Transcription
STATE OF CALIFORNIA-HEALTH AND HUMAN SERVICE AGENCYDEPARTMENT OF SOCIAL SERVICES744 P Street Sacramento, CA 95814www.cdss.ca.govFOR THISTHIS TRANSMITTALTRANSMITTALREASON FOROctober 8, 2008ALL COUNTYCOUNTY INFORMATIONINFORMATIONNOTICENOTICENO.NO. I-82-08I-82-08[ ] State Law ChangeFederal LawLaw oror RegulationRegulation[ ] FederalChangeCourt OrderOrder[ ] CourtRequested by[ ] Clarification RequestedOne or More CountiesInitiated byDSSbyCCDSS[X] InitiatedTO:WELFARETO: ALLALL COUNTYCOUNTY WE L F A R E DIRECTORSDIRECTORSALLWELFAREALL COUNTYCOUNTY WE L F A R E SERVICESS E R V I C E S PROGRAMPROGRAM MANAGERSMANAGERSALLOFFICERSALL CHIEF PROBATIONPROBATION OFFICERSSUBJECT:S U B J E C T : OUTCOMEO U T C O M E INDICATORINDICATOR ONON HEALTHH E A L T H ANDAND DENTALDENTAL AASSESSMENTSSSESSMENTSImprovement and AccountabilityThe Child Welfare System ImprovementAccountabilityAct,Act, AssemblyAssembly BillBill (AB)(AB) 636,increased importanceimportance onon thethe needneed forfor accurate, timelytimely andand completecomplete Childplaced increasedServices (CWS)( C W S )data.data. TheTheprimaryprimarysourcesourceforfor thisthis datadata isis thethe ChildChild WelfareWelfare hproducesOutcomesServices Case Management(CWS/CMS), which produces Outcomes andAccountability QuarterlyAccountabilityQuarterly DataData ReportsReports forfor eacheach childchild welfare agency.County InformationInformation Noticeintended tocounties inin meetingmeetingThis All CountyNotice (ACIN)(ACIN) is intendedto assist countiesC W S programprogram documentation,documentation, datadata reportingreporting andand programprogram performanceperformancecritical CWSrequirements. This andand futurefuture ACINsACINs willwill provideprovide informationinformation tomeasurement requirements.to assistin followingfollowing uniformuniform programprogram policyentry procedures withcounties inpolicy andand data entrywith thethe goal ofcontinuously improvedW S / C M S datacontinuouslyimprovedCCWS/CMSdata accuracy.W S / C M S case recordsThe purpose ofof thisthis ACINACIN isis toto ensureensure iding existing programprogram requirementsrequirements and data entryentry proceduresprocedures regardingregarding healthhealthby providingand dentaldental .assessments. It is not intended to impose new requirements.Introduction ofIntroductionof NewNew Measure:Measure: MeasureMeasure 5B5B -– HealthHealthandand DentalDentalAssessmentsAssessmentsmeasure reportsreports thethe percentpercent ofof childrenchildren whowho meetmeet thethe periodicityperiodicity schedule forThis measureassessments. AttachmentAttachmentAA describesdescribesthethemethodologymethodology used formedical and dental assessments.new measure. The requirementsrequirements forthethis newfor thesethese assessmentsassessments are specified in thefollowing attachmentC H D P ) ProgramProgramfollowingattachmenttoto thethe ChildChild HealthHealth andand DisabilityDisability PreventionPrevention ((CHDP)provider th c01.pdf
All CountyCounty InformationInformation NoticeI-82-08Notice No.No. I-82-08Page TwoAdditionally,the percentpercent ofof childrenchildren whowho meetmeet thethe periodicityperiodicity schedule forAdditionally, it shows thedentaldental assessmentsassessments ininthethefollowingfollowing CHDPC H D Pproviderprovider informationinformation dfAlthoughthese schedulesschedules applyto allall CHDPAlthough theseapply toC H D P ProgramProgram eligibleeligible children, this measuremeasure willapply onlyW S agencies.applyonly toto childrenchildren placedplaced byby countycounty CCWSAccording toAccordingto TitleTitle 17 of thethe CaliforniaCalifornia CodeCode ofof RegulationsRegulations (Division(Division 1,1, Chapter 4,Section 6847(c)),6847(c)), riodic healthhealthSubchapter 13, Article 4, Sectionassessments shallshall receivereceiveoneone assessmentassessmentduringduring eacheachageage periodperiod listed listed. [and][and] .will.willassessmentson thethe first day he or she enters a newnew agebe considered overdue forfor anan assessment onperiod withoutbeing performedperformed inperiod." For example,periodwithout assessmentassessment beingin thethe previousprevious ageage period.”must receive at least one CHDPC H D P healthhealth assessmentassessment (or(or equivalent)equivalent) betweenbetween hishisa child mustand thirdthird birthdays.birthdays.or her second andHealth Insurance PortabilityPortability and AccountabilityAccountability ActHealthHealth InsuranceInsurance PortabilityPortability andand AccountabilityAccountability Act of 19961996 doesdoes notnot restrictrestrict thetheThe Healthinformation bysocial workerworker oror juvenilejuvenile probationprobation officerofficer whoreceipt of medical informationby a socialwho hasand custodycustody ofof aa fosterfoster childchild andand doesdoes notnot restrictrestrict thethe entryentry of the child’schild's medicalmedicalcare clarifiedonthispointby ABinformation into the CWS/CMSState law has been clarified on this point by1687 (Statues ofof 2007), whichwhich recentlyrecently added Civil Code 56.103. EntryEntry ofof medicalmedical data1687into theW S / C M S systemsystem andandprovisionprovision ofof thethe healthhealth passportpassport toto thethe child’schild's fosterintothe CCWS/CMSparent are requiredrequired underunder statelaw to assist withwith thethe coordinationcoordination ofparentstate lawof healthhealth carecare serviceminor andThe fosterfoster parentparent should beto the minorand thusthus allowedallowed underunder CivilCivil CodeCode 56.103. Thestrongly advised aboutabout the need toto keepkeep thethe child’schild's healthhealth informationinformationcarefully and stronglyconfidential, aside fromfrom sharing itit withwith thethe child’schild's socialsocial worker,worker, probationprobation officer,officer, orconfidential,medical servicesservices provider.provider.Pleaseto thethe HealthHealth CareCare ProgramProgram forfor ChildrenChildren inin FosterFoster Care atPlease useuse thethe followingfollowing linklink tofor additionaladditional FC/Documents/guide.pdf forassistance. ForForaacurrentcurrent rosterroster ofof dentistsdentists acceptingaccepting newnew Denti-Caland resource assistance.patients: http://www.denti-cal.ca.gov/WSI/Bene.jsp?fname sp?fname ProvReferralpatients:Data Entry Instructionsentry instructions,instructions, please refer toFor data entryto thethe HealthHealth EducationEducation Passport New UserCurriculumCurriculum rriculum/HEP NU/ 10 HEP 101.doc# Toc162326346.
All CountyCounty InformationInformation NoticeNotice No.I-82-08No. I-82-08Page Threefollowing sectionsThe followingsections applyapply toto MeasureMeasure 5B:Entering CHDPExamsC H D P MedicalMedical and DentalDental Ex a m s (page 29)Service ProviderProvider NotebookNotebook (page 33) andCreating a ServiceRecording WellWell ChildChild Exam Result (page 34)The Newwaswith ReleaseRelease 6.16.1 on November17, 2007.New User CurriculumCurriculum wa s updatedupdated withNovember 17,the instructionsinstructions in the curriculum.curriculum. InIn addition,addition, countiescounties areare screenshotsscreenshots withwith theThere aredemonstrate theentry withManager.able to demonstratethe data entrywith thethe curriculumcurriculum andand Scenario Manager.Two quarters of test data willwill be shared withwith the counties. FollowingFollowing thethe test period,period, themeasure willwill officiallyofficially become a part of the Child Welfare SystemSystem ImprovementImprovement andand5B measureABquarterly reportsreports (estimated2008 report)report) and will bebe postedpostedAB 636, quarterly(estimated startstart date:date: January 2008at http://cssr.berkeley.edu/ucb childwelfare/Ccfsr.aspx .questions oror needneed furtherfurther information,information, please contactcontact your California ChildChildyou havehave questionsIfIf youServices ReviewReview ConsultantConsultant at (916)-651-8100, oror sendsend anan email toand Family Serviceschldserv@dss.ca.gov.Sincerely,Original DocumentDocument SignedSigned By:By:OriginalFranciscoFrancisco SanchezSanchez forforGREGORYE. ROSEGREGORY EROSEDeputyDeputy DirectorDirectorDivisionChildren andand Family Services Divisionc: CaliforniaCalifornia WelfareWelfare DirectorsDirectors AssociationProbation Officers of CaliforniaCaliforniaChief ProbationAttachmentsAttachments
AttachmentAttachment AMETHODOLOGY FOR MMEASUREE A S U R E 5BMedical andand DentalDental Care ExaminationsDescriptionThis measuremeasure reportsreports thethe percentpercent ofof childrenchildren whowho meetmeet thethe periodicityperiodicity scheduleas specifiedspecified ininthethefollowingfollowing attachmentattachment to the Childfor medicalmedical assessmentsassessments asDisability PreventionC H D P ) ProgramProgram providerprovider manual:Health and DisabilityPrevention cations/MastersOther/CHDP/forms/periodhealth c01.pdfAnd the percentpercent ofof childrenchildren who meetmeet thethe periodicityperiodicity schedule forfor g CHDPC H D Pproviderproviderinformationinformation hdppl0413.pdfAlthough theseC H D P ProgramProgram eligibleeligible children, thisAlthoughthese schedulesschedules apply toto allall CHDPapply only to childrencounty childmeasure will applychildren placed by countychild welfarewelfare serviceagencies.AccordingAccording toto TitleTitle 17 of thethe CaliforniaCalifornia CodeCode ofof RegulationsRegulations (Division(Division 1, Chapter 4,Section 6847(c)),6847(c)), “Persons"Personseligibleeligibleforfor periodicperiodic healthhealthSubchapter 13, Article 4, period listed listed. [and][and]assessmentson thethe first day he or she enters.will be considered overdue forfor anan assessment onnew age periodperiod withoutwithout assessmentbeing performedperformed in the previousprevious agea newassessment beingperiod." For example, a child must receive at least one CH D P healthhealthperiod.”CHDPassessment (or(or equivalent)equivalent) betweenbetween hishis oror herher secondsecond andand thirdthird birthdays.birthdays.assessmentFrequencyreport runs quarterly. MinorsMinors must be in placementplacement the lastlast dayday ofof theThis es:in openopen out-of-homeout-of-home placementplacementChild indays oror moremorePlacement episodes open 31 daysDepartment ("34")placementCounty Welfare Department(“34”) is the responsible placementagencyPrimary assignment at quarter’squarter's endend determinesdetermines countycounty assignmentMinors’Minors' age taken from quarter’squarter's endPlacement home is in California
AttachmentAttachment AExcludes:All non-childnon-child welfare departmentdepartment placementsplacements (probation,(probation, etc.)than 31Placement episodes less than31 daysin placementplacement homeshomes outsideoutside of CaliforniaCaliforniaChildren inplacement (no run-aways oror openopen episode/closedepisode/closedChildren not in aa placementOHP)OHP)Non-foster carecareplacementsplacements( (NFC PLCTNon-fosterN F C P L C T table)Non-dependentNon-dependent LegalLegal Guardians:1413o s:codes: 1409,1410,1411,14121409,1410,1411,1412 and 1413(Guardian Home)Home)o PlacementPlacement FacilityFacility TypeType 54115411 (GuardianCHDP MEDICAL HEALTH EXAMSDoes the child have a current CCHDPH D P medicalmedical assessmentassessment oror equivalentequivalent asas ofof thechild's currentcurrent age period?period?end of the child’sService contactcontact type codes:Delivered Service1746 –- HealthHealth//CCHDPH D P ServicesServices1769 –- CCHDPH D P MedicalMedical DeliveredDeliveredE P -- CCHDPH D P Equivalent3236 -–HHEPEquivalent PhysicalPhysical ExamE P -- CCHDPH D P Physical3238 -–HHEPPhysical ExamNote:Note: CodeCode 32373237 “Medical"Medical Visit”Visit" isis notnot usedused toto indicateindicate aa CHDPCHDPequivalentequivalentexam.exam.CHDP DENTAL EXAMSDoes the child have a currentcurrent CHDPC H D P dentaldental referralreferral asas ofof thethe endend ofof thethe child’schild'scurrent age period?period?currentService contactcontact type codes:Delivered Service- CH D P DentalDental DeliveredDelivered1768 –CHDP-HE P - Periodic Dental3239 –HEPDental ExamNote:Note: CodeCode 32373237 “Dental"Dental Visit”Visit" isis notnotusedused totoindicateindicate aaCHDPCHDPequivalentequivalent exam.exam.
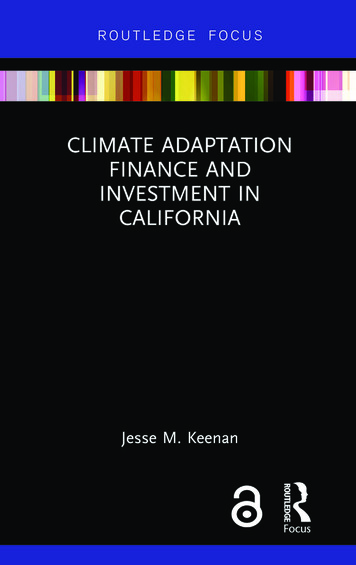
Section 101Table 101.1 P E R I O D I C I T Y S C H E D U L E FORH E A L T H ASSESSMENT R E Q U I R E M E N T S BY A G E GROUPSAge of Person Being ScreenedScreeningRequirementUnder1-21 mo,mos.I n t e r v a l U n t i l Next E x a m1 mo. 2 mo.History and P h y s i c a l E x a m i n a t i o nDental A s s e s s m e n tNutritional A s s e s s m e n tDevelopmental/BehvioralAnticipatory G u i d a n c e7-910-12mos.mos.mos.mos.2 mo.2 mo.3 mos.3 mos.13-1516-23mos.mos.23 mos. 6 mos.3Yr.Yr.Yr.Yr.Yr.Yr.1yr2yr3 yr4 yr.4 yr.None. . . . .Head CircumferenceH e i g h t / L e n g t h and W e i g h t.B l o o d PressureSensoryScreeningV i s u a l A c u i t y Test ( S n e l l e n ).C l i n i c a l /Tests. .T u b e r c u l i n TestT B Exposure R i s k Assessment.Hematocrit or H e m o g l o b i n.U r i n e D i p s t i c k or U r i n a l y s i sBlood Lead TestBlood Lead Risk AssessmentOther.2. .Laboratory. .TESTSV D R L . RPR, or A R TTo be done w h e n health history and/or physical examination warrants.Gonorrhea TestTo be done w h e n health history and/or p h y s i c a l examination warrants.Chlamydia TestTo be done w h e n health history and/or physical examination warrants.Papanicolaou ( P a p ) S m e a rTo be done w h e n health history and/or physical examination warrants.Sickle CellTo be done w h e n health history and/or physical examination warrants.O v a and ParasitesTo be done w h e n health history and/or physical examination warrants.A d m i n i s t e r as necessary to make status current.ImmunizationsNOTE:.Pelvic E x a m 1Measurements17-2013-16Yr.9-121 yr.6-84-5.Tobacco Assessment5-63-4C h i l d r e n coming u n d e r care who have not received all the recommended procedures for an earlier age should be brought upto-date as a p p r o p r i a t e .1. R e c o m m e n d e d for s e x u a l l y active females and females age 18 years and older.2.Snellentesting and audiometric testing should start at age 3 years i f possible. C l i n i c a l observation and nonaudiometric testingm a y be substituted if child is uncooperative.Department o f H e a l t h C a r e S e r v i c e s , Systems o f C a r e D i v i s i o n . C h i l d r e n ' s M e d i c a l S e r v i c e s B r a n c hDate issued September 2007101-2.
State of California-Health and Human Services AgencyDepartment of Health ServicesCaliforniaDepartmentof Health ServicesSANDRASHEWRYARNOLD SCHWARZENEGGERGovernorDirectorJune 18, 2004C H D P Program Letter No.: 04-13TO:A L L COUNTY CHILD H E A L T H AND DISABILITY P R E V E N T I O N (CHDP)PROGRAM DIRECTORS, DEPUTY DIRECTORS, S T A T E CHILDREN'SMEDICAL S E R V I C E S (CMS) BRANCH S T A F F AND REGIONAL O F F I C ESTAFFSUBJECT:C H D P P R O V I D E R INFORMATION NOTICE NO.: 04-13 CHDPRECOMMENDATION TO R E F E R C H I L D R E N TO A D E N T I S TBEGINNING A T ONE Y E A R O F A G EEnclosed is the C H D P Provider Information Notice No.: 04-13 announcing the newC H D P recommendation to refer children annually to a dentist beginning at one year ofage. Also included as enclosures are the following documents:1)T h e American Academy of Pediatrics policy statement, "Oral Health RiskAssessment Timing and Establishment of the Dental Home;"2)The revised Periodicity Schedule for Dental Referral by Age;3)The revised PM 160 Dental Guide.Please review and distribute this Provider Information Notice and enclosures, withoutany changes, to providers in your local program area and complete and return theenclosed "Report of Distribution."Please be prepared to assist providers in locating dentists if they should have difficultyin making these referrals. If you have any questions, please contact your RegionalOffice Nurse Consultant.Original signed by Marian Dalsey, M.D., M.P.H.Marian Dalsey, M.D., M.P.H., Acting ChiefChildren's Medical Services BranchEnclosures1515 K Street, Suite 400, MS 8100, P.O. Box 997413, Sacramento, CA 95899-7413(916) 327-1400Internet Address: http://www.dhs.ca.gov/pcfh/cms
State of California-Health and Human Services AgencyDepartment of Health ServicesCaliforniaDepartmentof Health ServicesSANDRASHEWRYARNOLD SCHWARZENEGGERGovernorDirectorJune 18, 2004C H D P Provider Information Notice No.: 04-13TO:A L L CHILD H E A L T H AND DISABILITY P R E V E N T I O N (CHDP) P R O G R A MPROVIDERSSUBJECT:C H D P RECOMMENDATION O F DENTAL R E F E R R A L BEGINNING A TONE Y E A R OF A G EThe purpose of this notice is to inform providers of the new C H D P recommendation tobegin referring children to a dentist at one year of age, and to provide changes to certaindocuments reflecting the new recommendation.Background InformationDental caries is the most prevalent infectious and chronic childhood disease (five timesmore prevalent than asthma). Early childhood caries ( E C C ) often starts as soon as thefirst tooth erupts, around 6 months of age. Studies show that more than one-third ofchildren have dental caries by the time they reach kindergarten. E C C affects children inall racial and socioeconomic groups; however, there is a higher prevalence in children oflow-income families, where it occurs in epidemic proportions.In May of 2003, the American Academy of Pediatrics (AAP) released a Policy Statement,"Oral Health Risk Assessment Timing and Establishment of the Dental Home." In thisStatement, the A A P discusses the transference of oral flora from the mother (or othercaregiver) to the child, inoculating the child between 6 and 30 months with cariogenicorganisms. To prevent caries in children, high-risk children and caregivers must beidentified, preferably during prenatal care. Decreasing the level of cariogenic bacteria inthe mother's oral flora can impact the child's predisposition to caries. Aggressivestrategies for both the mother and the child should be adopted, including anticipatoryguidance, behavior modification (oral hygiene and feeding practices) and theestablishment of a dental home by one year of age. The complete policy statement isattached as Enclosure 1 or you may visit the A A P website: www.aap.org.1515 K Street, Suite 400, MS 8100, P.O. Box 997413, Sacramento, CA 95899-7413(916) 327-1400Internet Address: http://www.dhs.ca.goy/pcfh/cms
C H D P Information Notice No.: 04-13Page 2June 18, 2004Another source of pertinent information for the health care provider is, "A HealthProfessional's Guide to Pediatric Oral Health Management" found at the NationalMaternal and Child Health website, www.mchoralhealth.org/PediatricOH/index.htm.This guide offers 7 modules for training health care providers to identify high-risk children,screen, offer anticipatory guidance and refer infants and young children to oral healthprofessionals.National dental and public health organizations also support a child's first dental visit byone year of age. These include the American Dental Association, American Academy ofPediatric Dentistry, American Public Health Association, Association of State andTerritorial Dental Directors and statewide organizations such as California DentalAssociation, California Society of Pediatric Dentists, and the California Dental Hygienist'sAssociation.Early and Periodic, Screening, Diagnosis and Treatment (EPSDT) statutes (Code ofFederal Regulations, Title 42) governing the State C H D P program require the provision ofdental services "at intervals which meet reasonable standards of dental practice, asdetermined by the State after consultation with recognized dental organizations involvedin child health care."Change in Age Recommendation for Dental ReferralsTherefore, in accordance with the recommendation of the A A P and the above-mentionednational and statewide dental organizations, effective the date of this letter, the C H D Pprogram recommends a direct referral to a dentist beginning at one year of age andannually thereafter. This recommendation does not change the regulatory mandate of adental referral at three years of age.If you are unable to locate a dentist to refer the child, please contact your local C H D Pprogram for assistance.The following documents have been revised to reflect the new recommendation.Relevant changes to the C H D P Provider Manual and Health Assessment Guidelines willbe available at a later date.
C H D P Information Notice No.: 04-13Page 3June 18, 20041.Periodicity Schedule for Dental Referral by Age. (Enclosure 2)2.The revised "PM 160 Dental Guide" is included, and can be downloaded from theC H D P website: www.dhs.ca.gov/chdp (Click on forms and publications) for its fullcolor version. (Enclosure 3)If you have any questions, please contact your local C H D P program.Original signed by Marian Dalsey, M.D., M.P.H.Marian Dalsey, M.D., M.P.H., Acting ChiefChildren's Medical Services BranchEnclosures
AMERICAN A C A D E M Y OF PEDIATRICSPOLICY STATEMENTOrganizational Principles to Guide and Define the C h i l d Health Care System a n d / o r improve the Health of A l l ChildrenSection on Pediatric DentistryOral Health Risk Assessment Timing and Establishment of theDental HomeA B S T R A C T . Early childhood dental caries has beenreported by the Centers for Disease Control and Preven tion to be perhaps the most prevalent infectious diseaseof our nation's children. Early childhood dental cariesoccurs in all racial and socioeconomic groups; however, ittends to be more prevalent in low-income children, inwhom it occurs in epidemic proportions. Dental cariesresults from an overgrowth of specific organisms that area part of normally occurring human flora. Human dentalflora is site specific, and an infant is not colonized untilthe eruption of the primary dentition at approximately 6to 30 months of age. The most likely source of inocula tion of an infant's dental flora is the mother or anotherintimate care provider, through shared utensils, etc. De creasing the level of cariogenic organisms in the mother'sdental flora at the time of colonization can significantlyimpact the child's predisposition to caries. To preventcaries in children, high-risk individuals must be identi fied at an early age (preferably high-risk mothers duringprenatal care), and aggressive strategies should beadopted, including anticipatory guidance, behavior mod ifications (oral hygiene and feeding practices), and estab lishment of a dental home by 1 year of age for childrendeemed at risk.TINTRODUCTIONh e C e n t e r s for D i s e a s e C o n t r o l a n d P r e v e n t i o nr e p o r t s that d e n t a l caries i s p e r h a p s the m o s tp r e v a l e n t o f i n f e c t i o u s diseases i n o u r n a t i o n ' sc h i l d r e n . D e n t a l c a r i e s i s 5 times m o r e c o m m o n t h a na s t h m a a n d 7 t i m e s m o r e c o m m o n than h a y f e v e r i nc h i l d r e n . M o r e t h a n 40% o f c h i l d r e n h a v e toothd e c a y b y the t i m e t h e y reach k i n d e r g a r t e n . I n f a n t sw h o are o f l o w s o c i o e c o n o m i c status, w h o s e m o t h e r shave a low education level, and w h o consume sug a r y foods are 32 t i m e s m o r e l i k e l y to h a v e caries atthe age o f 3 y e a r s t h a n c h i l d r e n i n w h o m those r i s kfactors are not p r e s e n t . D e c a y of p r i m a r y teeth canaffect c h i l d r e n ' s g r o w t h , lead t o m a l o c c l u s i o n , a n dr e s u l t i n s i g n i f i c a n t p a i n a n d p o t e n t i a l l y life-threat e n i n g s w e l l i n g . B e c a u s e p e d i a t r i c i a n s a n d other pe d i a t r i c h e a l t h care p r o f e s s i o n a l s are far m o r e l i k e l y toe n c o u n t e r n e w m o t h e r s a n d i n f a n t s t h a n are d e n t i s t s ,it is e s s e n t i a l that they be a w a r e of the i n f e c t i o u sp a t h o p h y s i o l o g y a n d associated r i s k factors o f e a r l yc h i l d h o o d d e n t a l caries t o m a k e a p p r o p r i a t e d e c i 123P E D I A T R I C S ( I S S N 0031 4005). Copyright 2003 by the A m e r i c a n A c a d emy of Pediatrics.sions r e g a r d i n g t i m e l y a n d effective i n t e r v e n t i o n .D e n t a l d e c a y c a n be w e l l a d v a n c e d by 3 y e a r s of age.BACKGROUNDD e n t a l caries r e s u l t s f r o m a n o v e r g r o w t h o f spe cific o r g a n i s m s that are p a r t of n o r m a l l y o c c u r r i n gh u m a n d e n t a l f l o r a . Streptococcus mutans a n d Lacto bacillus species are c o n s i d e r e d to be p r i n c i p a l i n d i c a tor o r g a n i s m s of those of a c i d u r i c bacteria r e s p o n s i ble for caries. H u m a n d e n t a l f l o r a i s site specific, a n da n i n f a n t i s not c o l o n i z e d w i t h n o r m a l d e n t a l florau n t i l the e r u p t i o n of the p r i m a r y d e n t i t i o n at a p p r o x i m a t e l y 6 to 30 m o n t h s of age, - T h e v e r t i c a l c o l o n i z a t i o n of S mutans f r o m m o t h e r to i n f a n t is w e l ld o c u m e n t e d . ' In fact, g e n o t y p e s of S mutans in i n fants a p p e a r i d e n t i c a l to those p r e s e n t in m o t h e r s inapproximately 7 1 % of mother-infant pairs. Further m o r e , e v i d e n c e suggests that specific o r g a n i s m s ex hibit discrete w i n d o w s o f i n o c u l a t i o n ; the a c q u i s i t i o nof S mutans occurs at an a v e r a g e age of a p p r o x i mately 2 years.45768910The s i g n i f i c a n c e of t h i s i n f o r m a t i o n becomes fo c u s e d w h e n c o n s i d e r i n g 3 p o i n t s . F i r s t , h i g h cariesrates r u n i n f a m i l i e s a n d are p a s s e d f r o m m o t h e r t oc h i l d f r o m generation to g e n e r a t i o n . T h e c h i l d r e n ofm o t h e r s w i t h h i g h c a r i e s rates are at a h i g h e r r i s k ofdecay,S e c o n d , a p p r o x i m a t e l y 70% o f all dentalcaries are f o u n d i n 2 0 % o f o u r n a t i o n ' s c h i l d r e n .T h i r d , the m o d i f i c a t i o n of the m o t h e r ' s d e n t a l flora atthe t i m e of the i n f a n t ' s c o l o n i z a t i o n can s i g n i f i c a n t l yi m p a c t the c h i l d ' s caries r a t e .Therefore, an oralh e a l t h r i s k a s s e s s m e n t before 1 year of age affordsthe o p p o r t u n i t y to i d e n t i f y h i g h - r i s k patients a n d top r o v i d e t i m e l y r e f e r r a l a n d i n t e r v e n t i o n for the c h i l da n d a l l o w s a n i n v a l u a b l e o p p o r t u n i t y t o decrease thel e v e l of cariogenic o r g a n i s m s in the m o t h e r w i t h as i g n i f i c a n t caries r i s k before a n d d u r i n g c o l o n i z a t i o nof the i n f a n t .1112131 4 - 1 6BASIC PREVENTIVE STRATEGIESH i s t o r i c a l l y , the a p p r o a c h to p r e v e n t i n g the d e v e l o p m e n t of d e n t a l caries h a s been to establish a n dm a i n t a i n good o r a l h y g i e n e , o p t i m i z e s y s t e m i c a n dtopical f l u o r i d e e x p o s u r e , a n d e l i m i n a t e p r o l o n g e de x p o s u r e to s i m p l e s u g a r s in the diet. T h e success ofthis age-old a p p r o a c h is also the f o u n d a t i o n for thei d e a l s t a n d a r d of e s t a b l i s h m e n t of the d e n t a l h o m eP E D I A T R I C S V o l . 111 No. 5 May 20031113
by 1 y e a r of age, as e n d o r s e d by the A m e r i c a n D e n t a lA s s o c i a t i o n , the A m e r i c a n A c a d e m y o f P e d i a t r i cDentistry, supporting organizations of Bright F u t u r e s , a n d n u m e r o u s other c h i l d r e n ' s h e a l t h o r g a n i zations.D e n t a l caries t y p i c a l l y r e s u l t s f r o m d i e t - m e d i a t e ds h i f t s i n d e n t a l bacterial p o p u l a t i o n s that f a v o r acidogenic-aciduric (cariogenic) o r g a n i s m s , T h e j u d i c i o u s o p t i m i z a t i o n o f diet, f l u o r i d e i n t a k e , a n d h y giene reverses the a c i d u r i c s h i f t , r e s u l t i n g i n f e w e rc a r i o g e n i c flora a n d d e c r e a s e d rates o f caries. C l i n i cal o b s e r v a t i o n s suggest that a c i d u r i c shifts are oftenassociated w i t h pregnancy, w i t h return to prepreg n a n c y c a r i o g e n i c - b e n i g n flora r a t i o o c c u r r i n g o n thes a m e t i m e l i n e as the c o l o n i z a t i o n of the i n f a n t w i t hd e n t a l f l o r a (6 to 30 m o n t h s of age). T h e o v e r a l lstrategy is to l o w e r the n u m b e r s of c a r i o g e n i c bacte r i a i n the m o t h e r ' s m o u t h a n d d e l a y c o l o n i z a t i o n a sl o n g a
by providing existing program requirements and data entry procedures regarding health and dental assessments. It is not intended to impose new requirements. Introduction of New Measure: Measure 5B - Health and Dental Assessments . This measure reports the percent of children who meet the periodicity schedule for medical and dental assessments.