Transcription
Application for Adjudication of ClaimOCR form sample packetThis packet contains instructions on how to fill in Optical Character Recognition (OCR)forms, examples of forms and is in the order in which they should be filed with thedistrict office.Use the table below to help identify the forms that you need to complete when filing anapplication for adjudication of claim. The table also shows the order in which the formsshould be assembled. To help you find the correct document separator sheet, theproduct delivery unit, document type and document title are in brackets.In this packet, you will see examples as filed by the applicant attorney for injuredworker. If a lien claimant is filing the forms, then complete and submit the documentsidentified in this reference table.12345678910111213Name of formDocument cover sheetDocument separator sheetApplication for adjudication of claimDocument separator sheet for labor codesection 4906(g)[ADJ-LEGAL DOCS-4906(g)DECLARATION]All declarations pursuant to labor codesection 4906(g)Document separator sheet for fee disclosurestatement[ADJ-LEGAL DOCS-FEE DISCLOSURESTATEMENT]Fee disclosure statementDocument separator sheet for venueauthorization[ADJ-LEGAL DOCS-VENUEVERIFICATION]Venue authorizationDocument separator sheet for lien verification[ADJ-LEGAL DOCS-10770.5VERIFICATION]Lien verification §10770.5Document separator sheet for proof of service[ADJ-LEGAL DOCS-PROOF OF SERVICE]Proof of xxxxxxxxxxxxxxxDivision of Workers’ Compensationwww.dwc.ca.gov(800) 736-7401xxxx
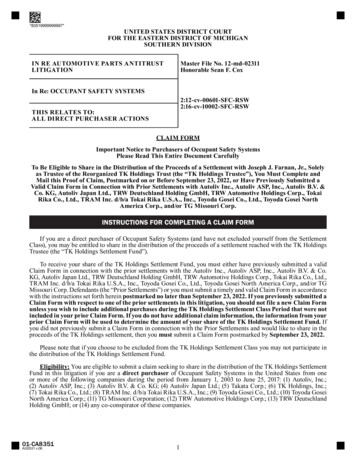
STATE OF CALIFORNIADWC DISTRICT OFFICEThis packet is an example of howto fill in forms and theorder in which they should be filedwith the district office.Is this a new case?Yes DOCUMENT COVER SHEETCompanion Cases ExistNoCHECK "YES" BOX ONLYDO NOT CHECK THIS BOXMore than 15 Companion Cases09/10/2008This example shows documentssubmitted by a representedinjured worker.Case Number 1Cumulative InjurySOCIAL SECURITYNUMBER IS NOTREQUIRED.SSN:Date:(MM/DD/YYYY)Specific InjuryNoDO NOT CHECK BOXESDATE YOU FILL OUT DOCUMENT COVER SHEETTHERE IS NO CASE NUMBER FORAPPLICATION FOR ADJUDICATIONLEAVE BLANK.YesWalkthrough11/02/2007(End Date: MM/DD/YYYY)(Start Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)SEE BODY PART NUMBERLIST ON PAGE 8IF CUMULATIVE INJURY MUST ENTER START AND END DATE USING MM/DD/YYYY.Body Part 1:420Body Part 3:Body Part 2:100Body Part 4:Other Body Parts:WHEN MORE THAN 5 BODY PARTS USE BODY PARTNUMBER 700 IN THIS FIELDPlease check unit to be filed on ( check only one box )ADJDEUSIFUEFINTRSUCompanion CasesSpecific InjuryCase Number 2Cumulative Injury(Start Date: MM/DD/YYYY)(End Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)Body Part 1:Body Part 3:Body Part 2:Body Part 4:Other Body Parts:DWC-CA form 10232.1 Rev. 7/2010 - Page 1 of 8Example
Specific InjuryCase Number 3Cumulative Injury(End Date: MM/DD/YYYY)(Start Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)Body Part 1:Body Part 3:Body Part 2:Body Part 4:Other Body Parts:Specific InjuryCase Number 4Cumulative Injury(Start Date: MM/DD/YYYY)(End Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)Body Part 1:Body Part 3:Body Part 2:Body Part 4:Do NOT print or submit blank page(s).Other Body Parts:Specific InjuryCase Number 5Cumulative Injury(Start Date: MM/DD/YYYY)(End Date: MM/DD/YYYY)(If Specific Injury, use the start date as the specific date of injury)Body Part 1:Body Part 3:Body Part 2:Body Part 4:Other Body Parts:DWC-CA form 10232.1 Rev. 11/2008- Page 2 of 8Example
District office codes for place of eAnaheimSanta AnaBakersfieldEurekaFresnoGoletaLos AngelesLong BeachMarina del linasSan BernardinoSan DiegoSan FranciscoSan JoseSan Luis ObispoSanta RosaStocktonVan NuysUse this document to complete forms, but do not file this document with your forms.DO NOT PRINT ORSUBMIT THIS PAGE.DWC-CA form 10232.1 Rev. 7/2010 - Page 7 of 8Example
Body Part Code ListThe body part codes listed below are used to complete forms that require the listing ofthe part of the body that is in issue. Please do not file this document with your 20430440450498Head - not specifiedBrainEar - not specifiedEar - externalEar - internal including hearingEye - including optic nerves and visionFace - not specifiedJaw - including chin and mandibleMouth - including lips, tongue, throat and tasteTeethNose - including nasal passages, sinus and smellFace - multiple parts any combination ofabove partsFace - forehead, cheeks, eyelidsScalpSkullHead - multiple injury any combination ofabove partsNeckUpper extremities - not specifiedArm - above wrist not specifiedArm - upper arm humerusArm - elbow head of radiusArm -forearm radius and ulnaArm - multiple parts any combination ofabove partsArm - not specifiedWristHand - not wrist or fingersFingersUpper extremities - multiple parts any combinationof above partsTrunk - not specifiedAbdomen - including internal organs and groinHerniaBack - including back muscles, spine and spinal cordChest - including ribs, breast bone and internalorgans of the chestHips - including pelvis, pelvic organs, tailbone,coccyx and buttocksShoulders - scapula and clavicleTrunk - use for side; multiple parts any combinationof above 810820830840841842850860870880999Lower extremities - not specifiedLegs - above ankles, not specifiedThigh femurKnee PatellaLower leg tibia and fibulaLeg - multiple parts any combination ofabove partsLeg - not specifiedAnkle malleolusFoot not ankle or toeToesLower extremities - multiple parts anycombination of above partsMultiple parts more than five major partsuse only in fifth position of listing of body partsBody system - not specificCirculatory system - heart -other than heartattack, blood, arteries,veins, etc.Circulatory system - Heart attackDigestive system - stomachExcretory system - kidneys, bladder, intestines,etc.Musculo-skeletal system - bones, joints, tendons,muscles, etc.Nervous system - not specifiedNervous system - stressNervous system - Psychiatric/psychRespiratory system - lungs, trachea, etc.Skin dermatitis, etc.Reproductive systemsOther body systemsUnclassified - insufficient information toidentify body partsDo NOT print or submit this pageExampleUse this document to complete forms, but do not file this document with your forms.DWC-CA form 10232.1 Rev. 11/2008 - Page 8 of 8
DOCUMENT SEPARATOR SHEETProduct Delivery UnitADJLEGAL DOCSDocument TypeDocument TitleAPPLICATION FOR ADJUDICATIONDocument DateAuthor04/16/2008DATE OF DOCUMENT FOLLOWINGDOCUMENT SEPARATOR SHEETMM/DD/YYYYUNIFORM ASSIGNED NAMEOffice Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2008 Page 1MM/DD/YYYYIF YOU ARE A CLAIMS ADMINISTRATOR,HEARING REPRESENTATIVE OFFICE OR LAWFIRM, USE YOUR OFFICE'S UNIFORMASSIGNED NAME. FOR ALL OTHERS ENTERYOUR NAME.
STATE OF CALIFORNIADIVISION OF WORKERS' COMPENSATIONWORKERS' COMPENSATION APPEALS BOARDAPPLICATION FOR ADJUDICATION OF CLAIMNO CASE NUMBER - LEAVE BLANKAmended ApplicationCase No.SSN (Numbers Only)SEE PAGE 6 FOR ADDITIONAL INSTRUCTIONS ON COMPLETING THIS FORM.Venue choice is based upon (Completion of this section is required) County of residence of employee (Labor Code section 5501.5(a)(1) or (d).)County where injury occurred (Labor Code section 5501.5(a)(2) or (d).)County of principal place of business of employee’s attorney (Labor Code section 5501.5(a)(3) or (d).)VNO3 DIGIT OFFICE CODE MUST BE IN COUNTY OF BOX CHECKED ABOVESelect 3 - Letter Office Code For Place/Venue of Hearing (From the Document Cover Sheet)Injured Worker (Completion of this section is required)JOHNMIFirst NameMILLERLast Name1234 WILLOW ROADStreet Address/PO Box (Please leave blank spaces between numbers, names or words)Street Address2/PO Box (Please leave blank spaces between numbers, names or words)International Address (Please leave blank spaces between numbers, names or words)CAVAN NUYSStateCity91401Zip CodeApplicant (If other than Injured Worker)Insurance CarrierEmployerLien ClaimantUSE THE UNIFORM ASSIGNED NAME AND ADDRESS FOR THE CLAIMSName (Please leaveADMINISTRATOR,blank spaces betweennames or words)IF YOUnumbers,ARE AN INSURANCECARRIER. USE YOUR NAME ANDADDRESS, IF YOU ARE AN EMPLOYER OR A LIEN CLAIMANT.Street Address/PO Box (Please leave blank spaces between numbers, names or words)Street Address2/PO Box (Please leave blank spaces between numbers, names or words)CityDWC/WCAB Form 1A (11/2008) - (Page 1)StateZip CodeWCAB1
Employer Information (Completion of this section is required)MUST CHECK ONE BOXInsuredSelf-InsuredLegally UninsuredUninsuredCOMPANY INJURED EMPLOYEE WORKED FOR AT TIME OF INJURYEmployer Name (Please leave blank spaces between numbers, names or words)COMPANY ADDRESS - MUST INCLUDE STREET ADDRESS OR PO BOX NUMBEREmployer Street Address/PO Box (Please leave blank spaces between numbers, names or words)MUST INCLUDE CITY, STATE AND ZIP CODECityStateZip CodeInsurance Carrier Information (If known and if applicable - include even if carrier is adjusted by claims administrator)NAME OF EMPLOYER'S INSURANCE CARRIERInsurance Carrier Name (Please leave blank spaces between numbers, names or words)INSURANCE CARRIER'S ADDRESS - MUST INCLUDE STREET ADDRESS OR PO BOX NUMBERInsurance Carrier Street Address/PO Box (Please leave blank spaces between numbers, names or words)MUST INCLUDE CITY, STATE AND ZIP CODEStateCityZip CodeClaims Administrator Information (If known and if applicable)UNIFORM ASSIGNED NAME OFCLAIMS ADMINISTRATORName (Please leave blank spaces between numbers, names or words)CLAIMS ADMINISTRATOR MEANS A SELF-ADMINISTEREDINSURER, A SELF ADMINISTERED SELF-INSUREDEMPLOYER, A SELF-ADMINISTERED JOINT POWERSAUTHORITY, A SELF-ADMINISTERED LEGALLY UNINSUREDOR A THIRD PARTY ADMINISTRATOR.CLAIMS ADMINISTRATOR ADDRESS - MUST USE THEONE IN UAN DATABASE.Street Address/PO Box (Please leave blank spaces between numbers, names or words)MUST INCLUDE CITY, STATE AND ZIP CODEStateCityZip CodeIT IS CLAIMED THAT (Complete all relevant information):1. The injured worker, bornMUST INCLUDEINJURED EMPLOYEE'SDATE OF BIRTH(OCCUPATION AT THE TIME OF INJURY)(DATE OF BIRTH: MM/DD/YYYY)(Choose only one)(Date of injury: MM/DD/YYYY)suffered a :cumulative injuryINJURY DATE/S MUST MATCH DATE/SINDICATED ON DOCUMENT COVERSHEET.DATE OF ACCIDENTspecific injuryThe injury occurred atJOB TITLE WHEN INJURED, while employed as a(n)which began on(Start Date: MM/DD/YYYY)and ended on(End Date: MM/DD/YYYY)MAY PUT "INJURED ON JOB SITE" OR COMPLETE ADDRESS WHERE INJURY OCCURED.Street Address/PO Box - Please leave blank spaces between numbers, names or wordsMUST INCLUDE CITY AND ZIPCODE.USE "CA" FOR STATE.CityDWC/WCAB Form 1A (11/2008) - (Page 2),CAStateZip Code.WCAB1
(State which parts of the body were injured)Body Part 1:420 BACKBody Part 2:100 HEADBODY PARTS MUST MATCH THE BODY PARTS INDICATED ONTHE DOCUMENT COVER SHEETIF MORE THAN 5 INJURED BODY PARTS,MAY ENTER 700 MULTIPLE IN OTHERBODY PARTS FIELD AND INCLUDEADDITIONAL BODY PARTS IN SECTION 2.Body Part 3:Body Part 4:Other BodyParts:2. The injury occurred as follows:(EXPLAIN WHAT THE WORKER WAS DOING AT THE TIME OF INJURY AND HOW THE INJURY OCCURED)3. Actual earnings at the time of injury:State value of tips, meals, lodging, or otheradvantages, regularly received MonthlyRate of Pay WeeklyMonthlyWeeklyHourlyHourlyDO NOT ENTER NONE,UNKNOWN OR N/A. IF YOUDON'T HAVE INFORMATION,LEAVE BLANK.Number of hours worked per week4. The injury caused disability as follows:Last day off work due to injury:MM/DD/YYYYFirst Period of Disability:Start DateSecond Period of Disability:Start DateMM/DD/YYYYEnd DateMM/DD/YYYYEnd DateMM/DD/YYYYMM/DD/YYYY5. Compensation:Compensation was paid:YesNoTotal paid:Weekly rate(s):Date of last payment:MM/DD/YYYY6. Has the worker received any unemployment insurance benefits and/or any unemployment compensationdisability benefits (state disability) since the date of injury?YesNoDWC/WCAB Form 1A (11/2008) - (Page 3)WCAB1
7. Medical treatment:Medical treatment was received:YesNoAll treatment was furnished by the Employer or Insurance Carrier:YesNoDate of last treatment:MM/DD/YYYYOther treatment was provided/paid by:(NAME OF PERSON OR AGENCY PROVIDING OR PAYING FOR MEDICAL CARE)YesDid Medi-Cal pay for any health care related to this claim?NoNames and addresses of doctor(s)/hospital(s)/clinic(s) that treated or examined for this injury, but that were notprovided or paid for by the employer or insurance carrier:Name of Doctor/Hospital/Clinic 1 (Please leave blank spaces between numbers, names or words)Name of Doctor/Hospital/Clinic 2 (Please leave blank spaces between numbers, names or words)8. Other cases have been filed for industrial injuries by this worker as follows:Case Number 1Case Number 3Case Number 2Case Number 49. This application is filed because of a disagreement regarding liability for:MUST SELECT AT LEAST ONE.Temporary disability indemnityPermanent disability indemnityReimbursement for medical expenseRehabilitationMedical treatmentSupplemental Job Displacement/Return to WorkCompensation at proper rateOther (Specify)DWC/WCAB Form 1A (11/2008) - (Page 4)WCAB1
Is the Applicant Represented? YesNoIf "No", applicant is to sign and date below.If "Yes", applicant’s representative is to complete the following and is to sign and date below.Law Firm/AttorneyNon-Attorney RepresentativeUNIFORM ASSIGNED NAME OF ATTORNEY FOR CLAIMS ADMINISTRATOR, INJURED WORKER OR LIENCLAIMANTLaw Firm or Company Name (If Applicable)Law Firm Number (If Applicable)Attorney/Representative First NameMIAttorney/Representative Last NameStreet Address/PO Box (Please leave blank spaces between numbers, names or words)CityStateMUST INCLUDE SIGNATURE WHEN APPLICANT ISREPRESENTEDAPPLICANT MUST SIGN WHEN NOTREPRESENTEDApplicant SignatureApplicant Attorney/Representative SignatureDated atDateCity04/16/2008MM/DD/YYYYDWC/WCAB Form 1A (11/2008) - (Page 5)Zip Code, CaliforniaDOCUMENT DATE ONDOCUMENT SEPARATORSHEETWCAB1
INSTRUCTIONSFILING AND SERVICE OF A DECLARATION OF READINESS IS A PREREQUISITE TO THE SETTING OF ACASE FOR HEARING.Effect of Filing ApplicationFiling of this application begins formal proceedings against the defendant(s) named in your application.Assistance in Filling Out ApplicationYou may request the assistance of an information and assistance officer of the Division of Workers' Compensation.Right to AttorneyYou may be represented by an attorney or agent, or you may represent yourself. The attorney's fee will be set by theWorkers' Compensation Appeals Board at the time the case is decided and is ordinarily payable out of youraward.Filling Out ApplicationFor "amended" applications, the venue choice must be the same as that specified on the original application, unless anorder changing venue has issued. A street or P.O. Box address within the United States must be entered for the placewhere the injury occurred. Therefore, if the injury did not occur at a fixed or identifiable location (such as a field, ahighway,or on water), or if the injury occurred outside of the United States, the employer's business address or anotherappropriate address must be specified; however, a short explanation regarding the place of injury may be appended tothe application. If medical treatment has been paid for by Medi-Cal, Medicare, group health insurance, or a private carrier,please specify.Service of DocumentsYour attorney or agent will serve all documents in accordance with Labor Code section 5501 and the Workers'Compensation Appeals Board's Rules of Practice and Procedure.If you have no attorney or agent, copies of this application will be served by the Workers' Compensation AppealsBoard on all parties. If you file any other document, you must mail or deliver a copy of the document to all parties in thecase.IMPORTANT!If any applicant is under 18 years of age, it will be necessary to file a Petition for Appointment of Guardian ad Litem.Forms for this purpose may be obtained at the district office of the Workers' Compensation Appeals Board, or bycalling the district office and requesting this form.DWC/WCAB Form 1A (11/2008) - (Page 6)WCAB1
DOCUMENT SEPARATOR SHEETProduct Delivery UnitADJLEGAL DOCSDocument Type4906(g) DECLARATIONDocument TitleDocument DateAuthorENTER DATE OF DOCUMENT FOLLOWINGDOCUMENT SEPARATOR SHEET04/16/2008MM/DD/YYYYUNIFORM ASSIGNED NAMEIF YOUYOU AREARE AA CLAIMSCLAIMS ADMINISTRATOR,ADMINISTRATOR,REPRESENTATIVEOR LAW FIRM,USEFIRM,YOURHEARING REPRESENTATIVEOR LAWUSE ICE'SFOROTHERS,ALL OTHER,ENTERYIOURNAME.ALLENTERYOURNAME.Office Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2008 Page 1MM/DD/YYYYExample
A Professional CorporationCOMPLIANCEWITH LABOR CODE§4906(g)EMPLOYEE:EMPLOYER:CASE NO/DATE OF INJURY:Pursuant to the requirements set forth in Labor Code §4906(g), I declare as follows:I have not violated Labor Code §139.3.I have not offered, delivered, received, or accepted any rebate, refund, commission,preference, patronage, dividend, discount, or other consideration, whether in the formof money or otherwise, as compensation or inducement for any referred examinationor evaluation.A photostatic copy of this declaration shall be as valid as the original.I declare under penalty of perjury under the laws of the State of California that theabove is true and correct.DATED: 4/16/08DATED:APPLICANT'S ATTORNEYExample
DOCUMENT SEPARATOR SHEETProduct Delivery UnitADJLEGAL DOCSDocument TypeDocument TitleFEE DISCLOSUREDocument Date04/16/2008DATE OF DOCUMENT FOLLOWINGDOCUMENT SEPARATOR SHEETMM/DD/YYYYLAW FIRM ONLY - USE YOURUNIFORM ASSIGNED NAMEAuthorUNIFORM ASSIGNED NAMEOffice Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2008 Page 1MM/DD/YYYYExample
State of CaliforniaDepartment of Industrial RelationsDivision of Workers’ CompensationFEE DISCLOSURE STATEMENTIf you choose to be represented by an attorney, your attorney’s fees will be deducted from yourbenefits. The fee will be approved by the Workers’ Compensation Appeals Board, withconsideration given to the: (1) responsibility assumed by the attorney; (2) care exercised inrepresenting you; (3) time involved; and, (4) results obtained.Attorney’s fees normally range from 9% to 12% ofthe benefits awarded. However a fee of 15% maybe charged if the case is complicated and timeconsuming. If your attorney has also represented youbefore the Rehabilitation Unit, there may also be a fee allowed for this representation.There are certain circumstances where your employer (or his/her insurer) may be liable to pay yourattorneys’ fees. For example, if employer disputes a permanent disability evaluation obtained whenyou were not represented by an attorney, your employer may, be liable for any attorney fees you incurbecause of the dispute.If at anytime you no longer wish to be represented by the attorney, you may withdraw fromrepresentation by notifying the attorney. If you withdraw from representation, the fee amount foundby a workers’ compensation judge to be the fair value of any work the attorney did in your case willbe deducted from your award.An Information and Assistance Officer may be able to answer your questions concerning your workers' compensationbenefits at no charge to you. He/She may be able to resolve your problems without the needfor litigation.Call this toll-free number 1-800-736-7401Employee’s SignatureDate: 9/16/08Employee’s NameAttorney’s SignatureDate:Attorney’s NameAddressPhone No,Any person who makes or causes to be made any knowingly false or fraudulent materialstatement or material representation for the purpose of obtaining or denying workers’compensation benefits or payments is guilty of felony.Example
DOCUMENT SEPARATOR SHEETTHIS IS AN EXAMPLE OF THE DOCUMENTSEPARATOR SHEET FOR VENUEAUTHORIZATIONProduct Delivery UnitADJDocument TypeLEGAL DOCSDocument TitleVENUE VERIFICATIONDocument DateAuthorENTER THE DATE OF THE VENUEAUTHORIZATION04/16/2008MM/DD/YYYYON VENUE AUTHORIZATION DOCUMENTSEPARATOR SHEET, LIST INJURED WORKERAS THE AUTHOR.JOHN SMITHOffice Use OnlyReceived DateDWC-CA form 10232.2 Rev. 7/2010 Page 1MM/DD/YYYYExample
VENUE AUTHORIZATIONI HEREBY AUTHORIZE MY WORKERS' COMPENSATION CASE(S) FOR INJURY(IES)DATEDTO BEFILED AT THEVANNUYSWORKERS' COMPENSATION APPEALS BOARD.DATED:4/16/2008APPLICANTDrive, SuiteCATEL:FAX:Example
DOCUMENT SEPARATOR SHEETProduct Delivery UnitADJLEGAL DOCSDocument TypeDocument TitlePROOF OF SERVICEDocument DateAuthor04/16/2008DATE OF DOCUMENT FOLLOWINGDOCUMENT SEPARATOR SHEETMM/DD/YYYYUNIFORM ASSIGNED NAMEIF YOU ARE A CLAIMSIFYOU ARE A ATIVE OR LAWREPRESENTATIVEOR LAW FIRM,FIRM USE YOUR UNIFORMUSEYOUR OFFICE'SUNIFORMASSIGNEDNAME. FORASSIGNEDNAME. FORALLUNREPRESENTEDINJUREDWORKERSAND OTHERSOTHERS,ENTERYOUR NAME.ENTER YOUR NAME.Office Use OnlyReceived DateDWC-CA form 10232.2 Rev. 11/2008 Page 1MM/DD/YYYYExample
Proof of ServiceI am at least 18 years of age, not a party to this action, and I am a resident of or employed in thecounty where the mailing took place.My business address is:On 04/16/2008 served a true copy of the following documents, along with supporting documents,described as: Application of adjudication of claim, 4906(g), fee disclosure statement and venue authorizationby enclosing them in a sealed envelope addressed to each of the parties named and at theaddresses set forth in the Party List, and placing each envelope for collection and mailing at thebusiness address herein following our ordinary business practices, with postage fully prepaid, orby other previously agreed-upon method of electronic service.I declare under penalty of perjury under the laws of the State of California that the foregoing istrue and correct.Dated:04/16/2008Declarant SignatureParty ListExample
Document separator sheet for lien verification [ADJ-LEGAL DOCS-10770.5 VERIFICATION] x : 11 Lien verification §10770.5 : x : 12 ; Document separator sheet for proof of service [ADJ-LEGAL DOCS-PROOF OF SERVICE] x : x : x : 13 Proof of service : x : x : x : Division of Workers' Compensation ; www.dwc.ca.gov (800) 736-7401 ;