Transcription
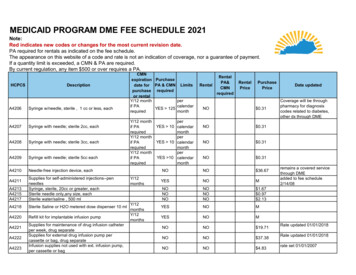
MEDICAID PROGRAM DME FEE SCHEDULE 2021Note:Red indicates new codes or changes for the most current revision date.PA required for rentals as indicated on the fee schedule.The appearance on this website of a code and rate is not an indication of coverage, nor a guarantee of payment.If a quantity limit is exceeded, a CMN & PA are required.By current regulation, any item 500 or over requires a PA.HCPCSDescriptionA4206Syringe w/needle, sterile , 1 cc or less, eachA4207Syringe with needle; sterile 2cc, eachA4208Syringe with needle; sterile 3cc, eachA4209Syringe with needle; sterile 5cc eachA4210Needle-free injection device, eachA4213A4215A4217Supplies for self-administered injections--penneedlesSyringe, sterile, 20cc or greater, eachSterile needle only,any size, eachSterile water/saline , 500 mlA4218Sterile Saline or H2O metered dose dispenser 10 mlA4220Refill kit for implantable infusion pumpA4211A4221A4222A4223Supplies for maintenance of drug infusion catheterper week, drug separateSupplies for external drug infusion pump percassette or bag, drug separateInfusion supplies not used with ext. infusion pump,per cassette or bagCMNexpiration Purchasedate for PA & CMN Limitspurchase requiredor rentalY/12 monthperif PAcalendarYES 125requiredmonthY/12 monthif PArequiredY/12 monthif PArequiredY/12 monthif alPA&CMNrequiredRentalPricePurchasePriceNO 0.31NO 0.31NO 0.31NO 0.31NONO 36.67YESNOMNONONONONONO 1.67 0.97 2.13YESNOMYESNOMNONO 19.71NONO 37.38NONO 4.83perYES 10 calendarmonthperYES 10 calendarmonthperYES 10 calendarmonthDate updatedCoverage will be throughpharmacy for diagnosiscodes related to diabetes,other dx through DMEremains a covered servicethrough DMEadded to fee schedule2/14/08Rate updated 01/01/2018Rate updated 01/01/2018rate set 01/01/2007
Medicaid Program DME Fee Schedule 2021HCPCSA4224A4225DescriptionSupplies for Maintance of insluin infusion catheter,per weekSupplies for external insulin infusion pump, syringetype cartridge, sterile, each)A4230Infusion set for external insulin pump, non needlecannula type eachA4231Infusion set for external insulin pump, needle typeeachA4232A4233A4234A4235A4236Syringe with needle for external insulin pump, sterile3ccReplacement battery , other than J cell homeglucose mon. eachReplacement battery , J cell, home glucose mon.eachReplacement battery, lithium, home glucose mon.eachReplacement battery, silver oxide, home glucosemon., eachCMNexpiration Purchasedate for PA & CMNpurchase requiredor urchasePriceNO 11.55Rate change effective7/1/2018;Rate change effective7/1/2018rate set 01/01/2007; qty limiteff. 5/1/09NO 7.33rate set 01/01/2007; qty limiteff. 5/1/09NONO 2.54NONO 0.51NONO 2.36NONO 1.00NONO 1.16NO 15.00NOMNO 8.32 19.71 2.64YES if PArequiredYES YES if PArequiredYES Y/12 monthif PArequiredY/12monthsY/12 monthif PArequired16 percalendarmonth16 percalendarmonthpercalendarmonthYES 2unitA4250Urine test or reagent strips or tablets 100 tablets orstrips 1 unitA4252Blood ketone test or reagent strip, eachA4253Blood glucose test or reag. strips blood glucosemonitor, 50 strips 1unitA4256Normal, low and high calibrator solution/chipsNONO 3.38A4258Spring-powered device for lancet, eachNONO 2.12A4259Lancets per box of 100 1 unit 100 lancetsNO 1.42A4261A4265Cervical Cap ContraceptiveParaffinNONO 1.39 3.24Y/12 monthif PArequiredDate updatedYESYES 4unitYES 2unitNONOpercalendarmonthpercalendarmonth2 of 95Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018Coverage will be throughpharmacy 10/5/10 and afterCoverage will be throughpharmacy 10/5/10 and afterCoverage will be throughpharmacy 10/5/10 and afterRate updated 01/01/2018Coverage will be throughpharmacy 10/5/10 and afterRate updated 01/01/2018Coverage will be throughpharmacy 10/5/10 and afterRate updated 01/01/2018Coverage will be throughpharmacy 10/5/10 and afterRate updated 01/01/2018
Medicaid Program DME Fee Schedule 4333A4334A4338DescriptionAdhesive skin support attachment for use withexternal breast prosthesis, eachIV delivery system disposable 50 ml or greater perhourCMNexpiration Purchasedate for PA & CMNpurchase requiredor rentalY/12monthsY/12IV delivery system disposable 5 ml or less per hourmonthsY/12 monthInsert tray w/o bag/cathif PArequiredY/12 monthInsertion tray w/o bag, with indwelling catheter, foleyif PAtype, 2-way latexrequiredCath w/o bag 2-way siliconeWith indwelling catheter, foley type, 3-way forcontinuous irrigationCath w/drainage 2-way latexCath w/drainage 2-way siliconeCath w/drainage 3-wayY/12 monthIrrigation trayif PArequiredY/12 monthIrrigation syringe, bulb or piston, eachif PArequiredMale external catheter w/integral collection chamber, Y/12 monthany type each, made of rubber or plastice, designed if PAto be washed & reused.requiredFem urinary collect dev cupFem urinary collect pouchStool collection pouchExternal drainage tubing for urinary leg bag orurostomy, eachLubricant, individual sterile, for insertion of urinarycatheter, eachUrinary catheter anchoring device, adhesive skinattachment, eachUrinary catheter anchoring device, leg strap, eachY/12 monthIndwelling catheter foley type, two-way latex withif PAcoating, PricePurchasePriceNONO 4.76YESNOMYESNOMNO 6.48NO 14.16NO 16.88NONO 17.67NONONONONONO 24.12 25.17 27.09NO 5.08NO 2.85NO 10.29NONONO 42.56 9.87 6.82NONO 3.04NONO 0.12NONO 2.10NONO 4.71NO 11.70YES 1YES 1NOYES 9YES 9YES monthpercalendarmonthpercalendarmonthperYES 31 calendarmonth3 of 95Date updated07/02/2007 limit change
Medicaid Program DME Fee Schedule 2021HCPCSDescriptionA4340Indwelling catheter, specialty type; coude,mushroom, wing, etc, eachA4344Catheter indwelling, foley type, 2 way, all silicone,eachA4346A4349A4351A4352Catheter indwelling, foley type, 3 way, forcontinuous irrigation, eachMale ext. catheter w or w/o adhesive, disposable,eachIntermittent urinary straight tip urine catheter, with orwithout coatingIntermittent urinary catheter, Coude tip, with orwithout coatingA4353Intermittent urinary cath sterile catheterization kitA4354Insertion tray with drainage bag but without catheterA4355Bladder irrigation tubing set through a three-wayindwelling foley catheter, eachA4356Ext ureth clmp or compr dvcA4357Bedside drainage bagA4358Urinary drainage bag, leg or abdomen, vinyl with orwithout tube with straps, eachA4359Urinary suspensory w/o leg bagA4361Ostomy face plateA4362Solid skin barrierA4363A4364Ostomy clamp, any type , eachAdhesive, liquid or equal, any type, per ounceCMNexpiration Purchasedate for PA & CMNpurchase requiredor rentalLimitsNOY/12 monthif PArequiredPurchasePrice 26.07NO 15.28NONO 18.69NONO 2.02NONO 1.47NONO 5.20YES 31percalendarmonth 6.67NONO 11.25NONO 8.50NO 43.52NO 7.86NO 5.39YES 4YES 14 per yearpercalendarmonthYES 66 per yearperYES 20 calendarmonthNONO4 of 95Date updated07/02/2007 limit change04/02/2007 limit changeNONOY/12 monthif PArequiredY/12 monthif PArequiredRentalPriceNOY/12permonths ifcalendarYES 124PA requiredmonthY/12 monthif PArequiredY/12 monthif PArequiredRentalRentalPA&CMNrequiredCMS DC1/07NO 18.37NO 3.17NONO 2.01 2.9339084rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007
Medicaid Program DME Fee Schedule 2021HCPCSA4366DescriptionOstomy vent, any type, eachA4367Ostomy 4391A4392A4393A4394A4395A4396Ostomy filterSkin barrier liquid per ozSkin barrier powder per ozOstomy Skin barrier solid 4x4 equivSkin barrier with flangeDrainable plastic pch w fcplDrainable rubber pch w fcpltDrainable plstic pch w/o fpDrainable rubber pch w/o fpUrinary plastic pouch w fcplUrinary plastic pouch w/o fpOstomy pouch, urinary, for use on faceplate, plastic,eachUrinary hvy plstc pch w/o fpUrinary rubber pouch w/o fpOstomy faceplt/silicone ringOst skn barrier sld ext wearOst clsd pouch w att st barrDrainable pch w ex wear barrDrainable pch w st wear barrDrainable pch ex wear convexUrinary pouch w ex wear barrUrinary pouch w st wear barrUrine pch w ex wear bar convOstomy pouch liq deodorant w/wo lubricantOstomy pouch solid deodorantOstomy belt with peristomal hernia supportA4397Irrigation supply sleeveA4381CMNexpiration Purchasedate for PA & CMN Limitspurchase requiredor rentalY/12permonths ifcalendarYES 1PA requiredmonthY/12months ifPA requiredY/12 monthif PArequiredYES ricePurchasePricerate change 8/1/2007NO 1.30rate change 8/1/2007NO 7.35NONONONONONONONONONONONONONONONONONONONONONO 0.26 2.42 3.65 4.18 6.28 17.18 47.58 4.29 30.75 15.02 37.33NONO NONONONONO 24.62 28.19 9.62 5.10 2.53 4.36 6.22 9.61 7.07 8.18 9.04 2.58 0.05 40.48NO 4.07YES 4percalendarmonth5 of 95Date updatedrate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007Rate updated 01/01/2018rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007
Medicaid Program DME Fee Schedule 2021HCPCSDescriptionA4398Ostomy irrigation bagA4399Ostomy irrig cone/cath w brsA4400Ostomy irrigation setA4402Lubricant price is per oz. 1 oz. 1 unitA4404Ostomy ring eachA4405Ostomy skin barrier, non-pectin based, paste, per ozA4406Ostomy skin barrier, pectin based, per ozOstomy skin barrier, with fl, extend wear, built inconvexity, 4x4 or Ostomy skin barrier, with fl, extend wear, built inconvexity, 4x4 or Ostomy skin barrier with flangeOstomy skin barrier, with fl, ex wear, without built inconvexity, 4x4 eaOstomy skin barrier, solid 4x4 or eq. ext. wear, builtin convexity, eachOstomy pouch, drainable, high otpt, use on barrierw/ o filter eachOstomy pouch, drainable, high otpt, use on barrierw/ fl with filter eaOstomy skin barrier, with fl, w/o built in convexity 4x4or Ostomy skin barrier, with fl, w/o built in convexity 4x4or Ostomy pouch, closed, w/barrier att. W/filter 1 pc.EachCMNexpirationdate forpurchaseor rentalY/12 monthif PArequiredY/12 monthif PArequiredY/12 monthif PArequiredY/12months ifPA requiredY/12 monthif PArequiredY/12months ifPA requiredPurchasePA & CMNrequiredYES 4YES 4Limits4 per year4 per yearpercalendarmonthpercalendarYES 4 ozmonthYES eNO 12.56NO 10.93NO 46.76NO 1.36NO 1.49NONO 3.40NONO 5.74NONO 8.76NONO 9.87NONO 6.22NONO 9.04NONO 5.10NONO 2.70NONO 5.50NONO 4.93NONO 6.00NO 2.75perYES 10 calendarmonthYES 60percalendarmonth6 of 95Date updatedrate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007 limit of4 oz. per calendar monthcorrected 2/6/08rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007rate change 8/1/2007
Medicaid Program DME Fee Schedule 2021A4417Ostomy pouch,closed, w/barrier att.,w/built-inconvexity, w/filter 1 pc, eachCMNexpiration Purchasedate for PA & CMN Limitspurchase requiredor rentalY/12permonths ifcalendarYES 60PA requiredmonthA4418Ostomy pouch,closed, w/o barrier att. W/filter 1 pc.EachY/12months ifPA requiredA4419Ostomy pouch, closed, use on barrier w/non-lockflange,w/filter 2pc, eachY/12months ifPA requiredA4420Ostomy pouch, closed, use on barrier with lockflange 2 pc, eachY/12months ifPA requiredHCPCSA4421A4423DescriptionOstomy supply, miscellaneousOstomy pouch closed, 2 pc. Locking flange, eachY/12months ifPA requiredY/12months ifPA requiredY/12months ifPA requiredA4424Ostomy pouch, drainable,w/barrier 1 pc, eachA4425Ostomy pouch drainable, non-locking flange 2 pceachY/12months ifPA requiredA4426Ostomy pouch, drainable, with locking flange, 2 pc.EachY/12months ifPA requiredA4427Ostomy pouch, drainable , use on barrier w/lockingflange, w/filter 2 pc, eachY/12months ifPA requiredYES 60YES 60YES YESYES 60YES 60YES 60YES 60YES percalendarmonthpercalendarmonth7 of ceNO 3.72NO 1.81NO 1.74NO 1.86NOMDate updatedrate change 8/1/2007NO 1.86rate change 8/1/2007NO 4.75rate change 8/1/2007NO 3.58rate change 8/1/2007NO 2.73rate change 8/1/2007NO 2.78
Medicaid Program DME Fee Schedule 2021A4428Otosmy pouch, urinary, extended wear faucet typetap, eachCMNexpiration Purchasedate for PA & CMN Limitspurchase requiredor rentalY/12permonths ifcalendarYES 60PA requiredmonthA4429Ostomy pouch, urinary w/convexity, faucet type tap,eachY/12months ifPA requiredA4430ostomy pouch urinary, ext. wear, convexity, faucettap, eachY/12months ifPA requiredA4431ostomy pouch, urinary, w/barrier, faucet type tap,w/valve ea.Y/12months ifPA requiredA4432ostomy pouch, urinary, non-locking flange, faucettype, ea.Y/12months ifPA requiredHCPCSDescriptionA4433ostomy pouch, urinary, w/locking flange, ea.A4434ostomy pouch, urinary, w/locking flange, w/faucettype tap ea.A4435OSTOMY POUCH, DRAINABLE, HIGH OUTPUT,WITH EXTENDED WEAR BARRIER (ONE-PIECESYSTEM), WITH OR WITHOUT FILTER, EACHA4450A4452Tape, non-water proof, 18 sq inchesTape, water proof , 18 sq inchesA4455Adhesive remover per ounceA4456Adhesive remover, wipes, any type, eachY/12months ifPA requiredY/12months ifPA requiredY/12months ifPA requiredY/12months ifPA requiredYES 60YES 60YES 60YES 60YES 60YES 60YES ePurchasePricerate change 8/1/2007NO 6.51rate change 8/1/2007NO 8.25rate change 8/1/2007NO 8.52rate change 8/1/2007NO 6.22rate change 8/1/2007NO 3.59rate change 8/1/2007NO 3.34rate change 8/1/2007NO 3.76CMS ADDED 1/1/13NO 5.01NONONONO 0.09 0.36YES 32NO 1.16NONO 0.268 of 95Date updatedCMS added 1/1/10
Medicaid Program DME Fee Schedule 2021HCPCSDescriptionA4465Non elastic binder for extremityA4466Garment, belt, sleeve or other covering, elastic orsimilar stretchable material, any type, eachA4467Belt, strap, sleeve, garment, or covering, any type)A4481Tracheostoma filterMoisture exchanger, disposable, for use withinvasive mechanical ventilation, eachIncontinent garment any type, each NOCOVERAGE THROUGH DMENon-disposable underpads, all sizesElectrodes, apnea monitor, per pairLead wires, apnea monitor per pairConductive paste or gel for use with electrical deviceE.G. tensPessary, rubber, any typePessary, nonrubber, any typeVag Inser Rectal Control SysSlingsTENS suppl 2 lead per monthsleeve for intmt. Limb compression device, 2A4563A4565A4595CMNexpiration Purchasedate for PA & CMNpurchase requiredor OMNONONONOM 9.94 10.53NONO 5.22NONONoNONONONONONONO 16.82 45.57 128.34 4.35 10.34YESNOMYESNOMNONO 38.55NO 14.76NO 15.99NO 52.63NONO 174.26NONONONONONONONONONO 65.00 137.96 22.75 8.51 1.27NOA4608Transtracheal oxygen catheter, eachHeavy duty battery, Ventilator, replacement forpatient ownedBattery cablesBattery chargerHand-held PEFR meterBreathing circuitsFace tentNOA4612A4613A4614A4618A4619NO 0.37Oximeter probe ceNOA4605A4601RentalMY/12monthsY/12Lithium ion battery for non-prosthetic use, repl. Onlymonthstubing with integrated heat use with pos. airwaypressure deviceTracheal suction catheter, closed system, eachA4600LimitsRentalPA&CMNrequiredNO4 percalendarmonth9 of 95Date updated39402Deleted 1/1/17 CMS added1/1/10Added effective 1/1/2017added to fee schedule4/14/08Added effective 1/1/2017Rate updated 01/01/2018Effective 01/01/2019Rate updated 01/01/20183908439084Rate updated 01/01/201801/02/2007 rate changeEFFECTIVE 7/1/14rate change per CMSrate change per CMS
Medicaid Program DME Fee Schedule 2021HCPCSDescriptionA4623Tracheostomy inner cannulaA4624Tracheal suction tubeA4625Trach care kit for new trachA4626Tracheostomy cleaning r, bag or reservoir for inhalerOropharyngeal suction cathTracheostomy care kitRepl bat t.e.n.s. own by ptUnderarm crutch padHandgrip for cane etcRepl tip cane/crutch/walkerAlternating pressure padA4649Surgical Supply, MiscellaneousA4928Surgical Mask, per 20. If medically necessary, thisitem may be provided to beneficiaries withrespiratory infections and their caregivers withoutfirst seekingA5051Pouch clsd w barr attachedA5052Clsd ostomy pouch w/o barrA5053Clsd ostomy pouch faceplateA5054Clsd ostomy pouch w/flangeCMNexpiration Purchasedate for PA & CMN Limitspurchase requiredor rentalY/12 monthperYES 31 calendarif PArequiredmonthY/12 monthperYES 91 calendarif PArequiredmonthY/12 monthperYES 1 calendarif PArequiredmonthY/12 monthperYES 2 calendarif PArequiredmonthNONONONONONONONOY/12YESmonthsY/12 monthif PArequiredY/12 monthif PArequiredY/12 monthif PArequiredY/12 monthif PArequiredpercalendarmonthperYES 60 calendarmonthperYES 60 calendarmonthperYES 60 calendarmonthYES 6010 of ceNO 5.31NO 2.14NO 6.61NO 2.59NONONONONONONONO 38.00 3.58 4.42 5.98 4.89 3.01 1.67 49.45NOMDate updatedRate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018No PA but for diagnosedCOVID-19 patients and 12.00 caregivers onlyNO 1.86NO 1.35NO 1.41NO 1.42rate set 08/01/2007
Medicaid Program DME Fee Schedule 2021HCPCSDescriptionA5055Stoma capA50571 pc ost pou w built in conv.A5061Pouch drainable w barrier atA5062Drnble ostomy pouch w/o barrA5063Drain ostomy pouch w/flangeA5071urinary pouch w/barrierA5072urinary pouch w/o barrierA5073urinary pouch on barr w/flngA5081Continent stoma plugA5082Continent stoma catheterA5083Continent device, stoma absorptive cover forcontinent device, eachA5093Ostomy accessory convex inseA5102Bedside drain btl w/wo tubeA5105A5112urinary suspensory with leg bag w/wo tube eachurinary leg bagCMNexpiration Purchasedate for PA & CMN Limitspurchase requiredor rentalY/12 monthperYES 31 calendarif PArequiredmonthY/12 monthperYES 31 calendarif PArequiredmonthY/12 monthperYES 20 calendarif PArequiredmonthY/12 monthperYES 20 calendarif PArequiredmonthY/12 monthperYES 20 calendarif PArequiredmonthY/12 monthperYES 20 calendarif PArequiredmonthY/12 monthperYES 20 calendarif PArequiredmonthY/12 monthperYES 20 calendarif PAmonthrequiredY/12 monthperYES 31 calendarif PArequiredmonthY/12 monthperYES 1 calendarif PArequiredmonthNOY/12 monthif PArequiredY/12 monthif PArequiredperYES 10 calendarmonth4 per yearYES 4NONO11 of riceDate updated 1.37 10.66NO 3.70NO 2.12NO 2.29NO 4.15NO 3.36NO 3.04NO 2.97NO 9.64NO 0.50NO 1.86NO 21.53NONO 33.88 33.02EFFECTUVE 1/1/161/16/09 rate change from 2.58rate change 02/14/2007eff. DOS 8-1-08 and after.CMS description chg. 1/08
Medicaid Program DME Fee Schedule 2021A5113Latex leg strapA5114Foam/fabric leg strapA5120Skin barrier wipes or swabs , eachA5121Solid skin barrier 6x6A5122Solid skin barrier 8x8A5126Disk/foam pad or- adhesiveA5131Appliance cleanerA5200Percutaneous catheter anchorA5500Diabetic shoe for density insert, per shoeA5501Diabetic custom molded shoe, per shoeCMNexpiration Purchasedate for PA & CMNpurchase requiredor rentalNOY/12 monthYES 1if PArequiredNOY/12 monthYES 20if PArequiredY/12 monthYES 20if PArequiredY/12 monthYES 10if PArequiredY/12 monthYES 1if PArequiredNOYes 2 perY/12calendarmonthsyearY/12 monthYESA5503Diabetic shoe w/roller/rocker, per shoeY/12monthsA5504Diabetic shoe with wedge, per shoeY/12monthsA5505Diabetic shoe w/metatarsal bar, per shoeY/12monthsA5506Diabetic shoe w/offset heel, per shoeY/12monthsA5507Modification to diabetic shoeY/12monthsHCPCSDescriptionYes 2 percalendaryearYes 2 percalendaryearYes 2 percalendaryearYes 2 percalendaryearYes 2 h2 percalendaryear2 percalendaryear2 percalendaryear2 percalendaryear2 percalendaryear2 percalendaryear2 percalendaryear12 of ceDate updatedNO 3.81NO 7.24NO 0.20NO 7.12NO 12.26NO 1.07NO 15.11NO 10.78NO 55.72NO 167.13NO 24.79rate change 08/01/2007; PAremoved eff 8-1-10;NO 24.79rate change 08/01/2007; PAremoved eff 8-1-10;NO 24.79rate change 08/01/2007; PAremoved eff 8-1-10;NO 24.79rate change 08/01/2007; PAremoved eff 8-1-10;NO 24.79rate change 08/01/2007; PAremoved eff 8-1-10;rate change 01/02/2007rate change 08/01/2007; PAremoved eff 8-1-10;rate change 08/01/2007
Medicaid Program DME Fee Schedule 2021CMNexpiration PurchaseHCPCSDescriptionRentaldate for PA & CMN Limitspurchase requiredor rentalY/122 perFor diabetics only, deluxe feature of off the shelfA5508YESNOmonthscalendardepth-inlay or custom-molded shoe, per shoeyearFor diabetics only, direct formed, compressionY/122 perA5510YESNOmolded, without heat, mul density insert prefab, per monthscalendarshoeyearYes 6 per 6 per yearY/12A5512Diabetic only insert mult. Density direct formed, each monthsNOcalendaryearDiabetic only insert mult. Density custom formed,Y/126 per yearA5513YESNOeachmonthsY/126 per yearYESNOA5514Mult Den Insert Dir Carv/CammonthsCollagen based wound filler, dry form, per gram ofA6010NONOcollagenCollagen based wound filler, gel/paste, per gram ofNONOA6011collagenA6021Collagen drsg, size 16 sq inches or less, eachNONOCollagen drsg, more than 16 sq in but less than 48 orA6022NONOequal to 48 inchesY/12YESNOA6023Collagen drsg, more than 48 square inches, eachmonthsA6024Collagen drsg wound filler, per 6 inchesNONOA6154Wound pouch eachNONOA6196alginate dressing 16 sq in, eachNONOA6197alginate drsg 16 48 sq in, eachNONOA6203Composite drsg 16 sq in, eachNONOA6204Composite drsg 16 48 sq in, eachNONOA6207Contact layer 16 48 sq in, eachNONOA6209Foam drsg 16 sq in w/o bdr, eachNONOA6210Foam drg 16 48 sq in w/o b, eachNONOA6211Foam drg 48 sq in w/o brdr, eachNONOA6212Foam drg 16 sq in w/border, eachNONOA6214Foam drg 48 sq in w/border, eachNONOA6216Non-sterile gauze 16 sq in, eachNONONon-sterile gauze 16 sq in 48", w/o adhesiveA6217YESNOborder, eachA6219Gauze 16 sq in w/border, eachNONOA6220Gauze 16 48 sq in w/border, eachNONOA6222Gauze 16 in no w/sal w/o b, eachNONO13 of 95RentalPA&CMNrequiredRentalPricePurchasePrice 32.00 32.00 22.73Date updatedPA removed eff. 8-1-10PA removed eff. 8-1-10rate change 08/01/2007; PAremoved eff 8-1-10; 32.00 44.56Effective 01/01/2019 24.77 1.82 21.02 20.05 181.51 5.90 13.71 7.01 15.68 3.19 5.94 7.00 7.14 19.00 28.01 9.25 9.82 0.05M 0.91 2.46 2.0307/02/2007 limit removedadded to fee scheduleMarch 09
Medicaid Program DME Fee Schedule ion Purchasedate for PA & CMNpurchase requiredor alPricePurchasePriceA6410Gauze 16 48 no w/sal w/o b, eachGauze 48 in no w/sal w/o b, eachGauze 16 48 sq in watr/sal, eachGauze, hydrogel, 16 sq in or less, eachGauze, hydrogel, more than 16 but less than 48 sqin, eachGauze, hydrogel, more than 48 sq inches, eachHydrocolld drg 16 w/o bdr, eachHydrocolld drg 16 48 w/o b, eachHydrocolld drg 48 in w/o b, eachHydrocolld drg 16 in w/bdr, eachHydrocolld drg 16 48 w/bdr, eachHydrocolld drg filler paste, eachHydrocolloid drg filler dry, eachHydrogel drg 16 in w/o bdr, eachHydrogel drg 16 48 w/o bdr, eachHydrogel drg 48 in w/o bdr, eachHydrogel drg 16 in w/bdr, eachHydrogel drg 16 48 in w/b, eachHydrogel drg 48 sq in w/b, eachHydrogel drsg gel filler per fl. ozAbsorpt drg 16 sq in w/o b, eachAbsorpt drg 16 48 w/o bdr, eachAbsorpt drg 48 sq in w/o b, eachAbsorpt drg 16 sq in w/bdr, eachAbsorpt drg 16 48 in w/bdr, eachTransparent film 16 sq in, eachTransparent film 16 48 in, eachTransparent film 48 sq in, eachImpreg gauze no h20/sal/yard,Sterile gauze 16 sq in, eachSterile gauze 16 48 sq in, eachPacking strips, non-impregn, up to 2 inches in width,per lin ydEye pad, sterile, eachA6441Padding bandg. Non-elast. 3" and 5", per yardNONO 0.54A6442Conforming bandg. Non-sterile, width 3", per yardNONO NO 2.30 3.44 3.44 4.46NONO NONONONO 18.30 6.24 16.05 25.99 7.54 21.74 11.68 2.45 5.79 11.75 37.46 6.93 9.46 22.68 15.49 1.90 3.10 6.05 1.16 2.89 1.46 4.10 10.43 1.83 0.12 0.41NONO 1.50NONO 0.4114 of 95Date updatedadded 5/1/10
Medicaid Program DME Fee Schedule 2021HCPCSDescriptionA6443Conforming bandg. Non-sterile, widtth 3' and 5",per yardA6444A6445CMNexpiration Purchasedate for PA & CMNpurchase requiredor urchasePriceNONO 0.23Conforming bandg. Non-sterile, width 5", per yardNONO 0.45NONO 0.26NONO 0.33A6447A6448Conforming bandg. Sterile, width 3", per yardConforming bandg. Sterile, width 3" and 5", peryardConforming bandg. Sterile, width 5 ",per yardLt. Compression bandg. Width , 3", per yardNONONONO 0.54 0.93A6449Lt. Compression bandg. Width 3", 5" per yardNONO 1.40NONO 4.73NONO 0.49A6446A6453High compression bandg., width 3 " and 5", peryardSelf-adherent bandg. Width 3", per yardA6454Self-adherent bandg. Width 3" and 5", per yardNONO 0.62A6455Self-adherent bandg. Width 5", per yardZinc paste impregnated width 3" and 5", peryardTubular drsg. W or w/o elastic any width, per linearyd.NONO 1.11NONO 1.02NONO 6507A6509A6510A6511A6512A6513Compression burn garment, facial hood, customCompression burn garment, glove to wrist, customfabricatedCompression burn garment glove to elbow sleevecustomCompression burn garment glove to axilla, customfab., eachCompression burn garment, foot to thigh lengthcustom fab., eachCompression burn vest, custom fabricated, eachCompression burn garment, trunk incl. arms down toleg openings (leotard) custom fabricated, eachCompression burn garment, lower trunk including legopenings, custom, eachCompression burn garment NOCCompression burn mask, face and/or neck, plastic orequal, customY/6 monthsY/6monthsY/6 monthsY/6 monthsY/6 monthsY/6 monthsY/6 monthsY/6 monthsY/6 monthsY/6 months15 of 95Date updatedadded for DOS 4/1/09 andaftercode added 07/02/2007code added 4-1-08code effective as of 8/1/07code added 04/02/2007code added to fee schedule8/21/09code added 07/02/2007code added 07/02/2007code added 04/02/2007
Medicaid Program DME Fee Schedule 2021HCPCSA6530A6531A6532A6534DescriptionGradient compression stocking below knee, 1830mm Hg, eachGradient compression stocking below knee, 3040mmg Hg, eachGradient compression stocking below knee, 4050mmg Hg, eachGradient compression stocking, thigh length, 30-44mm Hg, eachA6545GRADIENT COMPRESSION WRAP, NON-ELASTIC,BELOW KNEE, 30-50 MM HG, EACHA6549Gradient compression stocking/sleeve, 020Drsg. Set for neg. pressure wound therapyDisposable canister for pumpNondisposable pump canisterTubing used w suction pumpNebulizer administration setDisposable nebulizer sml volNondisposable nebulizer setFiltered nebulizer admin setLg vol nebulizer disposableDisposable nebulizer prefillNebulizer reservoir bottleDisposable corrugated tubingNebulizer water collec devicDisposable compressor filterCompressor nondispos filterAerosol mask used w nebulizeNebulizer dome & mouthpieceNebulizer not used w oxygenWater, distilled, nebulizer, 1000 mlInterface Cough Stimulating DeviceA7027Comb. Oral/nasal mask, used with CPAP, eachA7028Oral cushion for A7027, replacement only, eachA7029nasal pillows for A7027, replacement only, eachCMNexpiration Purchasedate for PA & CMNpurchase requiredor riceNOMNO 38.94NOMNOM2 peryear/perleg ONONONONONONONONONONONONONONONONONONONONO 21.94 8.20 27.96 3.11 1.47 1.24 11.73 7.47 2.59 8.94 39.23 15.76 2.89 0.57 3.20 1.28 6.53 121.19 0.31 16.07YESNO 120.01YESNO 33.56YESNO 15.0016 of 95Date updatedcode added 8/30/07,clarification 9/08code added 8/30/07clarification 9/08code added 1/9/09 foreffective date of 6/1/08code added 12/07Code added 9/1/16code eff. 1/1/2010; added4/30/10Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2021Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2018Rate updated 01/01/2021Effective 1/1/2015CMS code addition 1/08Rate updated 01/01/2018CMS code addition 1/08Rate updated 01/01/2018CMS code addition 1/08Rate updated 01/01/2018
Medicaid Program DME Fee Schedule 2021HCPCSDescriptionA7030Full face mask used with positive airway pressuredevice, eachA7031Face mask interface, replacement for full face mask,eachA7032Replacement cushion for nasal application device,eachA7033Replacement pillows for nasal application device,eachA7034nasal Interface(mask or cannula type) used with posairway pressure device wi
MEDICAID PROGRAM DME FEE SCHEDULE 2021 Note: Red indicates new codes or changes for the most current revision date. PA required for rentals as indicated on the fee schedule. The appearance on this website of a code and rate is not an indication of coverage, nor a guarantee of payment. If a quantity limit is exceeded, a CMN & PA are required.