Transcription
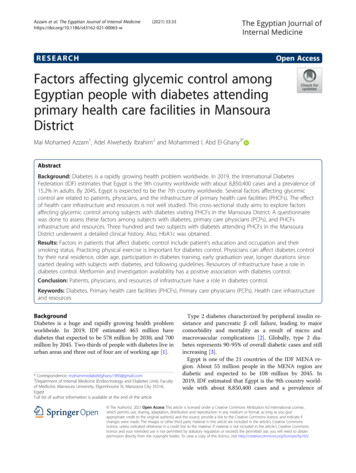
Mansoura Journal of Dentistry 2021;8(31):1-11.Efficacy of Locally Delivered Bifidobacterium Probiotic Gel as anAdjunctive Therapy in Periodontitis Patients (Clinical andMicrobiological Study) Dina R. Abuazab1, Una M. El-Shinnawi 2, Medhat A. El-Daker31. Master degree of Oral Medicine and Periodontology, Faculty of Dentistry, Mansoura University, Mansoura, Egypt.2. Professor of Oral Medicine ,Periodontology and Oral diagnosis Faculty of Dentistry, Galala University, Cairo, Egypt.3. Professor of Medical Microbiology and Immunology, Faculty of Medicine, Mansoura University, Mansoura, Egypt.Abstract:Objectives: This study evaluates the clinical and microbiological effect of Bifidobacterium probiotic gel as an adjunctive therapy toscaling and root planning (SRP) in chronic periodontitis patients and compering this effect with Chlorhexidine gel.Materials and Methods: Thirty chronic periodontitis patients (18 females, 12 males, aged between 30 and 50 years) were involved inthe study. They were classified into 3 groups randomly. 1 st group composed of 10 patients who received SRP associated with thesubgingival application of Bifidobacterium probiotic gel, 2 nd group composed of 10 patients who received SRP associated with thesubgingival application of Chlorhexidine gel and 3 rd group composed of 10 patients who received SRP only. Local drug delivery wasapplied once weekly for six weeks. All patients were evaluated clinically by measuring periodontal parameters (Plaque Index, GingivalIndex, Probing Pocket Depth and Clinical Attachment Level) , and microbiologically by culturing plaque samples anaerobically fordetection of total bacterial count, p.gingivalis & p.intermedia counts at baseline and six weeks after periodontal treatment.Results: All periodontal parameters (PI, GI, PPD and CAL), total bacterial count in addition to p.gingivalis & p.intermedia counts werereduced significantly after six weeks among all the groups. However by comparing in between groups there was significant difference inp.gingivalis & p.intermedia counts between groups 1&3 also between groups 2& 3.Conclusion: The local application of Bifidobacterium probiotic gel offers a promising therapeutic approach in periodontal treatment asadjunct to SRP.Keywords: Bifidobacterium probiotic, Chlorhexidine, Chronic Periodontitis, Local Drug Delivery.Introductioneriodonitis is a disease of the periodontiumcharacterized by the irreversible loss of connectivetissue attachment and supporting alveolar bone. Thisdestruction of the periodontium is a result ofinteractions between a complex of subgingival bacterialpopulation and specific host defense mechanisms. (1)Conventional periodontal treatment involves mechanicalsupra and subgingival debridement (Scaling and rootplanning) which considered as a gold standard treatmentmodality. (2) Although initially the number of pathogens canbe greatly reduced by (SRP), periodontal pathogens quicklyre-colonize the treated niches in the oral cavity. (3)Adjunctive use of local or systemic antimicrobials improvesthe outcome of periodontal therapy only temporarily. Thus,a life-long need for re-treatment arises, creating a serioussocio-economic problem. Additionally, increasing levels ofantibiotic resistant bacteria favour the development ofapproaches that do not rely on antibiotics. (3)Chlorhexidine remains the gold standard antimicrobialagents as it has a broad spectrum of antimicrobial activitythat play role in treatment of gingivitis and periodontitis.Also it has an anti-inflammatory action, inhibition of boneloss and promote the attachment of fibroblast to the rootsurface. Moreover a great effect on plaque accumulationand bleeding on probing. (4)P1Recently the use of beneficial bacteria has arisen as apromising concept in the management and treatment ofperiodontal diseases. (5) According to the World HealthOrganization, probiotics are live microorganisms that canconfer health benefits to the host when consumed inadequate amounts. (6)Probiotics have a proper scope in the field of periodontitisas they can reduce periodontopathogens, improveperiodontal clinical parameters, decrease the levels ofproinflammatory cytokines, and potentiate the effects ofSRP. (3)Probiotics, most commonly belong to the genera Lactobacillus and Bifidobacterium. (6) Bifidobacterium ispart of the human microbiota and presents a symbioticrelationship with the host. It is considered a potentialprobiotic as it possesses immunomodulatory andantimicrobial properties. (7-9)The knowledge regarding the benefits of Bifidobacteriumprobiotic in the management of chronic periodontitis islimited. Further studies should be conducted to confirm theoutcomes of this strain on both clinical and microbiologicalparameters, as well as to test new formulations of probioticsbesides the common lozenges.Dina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.1.2.Aim of the study:Evaluation the clinical and microbiological effect ofBifidobacterium probiotic gel as an adjunctive therapyto scaling and root planning (SRP) in chronicperiodontitis patients and compering this effect withChlorhexidine gel.Patients and Methods:3.1 patient selection:A total of 30 patients of both genders (18 females and 12males), aged between 30 and 50 years were selected fromthose attending the outpatient clinic of Oral Medicine andPeriodontology department, Faculty of Dentistry, MansouraUniversity. They were diagnosed as having moderatechronic periodontitis according to the criteria of theInternational Classification System for PeriodontalDiseases. Complete medical, dental histories andperiodontal charting were taken from all patients. The studywas approved by the internal Ethical Committee of Facultyof Dentistry, Mansoura University. All the participantsclearly understood the purpose and duration of the study,expected benefits and/or complications and agreed to enrollin the study and informed consent were obtained.3.2 Inclusion and Exclusion criteria:The inclusion criteria were age over 30 years, probingpocket depth (PPD) 4 mm and CAL 3-4mm with nohistory of antibiotic or periodontal therapy in the last 3months. The exclusion criteria were systemic conditionsthat could influence the progression of periodontitis ortreatment response (e.g. Diabetes Mellitus), Smoking,Pregnancy, long-term administration of anti-inflammatorymedications or usage of probiotics 6 months prior to thestudy.3.3 Patients Grouping :The selected patients weredivided into 3 groups as following:Group I (study group): Comprised of ten patientssuffering from moderate chronic periodontitis were treatedby scaling and root planning (SRP) followed by localdelivery of Bifidobacterium probiotic gel. Group II (studygroup): Comprised of ten patients suffering from moderatechronic periodontitis were treated by scaling and rootplanning (SRP) followed by local delivery of Chlorhexidinegel. Group III (control group): Comprised of ten patientssuffering from moderate chronic periodontitis were treatedby scaling and root planning (SRP) only.thoroughly dried then the gel was applied carefullysubgingivally and interproximally until excess gel wasobserved from the gingival margin, excess gel wasremoved with a cotton roll. Patients were alsoinstructed to avoid chewing hard or sticky foods,brushing near the gel treated site or using inter-dentalaids at the day of application. Gel application wasperformed once a week for six weeks. Bifidobacterium probiotic gel Preparation:Bacterial strain : Bifidobacterium bifidum, EMCC #: 1334,Designation: DSM 20082, E 319f, JCM 12, isolated fromintestine of adults and supplied as actively growingcultures. It was bought from Biological Resources Center(Cairo MIRCEN), Faculty of Agriculture, Ain ShamsUniversity, P.Box 68, Hadayek Shoubra, Cairo 11241,Egypt.The viability of the test strain was tested by monitoringtheir growth on Trypticase Soy Yeast Extract agar (TSYE)(Oxoid) under anerobic conditions prepared by Dr. M.Abdelmesih, (Microbilogy, F. Medicine, MansouraUniversity)Gel was prepared in November 12, 2019 (Liver ResearchLab-FAB-Lab, Pharmacognosy Department, Faculty ofPharmacy), Mansoura University, Egypt. Oral gel wasprepared using mucoadhesive polymer to achieveacceptable mucoadhesion so that the medication remains onthe spot of application for a longer time.3.5 Clinical Assessment: Clinical parameters wererecorded at the baseline and after 6 weeks oftreatment including: Plaque Index (PI), GingivalIndex (GI),Pocket Probing Depth (PPD) and ClinicalAttachment Level (CAL)3.6 Microbiological Assessment: Plaque samples weretaken at the baseline and after 6 weeks of thetreatment. Samples were cultured quantitatively onthree bacterial media; first, brain heart infusion agar(Oxoid). Second, brain heart infusion agarsupplemented with 5.0 ug/ml hemin for detection ofPorphyromonas gingivalis. Third, Blood agarcontaining 10 mg sulphamethoxazole/L and 0.5 mgtrimethoprim/L for detection of Prevotella intermedia.Inoculated plates were subjected to anaerobiccondition using an anaerobic jar and anaerobic gaspacks (Oxoid) with catalyst and then incubated at 37C for 5 days.3.4 Periodontal treatment: Treatment phase:A. Full mouth scaling and root planning performedusing hand instruments and ultrasonic scaler underlocal anesthesia when necessary for all groups.B. Application of Bifidobacterium probiotic gel forgroup 1 and Chlorhexidine gel for group 2 with thesame procedure by the following way: The selectedsites were isolated carefully with cotton rolls and23.7 Statistical analysis and data interpretation: Datawere fed to the computer and analyzed using IBMSPSS Corp. Released 2013. IBM SPSS Statistics forWindows, Version 22.0. Armonk, NY: IBM Corp.Qualitative data were described using number andpercent. Quantitative data were described usingmedian (minimum and maximum) for non-parametricdata and mean, standard deviation for parametric dataafter testing normality using Shapiro–Wilk test.Dina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.Significance of the obtained results was judged at the(0.05) level. Qualitative data: Monte Carlo test ascorrection for Chi-Square test when more than 25% ofcells have count less than 5 in tables ( 2*2).Quantitative data between groups:Parametrictests:One Way ANOVA test was used to compare morethan 2 independent groups with Post Hoc Tukey testto detect pair-wise comparison Paired t test to compare between 2 studied periods.Non Parametric tests: Kruskal Wallis test was used to compare more than 2independent groups with Mann Whitney U test todetect pair-wise comparison Wilcoxon signed Rank test to compare between 2studied periods.4 Results:Regarding Plaque Index pre-treatment; there was nostatistically significant difference between studied groupswith mean Plaque index was 2.34, 2.49 & 2.33 for groups1, 2 & 3, respectively. Post-treatment Plaque index showedstatistically significant difference between groups 1&2only. Mean Plaque index post-treatment was 0.766, 0.889& 0.826 for groups 1, 2 & 3, respectively. Comparing preand post treatment values of plaque index demonstrated astatistically significant lower mean values among allstudied groups (p 0.001). Table (1)Regarding Gingival Index pre-treatment; there was nostatistically significant difference between studied groupswith mean gingival index was 1.84, 1.815 & 1.83 forgroups 1, 2 & 3, respectively. Post-treatment gingival indexshowed non-statistically significant difference betweenstudied groups. Mean gingival index post-treatment was0.356, 0.341 & 0.353 for groups 1, 2 & 3, respectively.Comparing pre-and post-treatment values of gingival indexdemonstrated a statistically significant lower mean valuesamong all studied groups (p 0.001). Table (1)Regarding Pocket Probing Depth pre-treatment; there wasno statistically significant difference between studiedgroups with mean PPD was 3.29, 3.06& 3.28 for groups 1,2 & 3, respectively. Post-treatment PPD showed nonstatistically significant difference between studied groups.Mean PPD post-treatment was 2.02, 1.97 & 1.92 forgroups 1, 2 & 3, respectively. Comparing pre-and posttreatment values of PPD illustrated a statistically significantlower mean values among all studied groups (p 0.001).Table (1)Regarding Clinical Attachment Level pre-treatment; therewas no statistically significant difference between studiedgroups with mean CAL was 2.79, 2.57 & 2.78 for groups 1,2 & 3, respectively. Post-treatment CAL showed nonstatistically significant difference between studied groups.Mean CAL post-treatment was 1.87, 1.96 & 2.25 forgroups 1, 2 & 3, respectively. Comparing pre-and posttreatment values of CAL showed a statistically significantlower mean values among all studied groups (p 0.001).Table (1)3The mean value of total bacterial count was lowest amonggroup 2 followed by group 1 & group 3 pre-treatmentwithout significant difference between them with meanbacterial count was 884 , 928.5 & 965 , respectively.Similarly , no statistically significant difference of posttreatment bacterial count between studied groups with thelowest mean was detected among group 1 (505) , followedby group 2(581) and group 3(612). Table (2)Mean values of Prevotella intermedia count pre-treatmenthad no statistically significant difference between studiedgroups before treatment; while there was statisticallysignificant difference between studied groups aftertreatment. Mean P.intermedia count after treatment waslowest among group 1 followed by group 2 and the highestwas among group 3 (11, 12 &19 respectively). Comparingpre and post treatment P.intermedia count illustratedstatistically significant difference between groups (1, 3) &(2, 3) without statistically significant difference betweengroups (1, 2). Table (2)Mean values of Porphyromonas gingivalis countpre- treatment had no statistically significant differencebetween studied groups before treatment. However, therewas statistically significant difference between studiedgroups after treatment. Mean P. gingivalis count aftertreatment was lowest among groups 1, 2 &3 (7, 9&17respectively) and the highest was among group 3 (17).Comparing pre and post treatment P. gingivalis countillustrated statistically significant difference betweengroups (1, 3) & (2, 3) without statistically significantdifference between groups (1, 2). Table (2)5 Discussion:Periodontal diseases result from the complex interactionbetween pathogenic bacteria and the host immunoinflammatory responses. (10)Previous studies have shown that the local route of drugdelivery can attain 100-fold higher concentrations of anantimicrobial agent in subgingival sites compared with asystemic drug regimen. The advantages of local drugdelivery are high concentrations at the target site withreduced dosage, fewer applications, and high patientacceptability. (11)In this connection a new approach consists of modulatingthe composition of the newly formed oral biofilms throughthe administration of probiotics concomitantly to scalingand root planning, Probiotics as living micro-organismconfer health benefit on the host when administered insufficient doses, probiotics were useful in reducing gingivalinflammation and decreasing red & orange bacterialcomplexes count.(12)To the best of our knowledge we were among the first toprepare Bifidobacterium probiotic in the form of gel insteadof other available strains (lactobacillus) and forms(lozenges and chewing gums) as the application of gel wasfound to provide a long stay in the oral cavity ,possessrelatively faster release and administered. Moreover, beingbiocompatible and allow their adhesion to the mucosa in thedental pocket. (13)All clinical parameters were recorded at base line and 6weeks after treatment this precise period was takenDina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.according to Haffajee et al,and sokransky et al whoproved that greatest change in probing depth reduction andclinical attachment regain occurs within 1-3 months postSRP.(14)Regarding our results, all baseline recorded clinicalparameters revealed no significant difference amongstudied groups because they were selected randomly toavoid bias.Regarding group1 treated by Bifidobacterium probiotic gelin addition to SRP; showed statistically significantimprovement both clinically and microbiologicallycompared to the pretreatment values, this could beexplained by the fact that the probiotic strain used in thepresent study can perfectly adhere to subgingival biofilmsresulting in antimicrobial activity, as well as antioxidativeand immunomodulatory properties. It can modulate the oralmicrobiota by directly killing or inhibition of pathogenicbacterial growth or via producing several components thatact as antimicrobial agents, such as lactic acid, hydrogenperoxide and bacteriocins that may act alone or in concertin inhibiting pathogens.In addition it works well as host-modulating agents, as theyinfluenced the balance of proinflammatory and antiinflammatory cytokines and reduced attachment andalveolar bone losses, the local inflammation as well favoredthe tissue repair. They also produce antioxidants whichneutralize the free electrons which play a pivotal role inplaque formation as well as stain buildup. (15, 16)These results came in agreement with Invernici et al. intheir randomized clinical trial which they evaluated theeffect of Bifidobacterium animalis subsp. lactis (B. lactis)containing probiotic lozenges as adjuvant to scaling androot planing (SRP) in patients suffering of chronicperiodontitis. The patients treated with probioticexperienced superior results regarding decrease in probingpocket depth and clinical attachment gain. Furthermore,they demonstrated fewer periodontal pathogens of red andorange complexes and reduced proinflammatory cytokinelevels in gingival crevicular fluid when compared withpatients using placebo. (17)Regarding group 2 treated with Chlorhexidine gel inaddition to SRP; clinically and microbiologically showedstatistically significant improvement compared to theirpretreatment values, this could be explained as CHX is oneof the most used antimicrobial agents as it has a broadspectrum antimicrobial agents that play role in treatment ofgingivitis and periodontitis. Also it has an antiinflammatory action, inhibition of bone loss and promotethe attachment of fibroblast to the root surface. Moreover agreat effect on plaque accumulation and bleeding onprobing. (18, 19)These results are similar to findings ofseveral studies. (20, 21)4Our results in contrary with Butera et al. whom found intheir study that there is no antibacterial effect of the appliedprobiotic and CHX pastes as well as on clinical parametersregarding CHX group .The possible explanation for thevariation from that study results may be due to differentconcentration, forms and route of administration of appliedprobiotic in addition to different study design. Despite thisdisagreement their results found to be in accordance withour results in regard to probiotic as it has shownsignificance effect in improving periodontal parameters. (22)Regarding group3 treated by SRP only, clinically andmicrobiologically showed statistically significantimprovement compared to their pretreatment values. Theseresults could be attributed to that SRP generally reduces thelevel of microorganisms and inflammatory markers. Alsoslows down the progression of periodontal disease viaattachment gain and PD reduction. (23)In this study regarding Inter-group comparison ofperiopathognic bacteria p. gingivals and p. intermedia countrevealed marked statistical significance between probioticand CHX groups in compression to SRP alone group.These results explanation lie in the concept that relevant toguided pocket recolonization, (GPR) established byTughels et al., wherein the beneficial bacteria populate thesulcus and prevent the recolonization of periodontalpathogens through means of competitive inhibition bypreventing the adhesion of pathogenic bacteria, competingthe same nutrients. (3)On the other hand it could be because P.gingivalis andP.intermedia were found to colonize nearly all niches inthe oral cavity, such as tongue, mucosa, saliva even thetonsils. A translocation of these pathogens may occurrapidly and a recently root-planed deep pocket might be recolonized from the remaining untreated pockets or fromother intraoral niches, before a less pathogenic ecosystemcan be established. (24)Probiotics present a new ray of hope in periodontal therapy.With a proven track record of being safe and effective.6Conclusions:1. Considering the clinical relevance, localapplication of both Bifidobacterium probiotic geltested in this study as well as chlorhexidine gelseem to be a valid adjunctive therapy to SRPalone.2. Bifidobacterium probiotic revealed a significantimprovement on clinical indeces in addition toreduction of periopathogenic bacteria P. gingivalisand P. intermedia.3. During this study, no side effects were detectedand hence probiotic gel can be used safely inmedically compromised patients.Dina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.Figure (1):A- Case suffering from chronic periodontitis at baselineB-Case presentation after treatment (SRP Bifidobacterium Probiotic Gel)AB5Dina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.Figure (2):C- Plaque SamplingD- Application of Bifidobacterium Probiotic Gel)CofD6Dina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.Table (1): Clinical periodontal parameters among study groups pre- and post-treatmentPlaque Indexmean SDPrePost0.766 0.096 0.889 0.138 0.826 0.109 F 2.82P 0.0867.3%62.4%64.5%1.84 0.171.815 0.181.83 0.19F 0.054P 0.9480.356 0.060.341 0.0580.353 0.07F 0.147P 0.864 0.001* 0.001* 0.001*80.6%81.2%80.7%Pre3.29 0.393.06 0.453.28 0.39F 0.969P 0.392Post2.02 0.421.97 0.321.92 0.23F 0.244P 0.785 0.001* 0.001* 0.001*38.6%35.6%41.5%Pre2.79 0.342.57 0.342.78 0.31F 1.41P 0.26Post1.87 0.411.96 0.412.25 0.35F 2.60P 0.09 0.001* 0.001* 0.001*32.9%23.7%19.1%Paired t testp-value% of changePaired t testp-value% of change7test ofsignificanceF 1.53P 0.236 0.001*PostPaired t testp-value% of changeGroup 3n 102.33 0.21 0.001*Gingival Index Premean SDClinicalAttachmentlossmean SDGroup 2n 102.49 0.245 0.001*Paired t testp-value% of changeProbing depthmean SDGroup 1n 102.34 0.24within groupsignificanceP1 0.161P2 0.894P3 0.127P1 0.025*P2 0.257P3 0.235P1 0.749P2 0.912P3 0.835P1 0.612P2 0.919P3 0.685P1 0.229P2 0.958P3 0.249P1 0.722P2 0.249P3 0.737P1 0.148P2 0.947P3 0.167P1 0.609P2 0.038*P3 0.107Dina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.Table (2): Total bacterial count counts of P.intermedia & P. gingivalis among study groups pre- and post-treatmentGroup 1n 10Group 2n 10Group 3n 10test ofwithinsignifica groupncesignificance884.0 187.3 965.0 166.0 F 0.33P1 0.58492P 0.722P2 0.435P3 0.815581.0 177.6 612.0 146.3 F 1.09P1 0.31705P 0.35P2 0.163P3 0.681 0.001* 0.001*34.3%36.6%99.00 18.792.0 8.93P 0.154P1 0.775P2 0.52P3 0.8812 1.519 3.1P1 0.292P 0.001P2 0.001**P3 0.001*P 0.001*P 0.002*Pre928.50 183.88Post505 174.42Paired t test%of changePreP.intermediamean SDPost 0.001*45.6%35.0 11.28Paired t testP 0.006*% of change68.6%63.6%40.6%Pre93 14.4382 17.5289.0 10.15p 0.235P1 0.197P2 0.746P3 0.110Post7.0 1.49.0 2.077.0 1.9p 0.002*P1 0.644P2 0.01*P3 0.03*Paired t testp 0.001*p .001*p 0.001*% of change76.7%67.9%41.4%Totalbacterialcountmean SDP.gingivalismean SD11 2.5F: One Way ANOVA test # by Post Hic Tukey test, p1: difference between group 1&2, p2: difference between group 1&3, p3: differencebetween group 2&3KW: Kruskal Wallis test, p1: difference between group 1& 2, p2: difference between group 1&3, p3: difference between group 2&38Dina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.Table (2): Total bacterial count counts of P.intermedia & P. gingivalis among study groups pre- and post-treatmentGroup 1n 10Group 2n 10Group 3n 10test ofwithinsignifica groupncesignificance884.0 187.3 965.0 166.0 F 0.33P1 0.58492P 0.722P2 0.435P3 0.815581.0 177.6 612.0 146.3 F 1.09P1 0.31705P 0.35P2 0.163P3 0.681 0.001* 0.001*34.3%36.6%99.00 18.792.0 8.93P 0.154P1 0.775P2 0.52P3 0.8812 1.519 3.1P1 0.292P 0.001P2 0.001**P3 0.001*P 0.001*P 0.002*Pre928.50 183.88Post505 174.42Paired t test%of changePreP.intermediamean SDPost 0.001*45.6%35.0 11.28Paired t testP 0.006*% of change68.6%63.6%40.6%Pre93 14.4382 17.5289.0 10.15p 0.235P1 0.197P2 0.746P3 0.110Post7.0 1.49.0 2.077.0 1.9p 0.002*P1 0.644P2 0.01*P3 0.03*Paired t testp 0.001*p .001*p 0.001*% of change76.7%67.9%41.4%Totalbacterialcountmean SDP.gingivalismean SD11 2.5F: One Way ANOVA test # by Post Hic Tukey test, p1: difference between group 1&2, p2: difference between group 1&3, p3: differencebetween group 2&3KW: Kruskal Wallis test, p1: difference between group 1& 2, p2: difference between group 1&3, p3: difference between group 2&39Dina R. Abuazab
Mansoura Journal of Dentistry 2021;8(31):1-11.8- Singh RP, Damle SG, Chawla A. imodulations in young children on consumption1- Pihlstrom BL, Michalowicz BS, Johnson ofprobioticice-creamcontainingBifidobacterium lactis Bb12 and Lactobacillusacidophilus La5. Acta Odontol Scand. 2011;69(6): 389-394.2- Rhemrev GE, Timmerman MF, VeldkampI,Van Winkelhoff AJ, Van der Velden U.9- Toiviainen A, Jalasvuori H, Lahti E, Gursoy U,Immediate effect of instrumentation on theSalminen S, Fontana M, et al. Impact of medlozengeswithLactobacilluspockets under strict plaque control. J Clinrhamnosus GG and Bifidobacterium animalisPeriodontol 2006;33:42–8.subsp. lactis BB-12 on the number of salivarymutans streptococci, amount of plaque, gingival3- Teughels W, Newman MG, Coucke W, et al.Guiding periodontal pocket recolonization: fectious pathogens by chlorhexidine-coatedControlhealthy adults. Clin Oral Investig. 2015; 19(1):77-83.10- Lamster IB, Novak MJ. Host mediators in4- Modak, Shanta, et al. Rapid inactivation ofgloves. Infectioninflammation and the oral microbiome in&Hospitalgingival crevicular fluid: implications for thepathogenesis of periodontal disease. CriticalReviews in Oral Biology & Medicine 1992; 3:31-60.Epidemiology, 1992, 13.8: 463-471.11- Rao SK, Setty S, Acharya AB, Thakur SL.5- Teughels W, Durukan A, Ozcelik O, PauwelsM, Quirynen M, Haytac MC. Clinical andmicrobiological effects of Lactobacillus tis: a randomized ycyclinemicrospheres in chronic localized periodontitisand on Porphyromonas gingivalis. Journal 34.study. J Clin Periodontol. 2013; 40(11): 1025-12- Martin‐Cabezas,1035.R.,Davideau,J.L.,Tenenbaum, H., & Huck, O. (2016). Clinical6- Joint FAO/WHO Working Group. Workingefficacy of probiotics as an adjunctive therapyGroup Report on Drafting Guidelines for theto non‐surgical periodontal treatment of chronicEvaluationperiodontitis: A systematic review and meta‐ofProbioticsinFood;WHO:London, UK, 2002.analysis. Journalofclinicalperiodontology, 43(6), 520-530.7- Biavati B, Vescovo M, Torriani S, Bottazzi V.10Bifidobacteria: history, ecology, physiology and13- Jones DS, Woolfson AD, Brown AF, O'Neillapplications.Ann Microbiol. 2000; 50: 117-131.MJ. Mucoadhesive, syringeable drug deliveryDina R. Abuazab
Mansoura Journal of Dentistry valuationofclinicalefficacyof0.2%metronidazole to the periodontal pocket: Inchlorhexidine irrigation, 1.5% chlorhexidine gelvitro release kinetics, syringeability, mechanicaland 2.5 mg biodegradable chlorhexidine chip asandan adjunct to scaling and root planing in themucoadhesiveproperties.JournalofControlled Release. 1997;49:71-9management of Chronic Periodontitis. Journalof Dental Specialities. 2016;4(2):142-6.14- SocranskySS,HaffajeeADJP.Periodontal microbial ecology.21- Firkova E, Stamenov N. Effect of subgingival2005;application of chlorhexidine gel in chronic38(1):135-87.periodontitis. BioCell. 2019;43(2):1-3.15- Kuru BE, Laleman I, Yalnizoglu T, Kuru L,TeughelsW(2017)TheInfluenceofaBifidobacterium animalis Probiotic on GingivalHealth: A Randomized Controlled ClinicalTrial. Journal of periodontology.88 (11):1115–22- Butera, A., Gallo, S., Maiorani, C., Molino, D.,Chiesa, A., Preda, C& Scribante, A. ontal Therapy: Evaluation of Clinical andMicrobiological1123.Parameters. Microorganisms, 9(1), 69.16- Biavati, B., Vescovo, M., Torriani, S., &Bottazzi, V. (2000). Bifidobacteria: history,ecology, physiology and applications. Annals ofmicrobiology, 50(2), 117-13223- Loesche WJ, Giordano J, Soehren S, et al.Nonsurgical treatment of patients withperiodontal disease. Oral Surgery, Oral Medicine,Oral Pathology, Oral Radiology and Endodontics.81(5):533-543.17- Invernici, M. M., Furlaneto, F. A., Salvador, S.L., Ouwehand, A. C., Salminen, S., Mantziari,A., . & Messora, M. R. (2020). dulatesthe24- Beikler T, Abdeen G, Schnitzer S, et al.Microbiological shifts in intra‐and rapy. Journal of clinical periodontology2004; 31: 777-783.immunological response of oral mucosa inperiodontitispatients. Journalofclinicalperiodontology, 45(10), 1198-1210.18- Modak, Shanta, et al. Rapid inactivation ofinfectious pathogens by chlorhexidine-coatedgloves. InfectionControl&HospitalEpidemiology, 1992, 13.8: 463-471.19- Van der Weijden, G. A., et al. Three tion with chlorhexidine. Journal ofclinical periodontology, 2005, 32.1: 89-92.20- Vaish S, Dodwad V, Mahajan A, Gupta S.11Dina R. Abuazab
Abdelmesih, (Microbilogy, F. Medicine, Mansoura University) Gel was prepared in November 12, 2019 (Liver Research -FAB Lab, Pharmacognosy Department, Faculty of Pharmacy), Mansoura University, Egypt. Oral gel was acceptable mucoadhesion so that the medication remains on the spot of application for a longer time.