Transcription
Recommendations of theSchool Health Work Group, convened jointlyby the California Department of Educationand the California Department of Health Services
Publishing InformationBuilding Infrastructure for Coordinated School Health:California’s Blueprint was developed by a statewidework group staffed by the School Health ConnectionsOffice of the California Department of Education andthe School Health Connections Office of the CaliforniaDepartment of Health Services. This document waspublished by the California Department of Education,721 Capitol Mall, Sacramento, California (mailingaddress: P.O. Box 944272, Sacramento, CA 942442720). It was distributed under the provisions of theLibrary Distribution Act and Government Code Section11096. 2000 by the California Department of EducationAll rights reservedNoticeThe guidance in Building Infrastructure for CoordinatedSchool Health: California’s Blueprint is not binding onlocal educational agencies or other entities. Except forthe statutes, regulations, and court decisions that arereferenced herein, the document is exemplary, andcompliance with it is not mandatory. (See EducationCode Section 33308.5.)Prepared for publicationby CSEA members.ii
ContentsForeword . vForewordPreface . viiPrefaceAcknowledgments . ixExecutive Summary . 1The California Blueprint:Blueprint: Goals and Action Steps . 11Goal 1: Coordinated school health policies and programs will support andcontribute to the positive development of children and youth . 12Goal 2: Policies at all levels will fully support coordinated school healthfor California’s diverse populations . 17Goal 3: Funds and resources will be allocated to support coordinated schoolhealth for California’s diverse populations . 19Goal 4: Closer collaboration and better coordination will be established withinand between the California Department of Education and the CaliforniaDepartment of Health Services, other state and local agencies, andbusiness and community partners . 23Goal 5: Personnel capacity in school health at the state and local levelswill increase and will reflect California’s diverse populations . 28Goal 6: Use of state-of-the-art, research-based strategies to implementcoordinated school health will increase . 31Appendixes . 33A. Executive Summary of CSHP Needs Assessment . 33B. Tables: California’s Leading Causes of Death . 43Selected ReferReferencesences . 57iii
iv
ForewordOne of the most important, cross-cutting socialpolicy perspectives to emerge in recent years is an awarenessthat no single institution can create all conditions that youngpeople need to flourish, not only in schools but intheir careers and as parents.—Melaville and BlankWE EMBRACE THE CONCEPT THAT A MULTITUDE OF INSTITUTIONS, AGENCIES, ANDorganizations must assume responsibility for the health and academic successof California’s children and youth. As such, more than 70 people from a broadspectrum of organizations worked together as members of the Coordinated School HealthWork Group to determine how best to build an interagency system of supports for the state’schildren and their families. The result was the development of Building Infrastructure forCoordinated School Health: California’California’ss Blueprint to provide recommendations andaction steps that can be initiated by the California Department of Education, the Departmentof Health Services, and other state departments; county offices of education; local healthdepartments; school districts and schools; and community and business partners.v
In the development of this document, the Work Group identified six goals focused on thefollowing elements:w Youth developmentw Policy developmentw Collaboration and coordinationw Personnel capacityw Research-based strategiesw FundingThe aim of the Coordinated School Health Work Group is to enable California’s childrenand adolescents to become healthy, successful students at school and contributing members intheir communities. This Blueprint delineates the foundation upon whichchildren and adolescents in California can develop their capabilities for leading rewardingand productive lives.A coordinated school health approach effectively addresses students’ health, thus improving their ability to learn. This approach features eight interrelated components: healtheducation; physical education; school health services; school nutrition services; schoolcounseling, psychological, and social services; a healthy school environment; and schoolsite promotion of health for staff.The Coordinated School Health Work Group invites and encourages you and others totake action in your community by implementing the Blueprint recommendations that followin this document.Joan Davies, Alameda County Office of EducationClaudia Epperson, Modesto City Schools, Robertson Road Healthy StartAlan Henderson, American Cancer Society and California State University, Long BeachCarla Niño, California State Parent–Teacher AssociationMaxine Sehring, American Academy of PediatricsGregory Thomas, California Conference of Local Health Department Officials/San Luis ObispoGregoregoryCounty Health Agencyvi
PrefaceThe term health is used in the broadest sense. Health ismuch more than simply the absence of disease; health involvesoptimal physical, mental, social, and emotional functioningand well-being.—World Health OrganizationRISING CONCERNS OVER THE STATE OF HEALTH OF OUR CHILDREN AND OUR YOUTH HAVEresulted in a national dialogue, proposed legislation, and myriad initiatives andproposals to deal with those concerns. Because schools touch most families, coordinated school health programs show considerable promise toward aiding those efforts.The previous emphasis in the schools on prevention is slowly shifting away from merely“fixing the kid”—focusing on deficits—to creating an environment that provides provensupport and opportunities for children and youth, especially among low-income and racialor ethnic populations. Youth are increasingly being given a meaningful role in the development of programs and efforts to address health issues. In the process they develop lifelong leadership skills that they may draw on in the future in their workplace and in theircommunities.vii
When asked to identify what is necessary for students to learn before high school graduation, Americans ranked health education above instruction in language arts, mathematics,and science in a recent Gallup Poll. Nine of 25 standards selected by the respondents—or36 percent of the top 25 rated standards—were health standards (Marzano, Kendall, andCicchinelli 1999).Research has established links between a student’s health and school performance(Symons et al. 1997; National Commission on the Role of the School and the Community inImproving Adolescent Health 1990; National Health/Education Consortium 1990). Further,numerous studies have established the effectiveness of school health programs in reducingspecific risky behaviors (Symons et al. 1997; National Commission on the Role of theSchool and the Community in Improving Adolescent Health 1990; Dryfoos 1990). However, what has been lacking is a coordinated approach to school health and the necessaryinfrastructure to support it (Council of Chief State School Officers 1991; National Commission on the Role of the School and the Community in Improving Adolescent Health 1990).A coordinated approach will improve the health of children and youth and their capacity tolearn through the support of their families, schools, and communities working together. Atits very core, coordinated school health focuses on keeping students healthy over time,reinforcing positive healthy behaviors throughout the school day, and making clear thatgood health and productive learning go hand in hand.viii
AcknowledgmentsThere is no question that our schools have a key role to playin helping our children begin a lifetime of good health.—Donna Shalala, U.S. Secretary of Health and Human ServicesSPECIAL THANKS ARE OFFERED TO THE MEMBERS OF THE WORK GROUP AND THE STATEagency liaisons who participated in the meetings and developed the goals and actionsteps described in this document. Also appreciated are the contributions of the manypersons who reviewed drafts and provided comments. In addition, thanks are extended tothe thousands of Californians committed to building the infrastructure for coordinatedschool health so that children and youth will be mentally, socially, emotionally, physically,and spiritually healthy and will be lifelong learners.The publication of this document and the important work that led to its developmentwere made possible by funding from the Centers for Disease Control and Prevention,Division of Adolescent and School Health. That support is gratefully acknowledged. Theassistance provided by the California Department of Education and the California Departmentof Health Services is also deeply appreciated.ix
Coordinated School HealthWork GroupFrancine Eisenrod, Director, Los Angeles UnifiedEisenrod,School District, Health, Drug, Alcohol, andTobacco Education ProgramsApril Allen, Regional Manager, Dairy Councilof CaliforniaMargaret Elliot, Executive Director, CaliforniaMargaretPhysical Education and Health ProjectJackie Allen, Chair, California Alliance of PupilService OrganizationsClaudia Epperson, Healthy Start Project Coordinator, Modesto City Elementary School District*eywbreyey,, Coordinator, StudentLucinda Mejdell AwbrSupport Services, Visalia Unified School DistrictDean FenleyFenley,, Project Officer, Centers for DiseaseControl and PreventionRobin Gray Ballard, 1999–2000 President,California Association for Health, PhysicalEducation, Recreation, and DanceJared Fine, California Dental Association andDental Health Administrator, Alameda CountyPublic Health DepartmentLisa Bass, Youth Program Manager, AmericanCancer Society, California Division, Inc.Bruce FisherFisher,, Teacher, Fortuna Union SchoolDistrictRobert Bates, Medical Consultant, CaliforniaDepartment of Health ServicesTara GallagherGallagher,, Student, Woodland Joint UnifiedSchool DistrictBonnie Bernard, Senior Program Associate,WestEd, School and Community HealthResearch GroupBeatriz Garcia-de la Rocha, CHAMP Coordinator,Garcia-deLos Angeles Unified School DistrictRuth Bowman, Consultant, California Departmentof EducationWanda Grant, Child Nutrition Director, El MonteCity School District, California School FoodService AssociationBeverly BradleyBradley,, Assistant Clinical Professor,University of California, San Diego, Schoolof MedicineNina Grayson, Regional Adviser, CaliforniaDepartment of Social Services, Welfare-to-WorkDivisionMaria Campbell-CaseyCampbell-Casey,, Consultant, The PublicHealth InstitutealterCyndi Guerra-WGuerra-Walteralter,, WriterTricia Capri, Senior Program Manager, CorporateContributions, Pacific Gas and Electric CompanyAlan Henderson, Past President, American CancerSociety, and Professor, California State University, Long Beach, Health and Science DepartmentTricia Chicagus, Field Coordinator of NursingServices, Los Angeles Unified School DistrictBetty HennessyHennessy,, Physical Education Consultant,Los Angeles County Office of EducationNorm Constantine, Director, WestEd, School andCommunity Health Research GroupLisa HersheyHershey,, Coordinator, California Departmentof Health Services, Vehicle Occupant SafetyProgram*MarthaMartha Cornejo, Secretary, Woodland JointUnified School District, Community ServiceLearning CenterTaj James, Director of Youth Policy and Development, Coleman Advocates for Teens and YouthPeter Cortese, Chief (Emeritus), Program Development and Services Branch, Division ofAdolescent and School Health, Centers forDisease Control and PreventionJim KoolerKooler,, Deputy Director, California Departmentof Alcohol and Drug ProgramsYvonne Larsen, Member 1992–2000, CaliforniaState Board of EducationGus Dalis, Director, Los Angeles County Office ofEducation, Center for Health EducationKathy Lewis, Deputy Superintendent, CaliforniaDepartment of EducationJoan Davies, Director, Alameda County Office ofEducation, Bay Region IV School Support Center*Willie Lopez, Communicable Disease Specialist II,Fresno County Human ServicesDaphne Dennis, Social Services Administrator, Cityof West HollywoodRic Loya, Coordinating Teacher Adviser, LosAngeles Unified School District, AIDS Prevention Unit, and Vice President, California Association of School Health EducatorsPat Dumais, Registered School Nurse, WoodlandJoint Unified School District*Member of the Steering Committeex
State Staff Liaisons to theCoordinated School HealthWork GroupBarbara Marquez, Chief, California Departmentof Health Services, Office of CommunityChallenge Grants†Terry Maxson, Director, Children’s Hospitalerry(San Diego) School HealthJeanne Bartelt, Physical Education Consultant,School Health Connections*Edward Melia, Special Assistant for Children andYouth, Health and Human Services Agency*Tameron Mitchell, Deputy Director, CaliforniaameronDepartment of Health Services*Barbara Baseggio, Administrator, ElementaryNetworks OfficeChristine Berry, HIV/AIDS Prevention EducaBerrytion Consultant, School Health ConnectionsGeorge Monteverdi, Vice President, AmericanAcademy of Pediatrics, California Chapter*Donna Bezdecheck, Assistant Consultant, SchoolHealth Connections*Dave Neilson, Chief, Children and FamilyServices, California Department of MentalHealth, Mental Health Specialist Systems ofCare—ChildrenMarilyn Briggs, Director and AssistantSuperintendent, Nutrition Services Division*Wade Brynelson, Assistant Superintendent,Brynelson,Learning Support and Partnerships Division*Gary Nelson, Senior Program Officer, TheGaryCalifornia Wellness Foundation†Linda NeuhauserNeuhauser,, Executive Director, University ofCalifornia, Berkeley, Wellness Guide Project†Anna Diaz, School Outreach Coordinator forHealth Care Access, School Health ConnectionsLarry DickeyLarryDickey,, Chief, Office of ClinicalPreventative MedicineCarla Niño, Vice President 1999, California StateParent–Teacher Association*Nancy Gelbard, Chief, School HealthConnections†Donna Petre, Judge, Yolo County Superior CourtPetre,Marisela Romero, Student, Woodland Joint UnifiedRomero,School DistrictGerald Kilbert, Administrator, Healthy KidsKilbert,Program Office*Jennifer Rousseve, Consultant, CaliforniaDepartment of Education††Linda Ward Russell, Coordinator, Los AngelesUnified School District, Pregnant/ParentingTeen Programs*Donald Lyman, Division Chief, Chronic Diseaseand Injury Control DivisionPaul Meyers, Consultant, Student SupportServices and ProgramsPatricia Michael, Consultant, Special Education*Sarah Samuels, President, Samuels and Associates*Michele Sartell, Manager, 100% Campaign: HealthSartell,Insurance for Every California Child†Maxine Sehring, Pediatrician, American Academyof Pediatrics*Emily Nahat, Former Administrator, SchoolHealth ConnectionsMaggie Petersen, Nurse Consultant, Children’sMedical Services BranchCaroline Roberts, Administrator, School HealthCarolineRoberts,ConnectionsPenny Stone, California School Nurses OrganizationLinda Tayloraylor,, Codirector, University of California,Los Angeles, Center for Mental Health in SchoolRugmini Shah, Former Chief, Maternal and ChildHealth Branch†Gregory Thomas, Representative, CaliforniaGregoregoryConference of Local Health Officers**Louis Vismara, Commissioner, California Childrenand Families State Commission*Stephen Wilkes, Facilitator, Stephen L. Wilkesand Associates*Rhonda Simpson-Brown, Pregnant MinorProgram Consultant, Family and CommunityPartnerships OfficeSusan Thompson, Administrator, Family andCommunity Partnerships OfficeAlice Trathen, Child Development Consultant,Child Development DivisionDeborah Wood, Director, California Healthy KidsResource CenterCalifornia Department of EducationCalifornia Department of Health Services*†Member of the Steering Committee†State staff liaison to the Steering Committee*xi
Page xii is blank
Executive SummaryA comprehensive school health program is anintegrated set of planned, sequential, school-affiliatedstrategies, activities, and services designed to promote theoptimal physical, emotional, social, and educational developmentof students. The program involves and is supportive of familiesand is determined by the local community, based on communityneeds, resources, standards, and requirements. It is coordinatedby a multidisciplinary team and is accountable to the communityfor program quality and effectiveness.—Institute of MedicineBuilding Infrastructure for Coordinated School Health1
2Building Infrastructure for Coordinated School HealthTInfrastructure1. An underlying baseor foundation, esp.for an organizationor a system.2. The basic facilities,services, andinstallations neededfor the functioningof a community orsociety, such astransportation andcommunicationssystems.— The American HeritageCollege DictionaryHE MOST SERIOUS AND COSTLY HEALTH AND SOCIAL PROBLEMS THAT AFFLICT OURnation are caused in large part by (1) behaviors that cause unintentional andintentional injuries; (2) abuse of drugs and alcohol; (3) behaviors leading toinfection by sexually transmitted diseases, including HIV infection, and unintended pregnancies; (4) use of tobacco; (5) inadequate physical activity; and(6) dietary patterns that cause disease. Ultimately, all those behaviors are preventable. They are usually established during youth, persist into adulthood, areinterrelated, and contribute simultaneously to poor health, inadequate education,and inappropriate social outcomes. By preventing health problems that afflict ouryouth and threaten their adulthood, coordinated school health programs can helpreduce the spiraling costs of health care, help improve educational outcomes, andfoster positive youth development.To address the health concerns of children and youth in a coordinated,comprehensive manner, the California Department of Education and theCalifornia Department of Health Services have embarked on a process to buildinfrastructure support for coordinated school health through a grant provided bythe Centers for Disease Control and Prevention. To that end the departments haveestablished separate but coordinated school health program offices known asSchool Health Connections. The offices form a cross-departmental team andwork with other state agencies and organizations and associations that supportthe well-being of children, youth, and families.This planning document identifies goals and prioritized action steps that canbe initiated by the Department of Education, the Department of Health Services,county offices of education, local health departments, school districts, andschools. The goals and action steps reflect input from a diverse group of respondents, including state-level policymakers; staff members in schools, schooldistricts, and county offices; families; students; community leaders; and expertsin the field of school health.Needs AssessmentThe California Department of Education contracted with the Evaluation andTraining Institute (ETI) to conduct a statewide needs assessment and develop apreliminary plan for building infrastructure for coordinated school health inCalifornia. ETI undertook the work in conjunction with SRI International. Theassessment identified assets and needs related to coordinated school health andcomprehensive school health education at the state and local levels. The sourcesof the data used to develop the needs assessment were the following:w Interviews with key informants from the California Department of Education, the California Department of Health Services, universities, localagencies, and nongovernmental organizationsw Focus groups comprising local school health professionals, students,parents, and community members in six rural and urban locations acrossthe statew A survey of school health professionals at county offices of education andlocal health departments
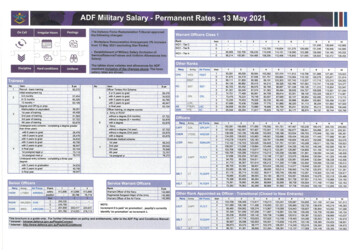
Building Infrastructure for Coordinated School HealthFor an overview of the findings, see Appendix A, “Executive Summary ofCSHP Needs Assessment.” For a more detailed description of the needs assessment, see “Comprehensive School Health Program Needs Assessment FinalReport” (California Department of Education 1998).Coordinated School HealthThe Centers for Disease Control and Prevention (CDC) describes coordinated schoolhealth as planned, integrated, school-affiliated programs designed to enhance thehealth of children and adolescents and comprising eight interrelated components: Comprehensive school health education Physical education Parent/community involvement Healthful school environment Health services Counseling, psychological services and social services Nutrition services Health promotion for staffEach of the components is present to some extent in most schools and districts butusually functions independently. Rarely have staff members serving in individualcomponents been directed to work with those in other components. Nor have theybeen informed of the activities taking place in those components.To change this situation, CDC is funding efforts in several states, including California,through the California Department of Education and the California Department ofHealth Services, to implement coordinated school health programs. Its intent is toenable the California agencies to work together to provide guidance and leadershiptoward promoting the health of children and youth through the state’s public schoolsystem.—PeterPeter A. Cortese, Chief (Emeritus), Program Development and Services Branch,Division of Adolescent and School Health, Centers for Disease Control and PreventionBlueprint for CaliforniaIn preparation for the development of a comprehensive plan for California, adraft blueprint was prepared and disseminated to the Coordinated School HealthWork Group for review and comments (see Table 1, “Model for the Development of California’s Blueprint for Coordinated School Health,” on p. 5). Thework group, composed of diverse stakeholders in school health, met twicebetween May and August 1999 to refine the draft. The group’s work was basedon the following assumptions (Lavin et al. 1992):w Education and health are interrelated.w Social morbidities are the biggest threats to health.3
4Building Infrastructure for Coordinated School Healthw A more comprehensive, integrated approach is needed.w Efforts should be focused in and around schools.w Prevention efforts are cost-effective (costs of inaction are highand escalating).A draft reflecting input from members of the work group was also disseminated for field review to hundreds of persons working in coordinated schoolhealth. (See “Mission of the Coordinated School Health Work Group” on p. 6.)The final blueprint includes six goals for accomplishing the mission. California’syouth, families, schools, communities, and government entities will work together to support the positive development of children and youth so that they willbe mentally, socially, emotionally, physically, and spiritually healthy and will belifelong learners. The blueprint also describes accompanying multilevel actionsteps that can be implemented by communities, organizations, and agencies at thelocal and state levels. The goals to be achieved are listed as follows:Goal 1: Coordinated school health policies and programs will support andcontribute to the positive development of children and youth.Goal 2: Policies at all levels will fully support coordinated school health forCalifornia’s diverse populations.Goal 3: Funds and resources will be allocated to support coordinated schoolhealth for California’s diverse populations.Goal 4: Closer collaboration and better coordination will be establishedwithin and between the California Department of Education and theCalifornia Department of Health Services, other state and localagencies, and business and community partners.Goal 5: Personnel capacity in school health at the state and local levels willincrease and will reflect California’s diverse populations.Goal 6: Use of state-of-the-art, research-based strategies to implementcoordinated school health will increase.Because California is one of the most diverse states in the nation, any effortof this magnitude must address the multicultural and multilinguistic needs ofchildren and youth and their families. A number of other factors apply to theplanning, implementation, and evaluation of many of the goals, such as youthdevelopment and social marketing.Within each goal, action steps are identified for state agencies, local healthdepartments, county offices of education, school districts, schools, andorganizations. Although the blueprint was developed on behalf of the CaliforniaDepartment of Education and the California Department of Health Services,implementation will be realized through broad-based partnerships involvingfamilies, schools, agencies, and communities to support further the well-beingand success of California’s children and youth.
Building Infrastructure for Coordinated School HealthTable 1Model for the Development of California’s Blueprintfor Coordinated School HealthSteeringcommitteeNeeds Assessment forCoordinated School HealthCenters forDisease ControlandPreventionCaliforniaDepartmentof HealthServicesw Community focus groupsCaliforniaDepartmentof Educationw Key informant interviewsw Surveys of county officesof education and localhealth departmentsw Review of key research,documents, laws, andregulationsStatewidework groupCommunity andfield commentsBlueprint forCoordinatedSchool Healthw Set priorities.w Identify action steps.Blueprint impacts at:w State levelw Regional/county levelw School sitesw Community levelComprehensive HealthAction Team(State InteragencyCoordination Group)w California Departmentof Educationw California Departmentof Health Servicesw California Departmentof Alcohol and DrugProgramsw California Departmentof Mental HealthSource: California Department of Health Services/California Department of Education, School Health Connections, August 18, 1999Dissemination,implementation,and evaluationof blueprint5
6Building Infrastructure for Coordinated School HealthWhen we adults are well, we are able to focus, learn, work,and be successful in what we do. Would this not be more sofor our children?—Lucinda Mejdell-Awbrey, CoordinatorStudent Support Services, Visalia Unified School DistrictSocial MarketingSocial marketing approaches are being used by a variety of public health programsto achieve large-scale behavioral changes. A practical definition is that socialmarketing applies commercial marketing approaches to achieve social goals.Operationally, social marketing uses the traditional mix of advertising, publicity,promotion, and personal sales from commercial marketing and adds communitydevelopment, consumer empowerment, institutional change, and partnership. Itemploys mass media and existing social systems, often called “channels,” to reachlarge numbers of consumers.—California Dietary Practices Survey, 1989–1997Mission of the Coordinated School Health Work GroupWhat we do:Through our contributions to this blueprint, this work group builds and maintainsthe infrastructure necessary for effective coordinated school health in California.How we do it:We work together through broad-based partnerships.For whom we do it:We do it for the agencies, organizations, groups, and communities that support thewell-being and success of California’s children and youth. Together, those groupswill advocate the health of children and youth to enhance the social and economicdevelopment of the communities in which they live.Purpose of the blueprint:The blueprint proposes an infrastructure that will enable us to achieve our vision.Why we do it:We do it to achieve our common vision for California’s children, families, andcommunities.
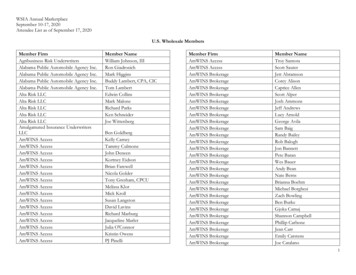
Building Infrastructure for Coordinated School HealthCalifornia’s Changing DemographicsCalifornia is one of the fastest-growing and most diverse states in the nation. By2040 California’s majority population, now white, will become a minority as theHispanic population increases. There will be no majority population. Consequently,it is imperative that all programs be designed and implemented in a culturallysensitive and linguistically appropriate manner. (See Fig. 1, below)FIGURE 1California Population Breakdown: 199653%White7%Black29%Hispanic11%Asian andPacific IslanderCalifornia Population Projection: 204030%White1%Other7%Black15%Asian andPacific Islander47%Hispanic7
8Building Infrastructure for Coordinated School HealthOnly when schools consider coordinated school healthprograms to be as essential as history, social studies, or languagearts will they be able to maximize academic achievementand positive health outcomes among the childrenand youths they serve.—Harriet Tyson
Office of the California Department of Education and the School Health Connections Office of the California Department of Health Services. This document was published by the California Department of Education, 721 Capitol Mall, Sacramento, California (mailing address: P.O. Box 944272, Sacramento, CA 94244-2720).