Transcription
NATIONAL INSTITUTES OF HEALTH OFFICE OF THE DIRECTOR VOLUME 30 ISSUE 1 JANUARY-FEBRUARY 2022Tackling DifficultProblems in Women’sHealth: ConferenceHighlightsBeyond the BooksA Dynamic NIH Library Inspires Innovation, Bolsters DiscoveryBY MICHAEL TABASKO, ODH i s t o r i c a l ly, m a n y m e d i c a ladvances have come from studies of menbecause women were underrepresentedas biomedical researchers and in clinicaltrials. Study findings were extrapolated towomen without taking into considerationsex differences such as in metabolism andresponses to medications. Even someanimals and cells used in studies weremale and assumptions were made aboutrelevance to females.Women’s health research took centerstage at the “Advancing NIH Research onthe Health of Women” videoconference,hosted by NIH’s Office of Research onWomen’s Health (ORWH) and held onOctober 20, 2021. The conference, whichfeatured 44 speakers, was held in responseto a congressional request to address threetopics: rising maternal morbidity andmortality rates; increasing rates of chronicdebilitating conditions in women; andstagnant cervical cancer survival rates.ORWH Founded Out of AdvocacyAwareness of inequities in research andhealth care was percolating in the 1960s asthe civil rights, women’s rights, and women’shealth movements were in full swing. In the1980s, the scientific, policy, and advocacycommunities began to respond; NIH’s RuthKirschstein, then director of the NationalCONTINUED ON PAGE 16CREDIT: KATHLEEN MCGLAUGHLIN, NIH LIBRARYBY TAMAR JACOBSOHN, NICHDNIH Librarians provide virtual support to the NIH Community through trainings, reference services, and more.Senior r adiologist A h m e d G h a r i b at the National Institute ofDiabetes and Digestive and Kidney Diseases is a timepiece connoisseur. He had an idea:What if the popular NATO watch band—a clever nylon strap and buckle of militaryorigin—could be adapted for use in magnetic resonance imaging (MRI)? He envisionedthe utilitarian design could be used to secure coils (specialized pieces that help the MRIscanner gather images of a specific body part) to larger patients or to irregularly shapedtesting devices called phantoms that act as a stand-in for human tissue. Gharib took hisconcept to the NIH Library, where the Tech Hub team used their 3D printer to builda supersized version of the NATO buckle. Gharib’s group has continued to work withthe library.“They are an outstanding service,” he said. “They go out of their way to be helpful.”His branch has since created custom paddings to optimize liver coils that are being usedCONTINUED ON PAGE 12CONTENTSFEATURES 1 Tackling Difficult Problems in Women’s Health 1 Beyond the Books: NIHLibrary 10 COVID-19 Timeline (Nov.-Dec.) 14 Dissecting the Causes of Health Disparities:Michele Evans 22 Obits 2021DEPARTMENTS 2 DDIR: My Time As DDIR 3 SIG Beat: Trans-NIH Gene Therapy 4 Training: Making Social Connections 5, 21 News Briefs: Larry Tabak Is NIH Acting Director;President Biden Announces New COVID-19 Plan 6 News You Can Use: Construction Updates 8 Research Briefs 15 NIH History: Where Did All the Acne Go? 18 Colleagues: RecentlyTenured 21 Abbreviations 24 Photographic Moment: Bone Growth Near a Fracture
FROM THE DEPUTY DIRECTOR FOR INTRAMURAL RESEARCHMy Time as Deputy Director for IntramuralResearch: The Early YearsBY MICHAEL GOTTESMAN, DDIROn July 15, 2021, NIH DirectorFrancis Collins announced my decisionthat it was time to step aside as the deputydirector for intramural research (DDIR)and make way for new leadership. Thisdecision was made after considerable selfreflection and with the desire to do whatI felt was best for the NIH intramuralprogram (IRP), which I truly believerepresents the epitome of biomedicalresearch excellence. I will remain as DDIRuntil a new IRP leader is in place. ThenI will return full time to the lab, where Iwill continue as the chief of the Laboratoryof Cell Biology in the National CancerInstitute’s Center for Cancer Research.I’ve had a lot of time to think about thenearly 30 years that I’ve served as the DDIR.My philosophy of science management hasled to important changes while preservingthe IRP’s basic conceptual underpinnings—that long-term, stable support of a diversegroup of talented scientists is a formulafor the extraordinary innovation andachievements of the IRP.My willingness to take on responsibilityfor the IRP grew out of my involvement asco-chair of the NIH committee respondingto a charge from Congress to review the“role, size, and cost” of the IRP. In 1992,Acting NIH Director Ruth Kirschsteinasked me to take on this responsibilityshortly after I had stepped down as actingdirector of the National Center for HumanGenome Research (now known as theNational Human Genome ResearchInstitute). The NIH committee workedwith an external committee chaired byGail Cassell (University of Alabama at2THE NIH CATALYST JANUARY–FEBRUARY 2022Birmingham) and Paul Marks (MemorialSloan Kettering Cancer Center), whichproduced a report that has been a blueprintfor the current architecture of the IRP. Myreward for this involvement with the MarksCassell report was to be asked by then–NIH Director Harold Varmus to becomeacting DDIR in 1993. I became DDIR thefollowing year after a search process.The report expands on the congressionalconcerns that led to the review of the IRP.To quote: “The challenge of ‘reinventing’the IRP requires that NIH rethink someof its practices regarding: 1) NIH-wideappointment and promotion of scientists;2) recruitment and retention of outstandingscientists; 3) invigorating postdoctoraltraining programs that transcend institutelines; 4) use of patient and research facilitiesin the Clinical Center; 5) instituting efficientmanagement and review practices that aremore responsive to the needs of the researchenterprise; and 6) exploring opportunities forincreased collaboration with the extramuralcommunity, including industrial andacademic laboratories.”An ideal research environment is avery delicate flower that must be cultivatedand can easily be damaged. Successfulresearch institutions are able to balancethe needs of many different personalitiesand talents with regulatory considerationsand a healthy interaction between localand central interests. The environmentfor creative science requires adequateresources, opportunities for collaboration,a shared mission, and a diversity of ideas,backgrounds, and scientific orientationsmade available to a group of talented, diversescientists who are eager to take advantage ofthis nurturing environment. I have alwaysviewed my job as encouraging the finerimpulses of our scientists, discouraging theless productive inclinations, and exercisingmy power to convene various groups withshared interests. I have helped to makematches between scientists and betweenthem and their research-resource needs. Ihave truly enjoyed serving as a convenor,matchmaker, and good listener, perhaps mymost valuable “powers,” since I do not havedirect supervisory authority over most of thescientists at the NIH.A major concern raised in the reportwas the need for NIH to continue to attractthe most diverse and talented scientists andsustain their careers in the IRP. Very earlyon, we established a tenure-track systemat the NIH and a process for recruiting,reviewing, and rewarding excellence (theBoards of Scientific Counselors reviewprocess and the tenure process). We hada legacy of outstanding scientists whocollaborated with our PIs and were essentialfor support and progress in our laboratories.They became staff scientists who now makeup the largest population of intramuralprofessionals. A system has been developedfor their recruitment and review.For our trainees, I wanted to assure acontinuity of opportunities—from highschool students to postdoctoral fellows—inthe IRP. Over the years we have built theOffice of Intramural Training and Education(very ably led by Sharon Milgram), whichworks with training directors in each of ourinstitutes and centers (ICs). In particular,I was directly involved in the formation of
.THE SIG BEATNEWS FROM AND ABOUT THE SCIENTIFIC INTEREST GROUPSNEW SIG: Trans-NIH Gene TherapyScientific Interest Groupthe postbac program; the NIH Academyfor postbacs interested in health-disparitiesresearch; the Undergraduate ScholarshipProgram for undergraduates from diversebackgrounds; the NIH Academy forpostbacs interested in health-disparitiesresearch; the Graduate Partnership Programfor graduate students; and various time-offprograms for medical students to learn aboutbiomedical research (the NIH-HowardHughes Medical Institute program and itssuccessors, the Clinical Research TrainingProgram and the Medical ResearchScholars Program). A student can enterthis continuum at any point and leave andre-enter as career aspirations dictate. In fact,some of our current PIs started at NIH ashigh school and college students.None of this could have beenaccomplished without a dedicated,scientifically adept senior staff in the Officeof Intramural Research (OIR), includingmany volunteers from the ICs, talented andhard-working directors of OIR programsand their staffs, and the strong support of thescientific and clinical directors and leadershipin the Office of the NIH Director and ineach of our ICs. We are very fortunate atthe NIH to have such capable leadership atall levels and in all institutes.In the next insta l lment of myruminations on the past 30 years of theIRP’s history, I will consider researchresource requirements, the reinvigorationof the Clinical Center and clinicalresearch programs at the NIH, technologytransfer developments, more recentchanges in our IRP program, and whatthe future may hold.The Tr a ns-NIH Gene Ther a pyScientific Interest Group (GRx SIG)was developed to strengthen crossdisciplinary gene-therapy research atNIH. The diversity of gene therapiesdictated the need to establish the GeneTherapy SIG to promote synergy acrossthe intramural research program (IRP).For example, the broad clinical areasof interest are rare diseases, pediatricdiseases, neurological diseases, infectiousdiseases, metabolic diseases, and cancer.Approaches and technologies includeantisense oligonucleotides; adenoassociated vectors and lentiviral vectors;small-interfering RNAs; and gene-,transcript-, and base-editing technologies.The translational and regulatory aspectsof gene therapy span the followingareas of interest: target identification,preclinical research and investigationalnew-drugs-directed studies (includingpharmacokinetics, pharmacodynamics,toxicology, and safety pharmacology),formulation and manufacturing, clinicaltrials, bioethics, and regulatory affairs.The goals of the GRx SIG are to 1)provide leadership, vision, and supportto promote gene-therapy research anddevelopment within the IRP; 2) shareknowledge about gene-therapy researchacross institutions, disciplines, and NIHinstitutes and centers (ICs); 3) collect,evaluate, and disseminate resources andopportunities for gene-therapy researchand development at NIH; 4) promoteinteractions, collaborations, and mentorshipamong intramural scientists and clinicians,and with extramural academic and industryresearchers; and 5) establish and implementa cohesive roadmap for gene-therapyresearch at NIH.The GR x SIG members includeprogram officers, program directors, andintramural investigators from differentICs. SIG activities will be coordinatedby a steering committee that oversees theorganization of meetings and educationalofferings on developing and applying genetherapy within NIH. Extramural academicand industry researchers may be invited toattend as guests. A combination of face-toface meetings and remote webinars will beheld, featuring guest speakers to provideperspective, comments, and expert feedback.The steering committee will communicatethe Gene Therapy SIG recommendationsand suggestions to the Gene TherapyTaskforce and vice versa. Meetings willbe held monthly (days and times to bedetermined).To receive e-mail notices of meetingsand how to attend, please subscribe to theGene Therapy LISTSERV at https://list.nih.gov/cgi-bin/wa.exe?A0 genetherapy-sig and click on the “Subscribeor Unsubscribe” link in the right sidebar.For more information and a schedule ofmeetings, visit the Gene Therapy SIG webpage nterest-group) or contact the chairof the Gene Therapy SIG, Bryan Traynor(bryan.traynor@nih.gov), or advisors AviNath (NINDS), Donald Lo (NCATS),and Carsten Bönnemann (NINDS).For a full lists of scientific interest groups, goto .gov/catalyst3
THE TRAINING PAGEFrom the Fellows CommitteeMaking Social Connections During COVID-19BY ALISON JANE MARTINGANO, NHGRILike many others, I started mypostdoctoral training at NIH during theCOVID-19 pandemic. I arrived in August2020, after almost all NIH employees,contractors, and trainees were assignedto mandatory telework (beginning inMarch 2020). In June 2020, those whosecould not work remotely were allowedto return to the labs. But the return waslimited. Capacity limitations to ensuresafe distancing meant that most traineesworked only part-time or in shifts.Trainees like myself, who can teleworkeffectively, are still working entirelyremotely.All of these changes, while necessaryfor ensuring employee and trainee safety,serve to make socializing with colleaguesdifficult. One trainee, who chose to remainanonymous, shared with me that “I quiteliterally haven’t spoken to another postdoc”since starting in August 2020.Most trainee events are held onlinenowadays including career and professionaldevelopment activities, wellness webinars,and meetings of trainee groups as wellas research symposiums and awardsceremonies. For many of these virtual venues,cameras-off has become the accepted normso you often don’t get to see the participants.In addition, there are few opportunities forthe kind of informal chitchat that mightnaturally occur at in-person gatherings.Zoom webinar formats usually donot allow for any audience interaction.Participants are held in virtual waiting roomsbefore events start and are unceremoniouslykicked out when the presenter is finished.These types of arrangements severely limitthe opportunities trainees have to socialize.Mallory Smith, a trainee in the NationalInstitute of Child Health and HumanDevelopment, put it simply: “You could4THE NIH CATALYST JANUARY–FEBRUARY 2022reach out via email afterwards, but frankly,you’re not very likely to do that.”Having social support is, unsurprisingly,a predictor of happiness and productivityat work. A survey of 522 remote workersduring COVID-19 found that more socialsupport people have, the less likely they areto procrastinate and feel lonely (Appl Psychol70:16–59, 2020).I asked several trainees to describe thesuccessful social-connection strategies theirinstitutes and centers (ICs) were using. Theysaid that making connections was easier, anddeeper conversations possible, when smallvirtual working groups shared a commoninterest and met regularly to write policydocuments or organize events. Some ICshosted outdoor activities such as hikesin which people break off naturally intoconversational pairs. I personally foundmeaningful connections at a virtual weeklysupport group for women scientists run bythe Office of Intramural Training andEducation (OITE), where I found empathyand encouragement in abundance.Dedicated social events held virtuallywere the least likely to generate meaningfulconnections. Trainees reported being morelikely to find deep connections at events notdeliberately designed for socializing, butwhere socializing was possible nonetheless.One of the problems with dedicatedsocial events is that they are often filledwith small talk rather than substantialconversations. How many of us internallygroan when asked to “go around andintroduce ourselves”? To deepen socialconnections, psychologists recommend weavoid small talk. Instead, we can try someof the closeness-generating questions—such as, “Before making a call, do you everrehearse what you’re going to say? Why?”,“What would constitute a perfect day foryou?”, or “For what in your life do youfeel most grateful?”—designed by socialpsychologist Arthur Aron (Pers Soc PsycholBull 23:363–377, 1997). He found thatasking and answering such questions witha stranger led to feelings of closeness thatapproached that of longtime friends.To encourage these kinds of deeperconversations in virtual settings, it is vitalthat trainees have access to private meetingspaces so they can feel free to speak honestlyand candidly. Trainees who work on campusmust still attend virtual trainings, but theymay not have any privacy. “Attending virtualmeetings while in a shared office makes itdifficult to make personal connections withthose on the call,” explained postdoctoralfellow Tiffany Zarrella (National CancerInstitute).While COVID-19 continues to upendour lives, we may have to accept that theway we socialize is different, but thatdoes not mean it has to be nonexistent.To f ind trainee events that mightinterest you, subscribe to the Fellow-LLISTSERV (https://list.nih.gov/cgibin/wa.exe?SUBED1 fellow-l&A 1) forofficial events, or contact the FELCOMsocial committee chair Nicholas Madianor the health and wellness committee chairTiffany Zarrella for other suggestions.More info on getting involved with OITEgroups can be found at https://www.training.nih.gov/wellness and .Alison Jane Martingan is a postdoctoral fellow inthe Immersive Stimulation Research Program,at the National Human Genome ResearchInstitute. Her research involves using virtualreality to evaluate how providers communicategenetic concepts and show empathy duringphysician-patient interactions.
NEWS BRIEFLawrence Tabak Named Acting Director of NIHWill Continue to Carry Out NIH’s Important InitiativesFROM THE OFFICE OF THE NIH DIRECTORActing NIH Director Lawrence Tabak.On December 20, 2021, L awrence A.Tabak, the principal deputy directorof the National Institutes of Health(NIH), began ser ving as the actingdirector of NIH. The previous NIHd i rec tor, Francis S. Col l ins, whostepped down from that position onDecember 19, was the longest-serving,presidentially appointed NIH director,having ser ved three U.S. presidentsover more than 12 years. Collins willcontinue to lead his research laboratoryat t h e Nat ion a l Hu m a n G e nom eResearch Institute.Taba k had ser ved as t he N IHprincipal deputy director and the deputyethics counselor since August 2010. Hepreviously served as the NIH actingprincipal deputy director in 2009, andprior to that as director of the NationalInstitute of Dental and CraniofacialResearch (2000–2010).Before joining NIH, Tabak was thesenior associate dean for research andprofessor of dentistry and biochemistryand biophysics in the School of Medicineand Dentistry at the University of Rochester(Rochester, New York). Tabak’s majorresearch focus has been on the structure,biosynthesis, and function of glycoproteins.He continues work in this area, maintainingan active research laboratory within theNIH intramural program in addition tohis administrative duties.A native of Brooklyn, New York,Tabak received his underg raduatedegree from City College of the CityUniversity of New York (New York), hisD.D.S. from Columbia University (NewYork), and both a Ph.D. and certificateof proficiency in endodontics from theUniversity of Buffalo (Buffalo, NewYork). A former NIH MERIT recipient,Tabak has received several honors andawards for his work including being anelected member the National Academyof Medicine (formerly the Institute ofMedicine) of the National Academies.“I am honored to assume the roleof the acting director of the NationalInstitutes of Health and lead the agencyduring this time of transition,” Tabakwrote in an email message to NIH staffon December 20, 2021. “Having servedat Dr. Collins’ side as the principaldeputy director since August 2010, Ihave been intimately involved in thescience, policies, and operations ofthe agency and will continue to carryout the important initiatives that Dr.Collins and I have built and fosteredtogether over the past 12 years . Dr.Collins’ singular focus has always beenfinding the best ways that NIH researchcan improve health, end suffering, andprovide hope for all people. As actingdirector of NIH, I will try to sustainthat legacy.”Other changes in the Office of theNIH Director:Tara A. Schwetz, who has been theNIH associate deputy director andalternate deputy ethics counselor atNIH since 2019 and recently did adetail to the White House Office ofScience and Technology Policy as theassistant director for biomedical scienceinitiatives, will serve as acting NIHprincipal deputy director. CourtneyF. Aklin, who was the senior advisorin the immediate Office of the Director,will resume her position as acting NIHassociate deputy director. John Burklow,formerly the NIH associate director forcommunications and public liaison, willcontinue as the acting chief of staff.To watch a farewell tribute to FrancisCollins, held on December 16,2 0 2 1 , g o t o h t t p s : // w w w . n i h . g o v atalyst5
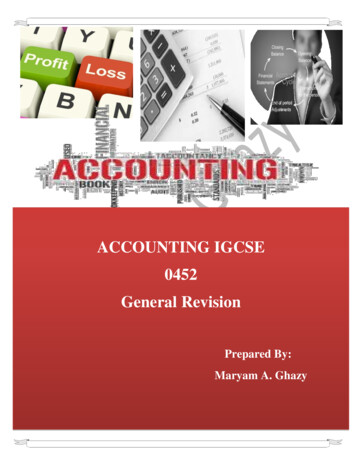
NEWS YOU CAN USEBuilding for the FutureNIH Construction Updates Facilities, Affects Parking and TrafficCREDIT: OFFICE OF RESEARCH FACILITIESBY MICHAEL TABASKO, ODConceptual rendering of the Surgery, Radiology, and Laboratory Medicine addition to the Clinical Center from thenorthwest view at Center Drive and the Old Georgetown Road entrance.Are you returning to the office orlab in 2022? Major construction projectsmay change how you navigate the day.A new multilevel parking (MLP) garagefor patients and employees is emergingalong Convent Drive in the northwestcorner of the Bethesda campus. AcrossSouth Drive, an expansion promisesto nearly double the size of the VaccineResearch Center (VRC). With fundingrecently appropriated by Congress, thelong-awaited Surgery, Radiology, andLaboratory Medicine (SRLM) additionwill begin to take shape on the west wingof the Clinical Center (CC). And out inHamilton, Montana, a new facility willboost Rocky Mountain Laboratories(RML) square footage by nearly 30%.During this biomedical infrastructuregrowth spurt, the Office of ResearchFacilities (ORF) has made easing the dayto-day impact on patients and employeesa top priority. A comprehensive strategyof mitigation measures aims to keep thechessboard of parking as well as vehicle6THE NIH CATALYST JANUARY–FEBRUARY 2022and pedestrian travel in motion. ORF,the Office of Research Services (ORS),and the CC are rolling out a collaborativecommunications campaign to keep the NIHcommunity informed. Over the comingmonths, be on the lookout for emails aswell as signage and posters that will directmovement throughout campus.Patient Parking Garage and Utility VaultWork on the new parking garage,MLP-14—located on the west side ofConvent Drive parallel to the CC—has beenunderway since January 2021. The structurewill shift parking from the aging garagelocated below the CC’s Ambulatory CareResearch Facility (ACRF), a nearly 40-yearold building that houses outpatient facilitiesand clinical laboratories. Beyond 2028, theold ACRF garage will eventually close. ORFis considering options to repurpose the space.Adjacent to MLP-14, upgraded electrical equipment will be installed in a newutility vault to power the growing hospitalcomplex once the new SRLM is completed.And protecting pedestrians from weatherand traffic, a tunnel under Convent Drivewill link to the CC.Construction on MLP-14 will wrapup later this year, but you won’t be able topark there just yet. Access will be restrictedbecause workers will use the garage andsurrounding area to stage materials for theSRLM project. The grand opening comesin summer 2028, when driveways off Centerand South Drives will make all 750 spacesavailable to patients, visitors, and staff.VRC expansionCranes and crews have begun preparingthe VRC for Building 40A: A six-story,80,000-square-foot addition that artfullyintegrates with the north side of the existingstructure via a central corridor and newlobby. On the north elevation, workers areinstalling a temporary weather barrier wallbehind the building’s exterior skin to shieldthe interior and allow research activity tocontinue unabated during construction. The20-year-old VRC is currently at capacity,and the new expansion will providededicated space for the future of criticalvaccine research. Supported by funds fromthe Coronavirus Aid, Relief, and EconomicSecurity (CARES) Act, ORF awarded theconstruction contract in November 2021.Completion is expected in the fall of 2024.SRLMA contemporary nine-story (with onebasement level) addition to the west wingof the CC will total 547,290 square feet,ensuring a future home for many of theadvanced services that make the CC aworld-class research facility. New space willhouse the General Radiology and ImagingServices, Department of PerioperativeMedicine, Department of LaboratoryMedicine, National Cancer Institutelabs, and other medical departments. Theambitious project will also renovate 82,150square feet of the existing CC and close
NEWS YOU CAN USE150 parking spaces in the ACRF garageand its west side P1 entrance. Constructionwill commence in February 2022 and lastuntil 2028. During this time, two roadswill be closed: 1) Center Drive from thegate at Old Georgetown Road to the frontof the Northwest Child Care Center (theparking lot to the child care center will stillbe accessible); and 2) Convent Drive northof the MLP-9 garage entrance.RML Comparative Medicine Center(RCMC)A sister project to the VRC addition, theRCMC is also supported by CARESAct funds and adds a three-story,120,000-square-foot vivarium, or animalfacility. Scientists at the National Instituteof Allergy and Infectious Diseases’ RMLcampus conduct vital research on emerginginfectious diseases. They often use animalmodels to better understand pathogens anddesign therapeutic studies for treatment andprevention. The new centralized animalreceiving and holding building replacesnearly 60-year-old facilities. It will supportall biosafety levels of research throughoutthe RML campus and scores of wideranging research projects including workon SARS-CoV-2.The RCMC will provide expandedcapabilities for studies with exotic species(such as bats), state-of-the-art imagingsystems, and a multispecies insectary tosupport the discovery of vector-bornediseases. Mosquitos and fleas could find anew home here, as well as ticks.Newly emerging and re-emerginginfectious diseases can trigger immediateneeds to shift research plans. Withthis in mind, each holding suite in theRCMC was designed for quick adaptationto accommodate different species.Construction is already underway, andimpacts to the scientific staff should beminimal. The project is scheduled to finishin spring 2024.PARKING AND TRAFFIC MITIGATION MEASURESClosures (dates are subject to change)Additions (dates are subject to change) February 2022: Center Drive will close from March 2022: A second gate arm installedthe gate at Old Georgetown Road to the frontat the Lincoln Drive entrance will double theof the Northwest Child Care Center (its parkinggate’s capacity for vehicles to enter campus.lot will still be accessible, however); ConventThe guard booth and exit lanes will beDrive alongside the CC (Building 10) will also berepositioned to improve pedestrian safety atclosed, but CC employees will still have accessthe intersection of Old Georgetown Road.to the MLP-9 parking garage. Both roads will March 2022: A temporary road from Southreopen in 2028 once the SRLM is complete.Drive (between Old Georgetown Road and February 2022: The P1 entrance (on the westConvent Drive) will access Building 60 andside) to the ACRF parking garage will close,the Safra Family Lodge. The one-lane road isbut the P3 entrance (on the east side) willdesigned to minimize environmental impactremain open for patients, visitors, and staff. Toand will include a small easement for oncomingaccess the P3 entrance, employee vehicles arevehicles to pull off.encouraged to enter campus on North Drive off March 2022: Secured parking attendantRockville Pike (where a new inspection stationbooths installed at Lot 10H (on the south sideis being built), and CC patients and visitors willof Building 10) will offer attendant-controlledcontinue to use the West Drive entrance andgeneral parking and recover 80 spaces lostinspection station. Remaining unchanged arefrom the ACRF garage.designated parking levels for patients and July 2022: Lot 18, a new visitor parking lot,visitors, general parking, and red-tag holders.will open on the south side of campus on thesite of Temporary Buildings 32 and 18 (whichChanges (dates are subject to change)are slated for demolition). Visitors who used Early 2022: The North Drive entrance willto park in Lot 4A (which will become the newbe open in the evening for exiting traffic onlyvalet parking lot for patients) will be able toto allow vehicles to exit right on Rockvillepark in Lot 18. A campus shuttle will serve thePike and access points east. ORF is currentlynew lot.working with the NIH police to finalize signage, August 2022: A remote inspection station willdetails, and timing.be set up along North Drive on parking lot 31B, February 2022: The MLP-9 garage, whichreplacing inspection capacity from the closedis now used by any NIH staff, will be only forACRF P1 entrance. Vehicles will receive a time-staff who work in the Clinical Center/Buildingstamped ticket before proceeding to the ACRF10 complex. Employees working in theP3 entrance on Memorial Drive.surrounding buildings may park in the MLP-6and MLP-8 garages. To minimize cross-campusYou can also check the “Campus Traffic andtraffic, all staff parking in MLP-6, -8, and -9Parking Changes” website for th
origin—could be adapted for use in magnetic resonance imaging (MRI)? He envisioned the utilitarian design could be used to secure coils (specialized pieces that help the MRI scanner gather images of a specific body part) to larger patients or to irregularly shaped testing devices