisstudy is to organize suitable key performance indicators (KPIs) for hospitals’ performance evaluation based on the balanced scorecard(BSC).Method: This is a mixed method study. In order to identify the hospital’s performance indicators (HPI), first related literature wasreviewed and then the experts’ panel and Delphi method were used. In this study, two rounds were needed for the desired level ofconsensus. The experts rated the importance of the indicators, on a five-point Likert scale. In the consensus calculation, the consensuspercentage was calculated by classifying the values 1-3 as not important (0) and 4-5 to (1) as important. Simple additive weightingtechnique was used to rank the indicators and select hospital’s KPIs. The data were analyzed by Excel 2010 software.Results: About 218 indicators were obtained from a review of selected literature. Through internal expert panel, 77 indicators wereselected. Finally, 22 were selected for KPIs of hospitals. Ten indicators were selected in internal process perspective and 5, 4, and 3indicators in finance, learning and growth, and customer, respectively.Conclusion: This model can be a useful tool for evaluating and comparing the performance of hospitals. However, this model is flexibleand can be adjusted according to differences in the target hospitals. This study can be beneficial for hospital administrators and it canhelp them to change their perspective about performance evaluation.Keywords: Hospital, Balanced scorecard, Performance, Indicator Please cite this paper as:Rahimi H, Kavosi Z, Shojaei P, Kharazmi E. Key performance indicators in hospital based on balanced scorecard model. J Health Man &Info. 2017;4(1):17-24.IntroductionHealth care system has become one of the world’s largest,costly and fastest-growing industries as it forms a massivepart of a country’s economy (1). Healthcare system is oneof the most noticeable section of service sectors. In themost developing countries, more than five percent of grossdomestic products (GDP) is allocated to health care sector.Hospitals consume more than 50 percent of total healthresources, so they are an important unit of the healthsystem (2-4). Health care organizations have to deal withan unstable environment due to various factors such as therapid transformation of technology, demographic factorsand change in lifestyles (5). Evaluation of the performanceof hospitals is of paramount importance because of thehospitals’ impact on the efficacy of health systems(6). Performance measurement system is a process of123assessing the organization progress in achieving the goalsand objectives. The idea of measuring performance is notonly to identify the current performance of the business,but also to enable the business to perform better in thefuture (7, 8).Performance evaluation is receiving increasing verificationall over the world. Nowadays in a lot of organizations,irrespective of their type or size, performance evaluationis the main concern and a key issue for top administrators(9, 10). Performance evaluation is an assessment modelto compare past plans and implementation of strategies,operating activities of organizations with executiveabilities, participating rate and competing rate of theemployees. In addition, this assessment model is helpingthe organizations to plan future strategies and set upperformance targets of the employees in order to achievethe final target of the entire organizations (11). It canSchool of Management and Medical Information, Shiraz University of Medical Sciences, Shiraz, IranHealth Human Resources Research Center, School of Management & Information Sciences, Shiraz University of Medical Sciences, Shiraz, IranDepartment of Management, Shiraz University, Shiraz, Iran*Corresponding Author: Z Kavosi, Health Human Resources Research Center, School of Management & Information Sciences, Shiraz University of Medical Sciences,Shiraz, Iran. Email: zhr.kavosi@gmail.com.
Rahimi H et al.equip the managers with the information they need forthe evaluating, controlling and monitoring of hospital’scurrent situation and effective technique to assessand supervise hospital activities (6, 12). Evaluation ofhospital performance is beneficial to payment systems,policymakers, hospitals, and physicians. The assessmentalso assists the managers in promoting the quality ofperformance (13).The main property of a perfect performance evaluationsystem is the accuracy of its outcomes. Thus, it is importantto choose the proper methods and reasonable indicatorsthat reflect the purpose of the performance evaluation (14).A set of indicators that properly reflect the organizationalperformance should be set up to fully utilize the functionof performance measurement. (15).Organizational performance is not a simple phenomenon;rather, it is a complex and multidimensional concept(16). Various models have been used to manage theorganizational activity and performance, including totalproduction analysis, Analytical Hierarchical Process(AHP), ratio analysis, Delphi analysis, Data EnvelopmentAnalysis (DEA), Six Sigma, Total Quality Management(TQM), and Balanced Scorecard (BSC), (1, 15, 17).The balanced scorecard is seen as a powerful tool fororganizational change and as an effective performancemeasurement system.Balanced scorecard developed in 1992 as a managementaccounting tool that translates an organization’s mission,strategies, and goals into performance measuring. TheBSC consisted of four perspectives such as financial,internal process, learning and growth and customer (5,15, 18). Balanced scorecard perceived as the most properframework is able to provide remarkable informationrelevant to the organizational internal and external factorsthat will subsequently contribute to the organization’ssuccess (1). The BSC is used increasingly for measuringand reporting health system performance. In this method,indicators are located in different perspectives, whichprovides a balanced view of performance and guidesstrategic decisions at the hospitals (19-21). This is forsetting up a complete performance evaluation systemand forming a whole set of performance indices toassess strategies so that the strategies and prospect oforganizations could be achieved (11).The BSC model indicates that a single performanceindicator could not show the performance of a complexorganization such as hospitals (9, 22). The advantages of theBSC are classified into three aspects, i.e. communicationand teamwork, commitment, and feedback and learning.The BSC enables the senior management to clarifyvision, develop teamwork, expand strategy, and foster theobligation to customer focus in the organization (23, 24).Thus, organization performance is a multi-criteriadecision-making (MCDM) issue. MCDM is relatively newto be used for the evaluation of performance. MCDM aimsat using a set of criteria for decision problem (10). One ofthe MCDM methods is simple additive weighting (SAW)which is known as a simple and most often used multiattribute decision technique (25-27). The purpose of thisstudy was to organize suitable key performance indicators(KPIs) for hospitals’ performance evaluation based on theBSC perspectives using SAW.MethodsThis is a mixed method study in which, depending onvarious phases of the investigation, various tools havebeen used (2013-2014). In order to identify the hospital’sperformance indicators (HPIs), first related literature wasreviewed and then the experts’ panel and Delphi methodwere used. The SAW technique was used to rank theindicators and select hospital’s KPIs.Literature reviewThe literature review was carried out to identify relevantstudies by searching electronic databases. We conducteda search of the literature for articles on PubMed, Scopus,Sciences direct, Google scholar, DOJA, SID, Iranmedex,Magiran, and Medlib databases.Keywords used for searching was a combination of“hospital,” “performance,” “assessment,” “evaluation,”“measurement,” “indicator,” and “criteria.” The BooleanOR AND operators were placed between keywords in thesearches.First, the titles of all articles were reviewed by two of theauthors, and then abstracts of the selected articles werereviewed. Then, the full text of the selected articles wasstudied and articles in the area of HPIs, which were mostrelevant to our study’s objective, were selected. The qualityof the selected articles was assessed by the Strengtheningthe Reporting of Observation Studies in Epidemiology(STROBE) instrument. STROBE instrument wasproduced in 2007 to improve the quality of observationalstudy reporting and allow for critical assessment by othersof the strengths and weaknesses in study design, conduct,and analysis (28). STROBE addresses the three maintypes of observational studies: cohort, case-control andcross-sectional studies (29).Expert panelWe asked an experts’ panel with five experts in the fieldof health services administration from “health caremanagement” and “community medicine” departments ofShiraz University of Medical Sciences (SUMS) to identifyHIPs from the extracted indicators of literature reviewbased on four BSC perspectives. Seventy-seven indicatorswere selected during the internal expert panel.Delphi methodsWe used a Delphi method to reach a consensus among apanel of experts. With Delphi method, the consensus isachieved through a series of rounds. In this study, tworounds were needed for the desired level of consensus.We selected the experts for the Delphi survey to assessthe validity of the indicators. The experts comprised 17professionals from industry and academia. All of theexperts had more than five years of related experience andseven of them had more than fifteen years. In addition,twelve of experts from industry had been managers/directors of hospitals, and five from academia wereprofessors/researchers with healthcare managementJ Health Man & Info. Jan 2017;4(1):18
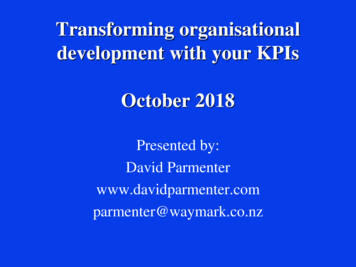
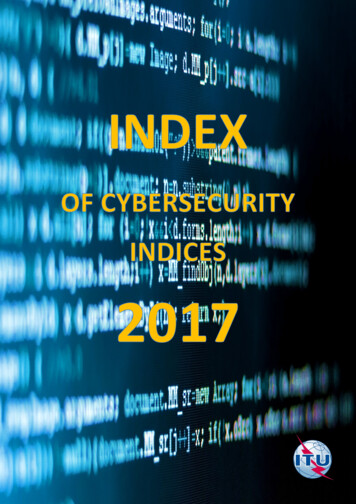
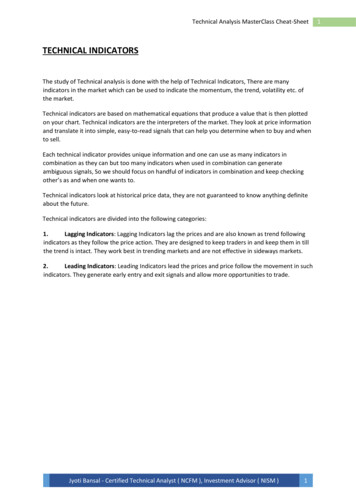
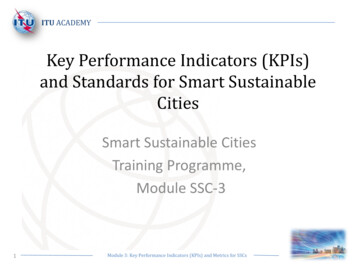
Key performance indicators in hospitalbackground. We guaranteed anonymity by assigning acode number to each participant. All of the participantswere anonymous volunteers.The data were collected using paper based survey. So,each expert completed two rounds of the Delphi survey.The first round was developed from indicators compiledas a result of the expert panel. Experts were given fivedays to complete the surveys. From the results of the firstround and comments listed by respondents, the secondround was developed. During the second round, individualand group results from the first round were presented tothe panel members and asked to indicate if they agreedor disagreed with each of remained indicators. All itemswhich did not receive agreement from 80% of the panelrespondents were removed from the list of indicators.In Delphi method, data were analyzed by descriptivestatistics using Excel software. The experts rated theimportance of the indicators, on a five-point Likertscale (“Not important,” “Somewhat important,”“Relative important,” “Very important,” and “Extremelyimportant,” respectively). The required level of consensuswas defined. Two necessary conditions had to be fulfilled:(1) a mean value of at least 4 (“Very important” and“Extremely important”) and (2) a consensus percentage ofat least 80%. In the consensus calculation, the consensuspercentage was calculated by classifying the values 1-3 asnot important (0) and 4-5 to (1) as important.Simple Additive Weighting (SAW)The SAW, which is known as a weighted linearcombination or scoring methods, is a simple and mostoften used multi-attribute decision technique. The SAWis based on the weighted average. The advantage ofsimple additive weighting is that it is a proportional lineartransformation of the raw data (25-27). The method of datacollection applied in this phase was a questionnaire, usingthe Likert scale from 1 to 5 (“Not important,” “Somewhatimportant,” “Relative important,” “Very important,” and“Extremely important,” respectively). The questionnaireswere completed by the participants of the Delphi method.The process of SAW consisted of the following steps (2527):Step 1:Determining and computing the weight of the criteriawere used as a reference in decision-making, namely Ci.In this study, the four selected criteria were necessity,specificity, relatively, and measurable.Step 2:Making a decision matrix (m n) that includes m indicatorsand n criteria. Calculating the normalized decision matrixfor positive criteria (1) and negative criteria (2):Step 3:Assessing each indicator, Ai by the following formula:A i cj .xij(3)Where xij is the score of the ith indicator according to thejth criteria, Cj is the weighted criteria.ResultsResults of literature review and expert panelA total of 39 studies were identified for inclusion in thereview. The search of databases provided a total of 14,842citations. Initially, the title of all the articles was checkedout and 13,985 were excluded owing to contradiction withthe study objectives. After adjusting for duplicates, 309articles were remained. Of this number, 173 articles wereomitted because after reviewing the abstracts it emergedthat these articles clearly did not meet the criteria andthere was a lack of indication to hospitals’ performanceindicators in their results. Sixteen articles were rejectedbecause the full text of the article was not accessible, thepaper could not be feasibly translated into English, thepaper was not in the English language, or the type of thearticle was not original. The full texts of the remaining120 articles were studied in more detail. It emerged that64 article did not meet the inclusion criteria. Then, usingthe STROBE instrument, we assessed the quality of 56remained articles and 39 of them had the quality needed.Finally, 39 studies (23 English and 16 Persian) met theinclusion criteria and were included in the literaturereview (Figure 1). Two hundred ninety-eight indicatorswere obtained from a review of selected literature.Finally, throughout the internal expert panel, 77 indicatorswere selected. These performance indicators wereclassified into four perspectives of BSC: finance (20),the customer (5), internal process (37), and learning andgrowth (15).Evaluation criteria by Delphi methodTwenty criteria were selected by the first Delphi round and30 criteria by the second Delphi round. Results of the tworounds are shown in Table 1.Simple Additive WeightingFirst, the weights of the criteria were computed by usingfive experts’ opinion with Interview: Necessity (C1) 0.4,Specificity (C2) 0.15, Relatively (C3) 0.15, and Measurable(C4) 0.3.Then, we calculated the normalized decision matrix forthe criteria used in this study; the criteria were positive,so we used formula 1, and the result is shown in Table 2.The SAW method evaluates each alternative (Ai) byformula 3. In this step, indicators of each BSC perspectiveare ranked separately. Finally, in SAW method, the bestindicators were P1, F9, G3, and C2 in the internal process,finance, learning and growth and customer perspective,respectively. The results of SAW method are shown inTable 3.Key performance indicatorsBased on the results in Table 4, 22 indicators were selectedfor KPI of hospitals. Ten indicators were selected in theinternal process perspective and 5, 4, and 3 indicators infinance, learning and growth, and customer, respectively.The result is shown in Table 4.J Health Man & Info. Jan 2017;4(1):19
Rahimi H et al.Figure 1. Details of literature review processTable 1. Selected indicators of hospital performance by Delphi methodBSC perspectivesIndicatorsIndicatorsFinance (F)F1Ratio of total revenue to total costsF6Current cost per bedF2% Deductions of hospitalF7the ratio of capital expenditures to current costsF3Average hospitalization expendituresF8the cost of drugs and materialsF4Average outpatient expendituresF9%Personnel costs of total costsF5Average expenditures per bed per dayF10Total fixed cost for per Bed occupancyP1average Length of stayP15Wrong-site surgeryP2Bed Turnover IntervalP16Leaving a foreign object during surgeryP3Bed occupancyP17Medication errorsP4bed turnoverP18wrong in the type of blood groupP5Mortality rateP19Patient falls rateP6Cancelled operationsP20Hospital accidents prevalence rateP7% Repeated surgeriesP21Sentinel event rateP8Discharge with Personal satisfactionP22Needlesticks and sharps injuryP9Hospital infection rateP23the legal complaint from a hospitalP10Clinical errorsP24Doctors on-call at nightP11Readmission rateP25Waiting time for admission operation roomP12% Occupational accidentsP26Mean Length of stay in emergency departmentP13Pressure Ulcers rateP27Emergency Room (ER) waiting timeP14Medical errorsP28Waiting time from triage to see doctorG1Staff satisfaction rateG6the amount of the electronic medical recordG2Staff turnoverG7number of days of sick leave to total employees ratioG3Training expenditures per capitaG8Employee absenteeism rateG4key Jobs Contains substituteG9Rate of employee sick-leaveG5Average hours of Internet useC1The facilities for families and visitorsC4Other Stakeholders satisfactionC2Patients satisfaction percentageC5Social satisfactionC3Rate of Patient complaintsInternal Process (P)Learning and Growth (G)Customer (C)J Health Man & Info. Jan 2017;4(1):20
Key performance indicators in hospitalTable 2. The normalized decision 7494G90.80630.81660.83930.9464Finance (F)InternalProcess (P)Learning andGrowth (G)G50.59570.69370.64020.7665Customer 10.96220.9011Table 3. The ranked indicators of hospital 55InternalP1Process 0.850921Finance 512G40.7623878G70.8458347Learning and G1Growth C50.7469045C211C40.7756764J Health Man & Info. Jan 2017;4(1):21
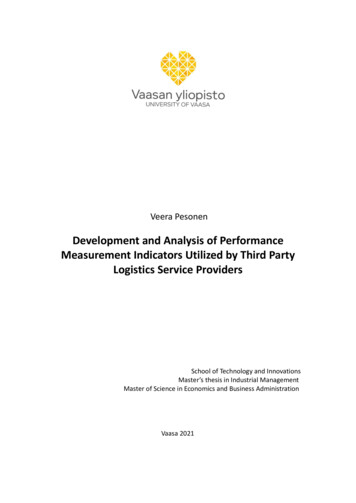
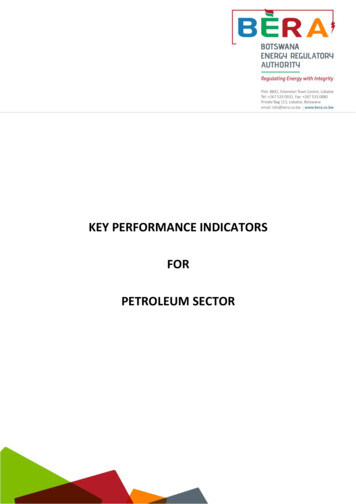
Rahimi H et al.Table 4. Key Performance Indicators (KPI) of hospital performanceBSC perspectivesIndicatorsIndicatorsFinance (F)F1F2F5Ratio of total revenue to total costsF8the cost of drugs and materials% Deductions of hospitalF9%Personnel costs of total costsInternal ProcessP1(P)P3P4average Length of stayP8Discharge with Personal satisfactionBed occupancyP9Hospital infection ratebed turnoverP10Clinical errorsP5Mortality rateP26Mean Length of stay in emergency departmentP6Cancelled operationsP27Emergency Room (ER) waiting timeG1Staff satisfaction rateG3Training expenditures per capitaG2Staff turnoverG8Employee absenteeism rateThe facilities for families and visitorsC3Rate of Patient complaintsLearning andGrowth (G)Customer (C)C1C2Average expenditures per bed per dayPatients satisfaction percentageDiscussionAccording to the results, 22 indicators were selectedfor KPI of hospitals using the opinion of the experts’panel. Ten indicators were selected in internal processperspective and 5, 4, and 3 indicators in finance, learningand growth, and customer, respectively.Hospital indicators represent the hospitals’ performancein different areas. So, it is essential to attend theseindicators (17, 30). Through this study, hospital indicatorswere classified based on balance scorecard under fourcategories as finance, internal process, learning andgrowth, and customer. This classification is consistentwith other studies (9, 31).In this study, 22 indicators were approved for KPIs inbalance scorecard. The mean indicators in the comparativestudy were 29. A study indicated that almost 30 indicatorswere used (32). Most researchers agree with 20- 25indicators although up to 30 indicators may be preferred(33).In the development of BSC, the number of indicators is notconsidered the main criterion, but it is also important tochoose the indicators with sufficient attention so that thekey and vital indicators are not removed (31).Ten performance indicators of finance perspective wereranked using SAW technique. Then, according to theexperts’ ideas, the first five indicators were selected asKPIs. KPIs in this perspective were personnel costs ofthe total cost (%), the ratio of total revenue to total cost,a discount off the hospital (%), average expenditures perbed per day, and cost of drug and materials, respectively.Nasiripour et al. showed that income per inpatient, incomeper outpatient, cost coverage; preventive maintenance costof the total budget and current cost per bed are financialindicators used to assess hospitals performance (9).Fadi El-Jardali et al. explained that the most importantperformance indicators to assess the hospitals financingare the cash-flow rate, total profit margin, debt servicecoverage, discount on total billed (%), and amounts by athird-party payer (19).Raeisi et al. selected five indicators of financial perspective;two indicators (% discount of hospital and % personnelcosts of total cost) were compatible with our results (31).In a study of Iravani Tabrizipour et al., eight indicatorswere selected and only one indicator (% discount off thehospital) was compatible with our results (34).Our findings are different in financial indicators in thestudy of Peters et al. They were facilities with user feeguidelines and facilities with exemptions for poor patients.Also, the findings of this study are not compatible withfinancial indicators in the study of Kocakulah and Austill;they were gross operating profit, days of available liquidity,and return on stockholder’s equity (35).Ten of the most important selected KPIs in the internalprocess perspective include the average length of stay,bed occupancy, mean length of stay in the emergencydepartment, mortality rate, bed turnover, discharge withpersonal satisfaction, Emergency Room (ER) waitingtime, hospital infection rate, canceled operations, clinicalerrors, respectively.Nasiripour et al. showed the length of stay, outpatient perdoctor, canceled operations, big surgery percent, in-patientper doctor, employee productivity, and bed occupancy (9).Raeisi et al. and Iravani Tabrizipour selected 14 and 10indicators to internal process perspective, respectively(31, 34).Inpatient mortality, unscheduled visits to the operatingroom, drug events per thousand of doses distributed,and fall off beds per 100 patient-days in the investigationof Kocakulah and Austill were selected as indicators ofinternal process perspective (35). Fadi El-Jardali et al.demonstrated 18 indicators in clinical utilization andoutcomes perspective (19). Arab et al. certified in theirresearch that the staying time in the hospital is a significantindicator which is utilized widely nowadays(36).Our experience demonstrates that most indicators are ininternal process perspective. These findings are compatiblewith Kaplan and Norton’s view about the necessity of thenumber of indicators in perspective internal processes(37).The tertiary perspective of balance scorecard is learningand growth. KPIs in this perspective were Trainingexpenditures per capita, staff satisfaction rate, employeeabsenteeism rate, and staff turnover, respectively.J Health Man & Info. Jan 2017;4(1):22
Key performance indicators in hospitalNasiripour et al. reported training expenditures per capita,sickness absence rate, employee satisfaction, percutaneousinjuries, training expenditures, and informationtechnology (IT) efficiency (9). Raeisi et al. and IravaniTabrizipour selected eight and seven indicators to internalprocess perspective, respectively (31, 34).Fadi El-Jardali et al. used staff satisfaction rate, staffturnover rate, employee absenteeism, and rate of employeesick-leave (19).In customer perspective, selected indicators were patients’satisfaction percentage, rate of patients’ complaints, thefacilities for families and visitors, respectively, that arecompatible with the findings of the study conducted byRaeisi et al., Barati et al., and also with the findings ofNasiri et al. (9, 31, 38). Fadi El-Jardali et al. used patient’ssatisfaction rate and discharge against medical advice(19). Peters et al. used overall patient satisfaction, patientperception of quality index, and written shura-e-sehieactivities in the community (39).Evaluation of the customers’ opinions is basicallyimportant because there is a serious competition betweenhospitals in the conditions of admission patients, reductionof medical costs, and earning more money (30).A limitation of this study was lack of proper definition forstrategic objectives. So, these indicators might not suitablefor all hospitals. However, BSC model is flexible and canbe adjusted according to differences in target hospitals.Furthermore, the study selected the key indicators fordeveloping the balanced scorecard for hospitals ratherthan evaluation and comparison of hospital performance.Therefore, it is recommended that in future studies thismodel ishould be used to evaluate and compare thehospitals performance.ConclusionOur research has presented KPIs on BSC model, which canbe used for the performance assessment in hospitals. Thisstudy can be beneficial for hospital administrators and itcan help them to change their thinking about performanceevaluation. Identifying the hospitals’ KPIs provides anopportunity for hospital administrators to recognizecritical points with lower costs and time. Thus, the areasof improvement for each hospital could be identified. Thismodel can be a useful tool for evaluating and comparingthe performance of hospitals. However, this model isflexible and can be adjusted according to differences intarget hospitals. We recommend that hospitals shoulduse our work as a framework for evaluating their ownperformance. Future studies could use this frameworkfor evaluating hospitals performance, identifying thefunctional weakness of hospitals, and ranking hospitals.AcknowledgementsThe authors would like to thank the experts’ panelbecause this survey would not have been possible withouttheir assistance. This article was extracted from the thesiswritten by Hamed Rahimi and financially supported byShiraz University of Medical Sciences grants No. 93-7014.Conflict of InterestNone 4.15.16.17.18.19.20.Shukri NFM, Ramli A. Organizational Structure andPerformances of Responsible Malaysian Healthcare Providers:A Balanced Scorecard Perspective. Procedia Economics andFinance. 2015;28:202-12.Lotfi F, Kalhor R, Bastani P, Shaarbafchi Zadeh N, EslamianM, Dehghani MR, et al. Various indicators for the assessmentof hospitals’ performance status: differences and similarities.Iranian Red Crescent medical journal. 2014;16(4):e12950.Abdullah MT, Shaw J. A review of the experience of hospitalautonomy in Pakistan. The International journal of healthplanning and management. 2007;22(1):45-62.Abolhallaje M, Bastani P, Monazam K, Abolhasani N,Ramezanian M. Health System Financing from ExpertsPoint ofView. Middle-East J Sci Res. 2012;12(10):1386-90.Koumpouros Y. Balanced scorecard: Application in the GeneralPanarcadian Hospital of Tripolis, Greece. International Journalof Health Care Quality Assurance. 2013;26(4):286-307.Bahadori M, Sadeghifar J, Hamouzadeh P, Hakimzadeh SM,Nejati M. Combining multiple indicators to assess hospitalperformance in Iran using the Pabon Lasso Model. TheAustralasian medical journal. 2011;4(4):175.Kairu EW, Wafula MO, Okaka O, Odera O, Akerele EK.Effects of balanced scorecard on performance of firms in theservice sector. European Journal of Business and Management.2013;5(9):81-8.Okwo IM, Marire IM. Performance Measurement in BusinessOrganizations: An Empirical Analysis of the FinancialPerformance of Some Breweries in Nigeria. Research Journal ofFinance and Accounting. 2012;3(11):48-57.Nasiripour AA, Afshar Kazemi MA, Izadi A. Designing ahospital performance assessment model based on balancedscorecard. HealthMED. 2012;6(9):2983- 9.Tsai H-Y, Chang C-W, Lin H-L. Fuzzy hierarchy sensitive withDelphi method to evaluate hospital organization performance.Expert Systems with Applications. 2010;37(8):5533-41.Wu H-Y, Lin Y-K, Chang C-H. Performance evaluation ofextension education centers in universities based on the
(AHP), ratio analysis, Delphi analysis, Data Envelopment Analysis (DEA), Six Sigma, Total Quality Management (TQM), and Balanced Scorecard (BSC), (1, 15, 17). The balanced scorecard is seen as a powerful tool for organizational change and as an effective performance measurement system. Balanced scorecard developed in 1992 as a management