Transcription
Tracheostomy: Procedures, Timing and TubesTRACHEOSTOMY:PROCEDURES, TIMING AND TUBESGail M. Sudderth RRTClinical SpecialistPassy-Muir Inc.gsudderth@passy-muir.com(949) 833-8255Objectives Explain how the timing of the tracheotomy andtube selection criteria plays a key role in successfuluse of speaking valves. List complications of improper cuff management.Indications for Tracheostomy Prolonged mechanical ventilation Inability to perform trans-laryngeal intubation(trauma, max/fax deformity) Upper airway obstruction (temporary or permanent) Secretion management (neuromuscular disease) List how the tracheostomy tube and inflated cuffcan impact swallowing and suggest ways toreduce clinical complications.Reputed Benefits Improved patient comfort/less need for sedationLower WOB/faster weaning from MVImproved safetyImproved oral hygiene and oral intakeLess long term laryngeal damageLower VAP ratesLower mortalityReduced ICU and overall LOSEarlier ability to speak/ Improved participationWHEN: TIMING OF TRACHEOTOMY21 Days ?7-10 Days ?2-3 Days ?Does timing affect outcomes ?What does the literature say ?Durbin, C. Resp Care 2010;55(8):1056‐1068Gail M. Sudderth, RRTClinical Specialist1
Tracheostomy: Procedures, Timing and TubesEndotracheal Tube Factors Cited To Contribute ToSwallowing Impairment and AspirationLaryngeal Intubation Granuloma Mucosal injury to theoral pharynx and larynx Injury to the vocal foldswhichhi h may beb transientti tor permanent Tracheal edema,ulceration and stenosisReproduced with permission from Houston Otolaryngology www.ghorayeb.comHOW: TRACHEOTOMY PROCEDURESPercutaneous TracheotomyOpen or Surgical TracheotomyTried and True MethodPercutaneous Dilatation or Balloon DilatationTracheotomyLLesscostlytl andd more convenienti tCricothyoidotomyAs seen on ER ShowsDoes the method of tracheotomy affect outcomes ?Permission for use granted by Cook Medical Incorporated, Bloomington, IndianaCricothyroidotomyParts of a tracheostomy tube - ISO STANDARDSNeck flangeTube shaftCuff15 mm connectorInflation linePilot balloonPilot port with one way valvePermission for use granted by Smiths MedicalGail M. Sudderth, RRTClinical Specialist2
Tracheostomy: Procedures, Timing and TubesTracheostomy Tubes Single Lumen/CannulaRoutine Tracheostomy Tube Changes Double Lumen/Cannula After initial tracheotomy– Surgeon preference Types of Tubes MATERIALS– PVC, Silicone, Metal– Metal Reinforced SHAPE– Curved, Angular, NonNonpre formed LENGTH– Standard– Extra length Proximal Distal Adjustable FlangeTo assure stoma and tract establishedTo reduce complicationpof ggranulation tissueFor down-sizingDifficult airways and special considerationsJackson Tracheostomy Tubes SINGLE LUMENDOUBLE LUMENFENESTRATEDMRI COMPATIBLES b l tti SSuctionSubglottictiTrach TalkCUFFS Improved Inner Cannula Original Style– Air, water, or foam– Double cuffed– Un-cuffed Custom MadeJackson Metal Tracheostomy TubesPMV 2020 (clear) With Jackson Improved Original Style Improved Permanent 15mmAdapterGail M. Sudderth, RRTClinical Specialist3
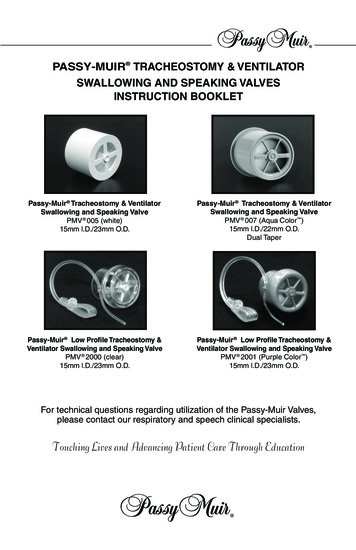
Tracheostomy: Procedures, Timing and TubesCalculating Tube SizeFenestrated Tracheostomy Tube ATS Consensus: Thetracheostomy tubeshould take up no morethan 2/3 the ID of thetracheatrachea.(for pediatrics, no adult standard)tracheaO.D. I.D. AP Diameter of tracheatube– Male:18 /- 5mm– Female: 12 /- 3 mmImage used by permission from Nellcor Puritan Bennett LLC, Boulder, Colorado, doing business as CovidienNot all size 6 trachs are equal !!Extra Length TubesSize 6.0 TracheostomyIDOD LPortex6.0 8.3 55.0Bivona6.0Shiley6.4 10.8 74.0SCT6.08.88.3distalproximal70.067.0Tracheal Malacia or StenosisIncreased skin‐to‐tracheal‐wall distanceImage used by permission from Nellcor Puritan Bennett LLC, Boulder, Colorado, doing business as Covidien.”Adjustable Flange TubeCuff Choices AIR FILLED – minimalleak TTS : WATER FILLED –minimali il occlusionl i((canbe air filled) FOME-Cuf – selfsealingGail M. Sudderth, RRTClinical Specialist4
Tracheostomy: Procedures, Timing and TubesAir Filled Cuffs Cuff InflatedWater Filled Cuffs TTS Cuff DeflatedCuff: Choices and Management Cuff Up Cuff DeflatedCuff Management – Minimal Leak Cuff up or down ?– Purpose of cuff– Cuffs and aspiration Cuff pressures– 18-22* cm H20– Minimal Leak– Minimal occlusionCuff Management – Direct MeasureClinical Complications - Cuff Gail M. Sudderth, RRTClinical SpecialistEsophageal impingementRefluxNecrosis and TraumaLaryngeal tetheringReduced airwayprotection5
Tracheostomy: Procedures, Timing and TubesCuff Over-InflationClinical Complications Reduced Airflow– Taste, Smell, Sensation– Voice Reduced Positive AirwayPressureAirflow––––Physiologic PeepCoughValsalvaSwallow Late Complications– Granuloma-Stenosis– Tracheal Malacia– FistulaeBenefits of Passy-Muir Valve Improved Voice/SpeechImproved Smell & TasteImproved SwallowMay Reduce AspirationImproved SecretionManagementRestored PEEPImproved OxygenationImproved Quality of LifeExpedites Weaning andDecannulationCost SavingsShorter Lengths of StayRoutine and Emergency Procedures SuctioningBroncho-pulmonary HygieneOxygen and Humidity TherapyTrach Care/Stoma CareInner Cannula Change CleaningOral CareUnplanned DecannulationBlocked Tube or Inner CannulaGail M. Sudderth, RRTClinical SpecialistAirway Assessment How does tube size andtype affect airwayassessment ?– Tube must be smallenough for adequateairflow.i fl– Cuff takes up space inthe airway– Tube length may causeresistance to airflow– Foam cuff is absolutecontraindicationDecannulation Plan Begins at Intubation-What is the Plan ? Evaluation for Decannulation–––––––Reason for tracheotomy has resolvedMedically stablePatent upper airwayTolerates speaking valveCan manage oral and tracheal secretionsTolerates capping/pluggingRisk of aspiration assessed6
Tracheostomy: Procedures, Timing and TubesAirway Management Team “Tracheostomy expertise must follow the patientwherever they go in the hospital.” Heffner, John E. Team Approach– Timing and tube selection– When to downsize– Plan of care Communication Swallowing– Decannulation– Impacts continuity of care– Impacts safety, length of stayand costsResources Cameron, T et al. Outcomes of patients with spinalcord injury before and after introduction of aninterdisciplinary tracheostomy team. Crit CareResus Mar 2009;11(1);14-19. Kamel KS et al.al In vivo and In vitro morphology ofthe human trachea. Clin Anat, 22:571-79, 2009. Durbin, CG. Tracheostomy: Why, When and How?Respir Care Aug 2010; 55(8);1056-6 Heffner, JH. Toward Leaner Tracheostomy Care:First Observe, Then Improve. Respir Care,2009:50(12)Resources www.Smiths-medical.com www.Cookmedical.comCook Medical Inc., Bloomington, Indiana www.Premusa.comwww Premusa comPremier Medical, Inc. Shiley Tracheostomy Pocket Click.aspx?fileticket AF0%2b2G%2bTVaU%3d&tabid 184 www.hopkinsmedicine.org/tracheostomy/aboutGail M. Sudderth, RRTClinical SpecialistResources Hess DR. Tracheostomy tubes and relatedappliances. Respir Care. Apr 2005;50(4):497-510. Yaremchuk K. Regular tracheostomy tubechanges to prevent formation of granulationtissue. Laryngoscope. Jan 2003;113(1):1-10. Epstein, S. Late Complications of Tracheostomy.Respir Care. Apr2005;50(4); 542-549. Johnson, et al. Tracheostomy Tube Changes.Clinical Procedures Jan 2010 (Medscape.com)Resources LeBlanc, et al. (2009) Outcome in TracheostomizedPatients with Severe TBI following Implementationof a Specialized Multidisciplinary TracheostomyTeam. Published in: Journal of Head and TraumaR h bRehab. Tobin A and Santamaria J (2008) An Intensivist-LedTracheostomy Review Team is Associated withShorter Decannulation Time and Length of Stay: Aprospective cohort study. Critical Care on-line at:www.medscape.com/viewarticle/575833Additional Educational Opportunities Self-study webinars available on demand–––––Getting StartedVentilator ApplicationSwallowingPediatricSpecial Populations Live group webinars www.passy-muir.com Passy-Muir Inc. is an approved provider ofcontinuing education through ASHA , AARC, CMSAand California Board of Nursing Credit7
Tracheostomy: Procedures, Timing and TubesReceiving CEU’s for this Course You will have 72 hours from the time this coursesends to complete the evaluation, which is requiredto receive credit.– Look in your email for a reminder link, or type this into yourI tInternett browser’sb’ addressddbar:b ep.passy-muir.comGail M. Sudderth, RRTClinical SpecialistGail M. Sudderth RRTClinical SpecialistPassy-Muir Inc.gsudderth@passy-muir.com(949) 833-82558
Improved oral hygiene and oral intake Less long term laryngeal damage Lower VAP rates Lower mortality Reduced ICU and overall LOS Earlier ability to speak/ Improved participation Durbin, C.Resp Care 2010;55(8):1056‐1068 WHEN: TIMING OF TRACHEOTOMY 21 Days ? 7-10 Days ? 2-3 Days ? Does timing affect outcomes ?