Transcription
CALIFORNIA PRO G R A M O NPOLICYA C C E SRESEARCHS TO CARECALIFORNIACalifornia Policy Research CenterCalifornia Program on Access to CareUniversity of California, Office of theUniversityPresident of CaliforniaThe California Program on Access to Care, in collaboration with the Center for California Health Workforce Studies at theUniversity of California, San Francisco presents:POLICY BRIEFING AGENDACalifornia Nurse Shortage: Impact of Nurse Education and Training InitiativesTuesday, August 23, 20051:30 to 4:00 pmUC Center1130 K St., Lower LevelSacramento, California1:30 pmWelcome and Opening Remarks: Gilbert Ojeda, Director, California Program on Access to Care (CPAC), CaliforniaPolicy Research Center, UC Office of the PresidentModerator: Joanne Spetz, Associate Professor and Associate Director, Center for California Health Workforce Studies,UC San Francisco1:40 pmThe Nursing Shortage and the Future of Nursing in CaliforniaJoanne Spetz, PhD, Associate Professor and Associate Director, Center for CaliforniaHealthWorkforce Studies, UC San Francisco2:00 pmSEIU Perspective on Nurse ShortageSharlyn Hansen, Executive Director, California Nurse Alliance, Service Employees International Union (SEIU)2:20 pmHospital Nurse Staffing: Today and TomorrowDorel Harms, Vice President, Quality and Professional Services, California Hospital Association2:40 pmBreak2:50 pmDealing with the Shortage: The Governor’s InitiativeThomas Johnson, Secretary of Veterans Affairs, Department of Veterans Affairs3:10 pmBuilding the Capacity to Educate the California Nursing WorkforceDeloras Jones, Executive Director, California Institute for Nursing and Health Care3:30 pmDiscussion and Closing Remarks4:00 pmAdjourn
The Nursing Shortage inCaliforniaJoanne Spetz, Ph.D.University of California, San FranciscoAugust 20051
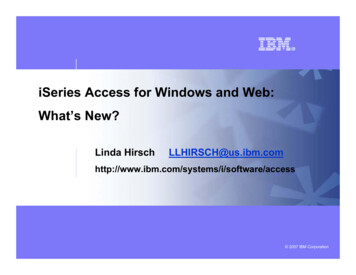
Projected supply and demandof RNs in California4000003500006,872 - 10000050000SupplyDemand - lowDemand - highDemand - Dept of 027202902
How bad is the shortage now?2004 survey data 1 monthago1 yearagoA surplus of RN resources, requiring cancellations, and/orlayoffs1.5%1.3%Adequate RN resources in all clinical areas3.6%2.7%A mild RN shortage: RN shortages on some shifts inlimited clinical areas41.0%28.2%A moderate RN shortage: RN shortages in many clinicalareas16.8%44.3%A severe RN shortage: RN shortages across entire facility14.8%18.8%Source: Survey of Chief Nursing Officers conducted by Hospital Association of SouthernCalifornia, California Institute on Nursing and Health Care, and UCSF3
Why is this happening? Supply issues: Fewer people chose nursing over past 20 yearsImpending retirements of baby-boom nursesLack of space to educate nursesLoss of nurses to other professionsDemand issues: Increasing populationAging of patients and higher acuityGreater attention to nursing’s effect on quality ofcare4
What can we do? Short-term solutions Hire traveling nurses – filled 4,408 full-timeequivalent jobs in 2004Recruit immigrants – 3,684 in 2002-2003Recruit inactive nurses back to nursing –improve working conditionsIncrease work hours of those now workingReduce health care services provided5
What can we do? Long-term solutions Expand nursing education programsIncrease efficiency of nursing programsIncrease diversityRetain nurses now licensed6
Use of short-term solutions,20041 month ago1 year agoOvertime/extra shifts94.0%92.7%Temporary agency80.1%78.1%Travelers76.8%70.2%Temporary limit of clinical services22.5%17.2%Permanent closure of services1.3%2.0%Source: Survey of Chief Nursing Officers conducted by HospitalAssociation of Southern California, California Institute on Nursing andHealth Care, and UCSF7
Costs of short-term solutions Hospitals have an average of 20 travelingnurses to handle vacancies Average cost: over 3 million per hospital40% are actively recruiting foreign nurses Average cost: 15,0008
Can we recruit domestically? Recruitment from other states Permanent migration into California estimated at3,179 to 7,270Permanent migration out of California estimatedat 4,323 to 9,307Return of inactive nurses BRN data on nurses who change from inactive toactive license: 303 in 2003-20049
Shares of nurses who work We’re not likely to getmuch more work fromthe nurses we havenow!age group% whoworkhours/week 78.7%35.665 55.4%27.110
To improve long-term supply: Expand nursing education programsIncrease efficiency of nursing programsIncrease diversityRetain nurses now licensed11
Increase funding to nursingeducation Number of new California RN graduates inthe 2003-2004 year: 6,158Strategies to expand education programs Grants from government and industryContract education from hospitalsDistance education12
Improve efficiency of nursingeducation For the 2000-2001 graduating class: NCLEX first-time pass rates: average 84% 20% of students delayed but still enrolled22% of students left without completingRange: 25% to 100%Strategies Scholarships and loansChildcare and transportation assistanceSkills assessments and tutoringNCLEX exam preparation13
Increase diversity of nursing Nursing cannot grow ifonly white women arerecruitedMinorities and men aremore likely to work fulltimeDemographics of newgraduates, 2003-20048%8%10%44%11% In 2003-2004, 14%male icanOther/unknown14
Retain nurses Compensation must be good Large wage increases over past 6 yearsBenefits are part of compensation Creative ideas such as pensions with phasedretirement optionsWorking conditions must be good Staffing levels“Mandatory” overtimeErgonomicsSupportive culture15
Policies now underway toaddress the shortage Government Industry Contract educationGrants to education programsLabor Workforce Investment Act moneyDirect education spendingPreceptor programsCareer ladders with industryFoundations16
Workforce Investment Act Nurse Workforce Initiative, 2002-2005 28 million from WIA 29.7 million in-kind contributions22 sites1,878 new slots created (most temporary)1,522 students received financial support & case managementSpecific new grants announced in past yearNurse Education Initiative, 2005-2010 30 million from WIA 30 million from industry 30 million from ?17
Industry, labor & foundationefforts Millions of dollars donated by hospitals Unions are active in growing the workforce 93% of hospitals have relationships with nursingprogramsShirley Ware Education Center & SEIU-KaiserCalifornia Nurses Foundation preceptor programFoundations are supporting many projects18
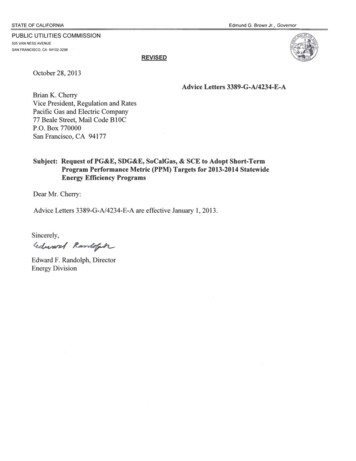
The nursing shortage is worsein some regions2004licensedRNs400-500 RNs/100,000500-650 RNs/100,000650-800 RNs/100,000800-1000 RNs/100,000Under 400RNs/100,000Blue is bestGreen is goodYellow & orange are middleRed and brown are worstMore than 1000RNs/100,00019
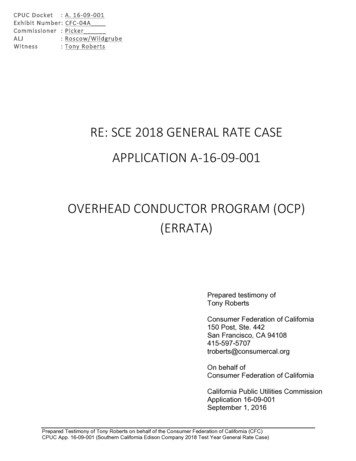
Improvements vary by region0 to 3% change- 4% to - 2% change- 2% to no change 5% to 7% change 7% to 9% change 10% change or greater 3% to 5% changeChange1999-2004- 4% change or greater20
Minimum staffing rules havenot had uniform effect Los Angeles & Central Valley had worsestaffing in 2000 Southern California hospital markets are morecompetitiveCenter for Studying Health System Changereports stress in Orange CountyKaiser, CHW, UC have embraced ratios21
Thoughts About the Future There are enough people interested innursing Nearly all nursing programs have more applicantsthan slotsNearly all programs have waiting lists or lotteries22
Thoughts About the Future There is not enough educational capacity Slots have expanded 10% and will shrink if newfunding not securedInnovative programs to consider: Distance learning (Bakersfield College model)On-site education for career ladders (RiversideCounty)Contract education (Sutter, Fresno City College)Labor-management partnerships (Shirley WareEducation Center)23
What do we need next? Assessment of policy goals How much do we care about averting a healthcare crisis?How much do we care about job opportunities forCalifornians?Research on effects of Supply-increasing programsMinimum staffing ratiosOther innovations in the workplace24
Visit us on the com/joanne25
Hospital Nurse Staffing:Today and TomorrowCalifornia Nurse Shortage: Impact of NurseEducation and Training InitiativesSacramento, CaliforniaAugust 23, 2005Dorel Harms, MS, RN, FACHEVice President, Professional ServicesCalifornia Hospital Association
We can all agree there is a shortage Shortage is national/internationalIn California, ratios regulations haveexacerbated shortage 14,000 open positions, according to January 2005survey“At all times” is biggest issue 1:6 equals 1:5.051:5 equals 1:4.21CHA 2
CHA Survey ResultsJan-Jun 2004Data Summary ReportWeeks of01/05/04 – 06/28/04Weeks of06/28/04 - 07/05/04Total Records in Sample66452301.0Take beds out of service or closeentire unit or service -- Any Unit orServiceYes 32%No 68%N 6625Yes 26%No 74%N 2302.0ED went on diversion, orrequested to do soYes 38%No 62%N 4178Yes 29%No 71%N 1393.0Average ED wait time comparedto similar week last yearLonger 36%About the same 58%Shorter 6%N 4895Longer 33%About the same 61%Shorter 7%N 1664.0Ratio requirements always met -in Every Unit, Every ShiftAlways 15%Not Always 85%N 6626Always 14%Not Always 86%N 2275.0Approximate number surgeriespostponedAverage 0.16N 963Average 0.11N 236.0Unable to transfer patients fromEDYes 26%No 74%N 5168Yes 18%No 82%N 1706.1Due to inability to meet ratiosYes 57%No 43%N 748Yes 36%No 64%N 22And, this was before1:5 in unitsmedical/surgicalCHA 3
Closed or DowngradedPsychiatric Inpatient Beds in Los Angeles CountySince January 2004In 2003 there were 3,563 Total Licensed Beds in Los Angeles County*ClosedDowngradedTotalCedars Sinai Medical Center17 (51 beds remain)-San Gabriel Valley Medical Center42-Presbyterian Intercommunity Hospital-10 (LPS to Voluntary)California Hospital Medical Center13-St. Mary Medical Center23-Century City Hospital41-Glendale Memorial Hospital & Health Center-49 (LPS to Voluntary)Northridge Hospital Medical Center, Sherman Way44-Robert F. Kennedy Medical Center43Total Closed or Downgraded in 200422359282Total Remaining3,340* 2002-2003 OSHPD DataCHA 4
Hospital Closures in California2004Date ofClosureOSHPDID No.Name of HospitalCityCountyLicensedBeds01/09/04190691Santa Teresita HospitalDuarteLos Angeles03/16/04364188Angels HospitalRanchoCucamongaSan Bernardino04/30/04190155Century City HospitalLos AngelesLos Angeles18605/26/04190541Monrovia HospitalMonroviaLos Angeles49Closed07/02/04100791Central Valley Orthopedic & SpineInstSangerFresno31Closed (Formerly Sanger)08/09/04190685Elastar Community HospitalLos AngelesLos Angeles110BasicClosed (Formerly Santa Marta)11/16/04190810Northridge – Sherman WayCampusVan NuysLos Angeles209BasicClosed12/09/04160366Robert F. Kennedy Medical CenterHawthorneLos Angeles274BasicClosed12/09/04430879San Jose Medical CenterSan JoseSanta Clara328BasicClosed216LicensedER LevelCommentsBasicBecame a Skilled NursingFacility55Closed by State of Calif DHSBasicClosed – may be re-opening inAprilCHA 5
RN Demographics(California)Supply California ranks 49th in the nation RNs/population. 585 RN’s per capita/average 798. 87% of RN’s working in nursing. Average Age 47; 30% over 50. 44% of the faculty are over 50. Less than 6,000 new grads per year.Demand CA will need 116,000 additional RN’s by 2020 (Governor’s Office). CA pop growth of 17 mil by 2025, highest in nation – internationalmigration.CHA 6
Outgoing & IncomingEndorsements History(CalStars Reports)Year endprojection basedon first 8 mosOUTGOING ENDORSEMENTS HISTORY(CalStars Reports)FISCAL YEAR 1991/92 1992/93 1993/94 1994/95 1995/96 1996/97 1997/98 1998/99 1999/00 2000/01 2001/02 2002/03 938,2778,58910,4548,147TOTALINCOMING ENDORSEMENTS HISTORY (CalStars Reports)FISCAL YEAR 1991/92 1992/93 1993/94 1994/95 1995/96 1996/97 1997/98 1998/99 1999/00 2000/01 2001/02 2002/03 259,45110,25210,5859,629TOTALDIFFERENCE OF RNs INTO STATE VERSUS RNs 858321,1741,6631311,482CHA 7
“AND, these numbers do not reflect: RNs from other states who obtain California licensesand stay temporarilyRNs allowing their licenses to expireRNs who die or retireInternational RNs who obtain California licenses aspass-thru (No CGFNS required)RNs who maintain California license but live inanother stateCHA 8
What are hospitals doing to increasethe number of nurses?A Compendium of Innovative Practices and Partnerships:Expanding Educational Capacity in California Schools of NursingPartnership ProgramsRN ADNRN BSNRN MastersBSN CompletionGraduate307235Cost of over 53 million annually.CHA 9
The Financial Perspective Annual cost of ratios to California hospitals Estimated – 453 millionActual – More than 1 billion2003 California hospitals Patient Revenue: 44.1 billionOperating Expense: 44.4 billion - .76% operating margin statewide 2004 California hospitals Patient Revenue: 47.1 billionOperating Expense: 48.1 billion - 2.07% operating margin statewideBased on OSHPD quarterly financial dataCHA 10
All California Hospitals Cannot sustain the level of financial commitmentmeet the increasing demands of ratios (2008)compete for RNs as salaries/benefits continueto riseWhere will it end?!?CHA 11
CHA 12
CaliforniaNursing Education Initiative
“Nurses are people of compassion and courage. Theirprofession is a labor of love and without them wesimply could not deliver quality care for patients.California is facing a severe nursing shortage and it isabsolutely critical that we open up the nursingprofession to everyone who has the passion andpotential.”-Governor Arnold SchwarzeneggerApril 13, 2005
Nursing Education Initiative The Problem The Solution The Task Force
Nursing Education InitiativeThe ProblemCalifornia’s major challenge is to expandeducational capacity in nursing programs Nursing programs are at capacity, and an averageof 40 percent of applicants are denied admissioneach year A lack of clinical lab space, classrooms andqualified faculty contribute to the limitededucational capacity California’s nursing programs graduate nearly6,000 nurses per year and will need to graduate atleast 9,000 more annually to meet demand
Nursing Education InitiativeThe ProblemA growing and aging population will increase thenursing shortage in the coming years The elderly population in California will continueto grow rapidly in the next thirty years. The number of Californians over the age of 65 will increasefrom 3.7 million in 2000 to 6.3 million in 2020. California’s RN population is also aging. The average age an RN in California is 47.7 years, which is5 years higher than the national average.
Nursing Education InitiativeThe SolutionThe Governor’s Nursing Education Initiative1. Help public colleges and universities expandeducational capacity2. Partner with private industry to build morenursing programs3. Recruit more qualified instructors4. Develop new avenues to nursing careers5. Seek additional funds for nurse education fromthe federal government and other funding sources
Nursing Education InitiativeThe Solution 1. Expand Educational CapacityThe Administration has partnered withCommunity Colleges to expand capacity innursing programs 90 million distributed over five years andthe cost is shared three ways: 30 million from Governor’s WIA 15% discretionaryfund 30 million from community colleges 30 million from private industry or foundations
Nursing Education InitiativeThe Solution2. Partner with Private Industry The Administration allocated 750,000 tohelp local public/private partners createregional clinical simulation labs This will fund the creation of 3 clinicalsimulation labs in rural areas Additional Baccalaureate Level Programsare needed
Nursing Education InitiativeThe Solution3. Recruit Nursing Instructors The Administration allocated 150,000 to establish a statewideloan forgiveness programMasters of Science in Nursingand PhD students will be eligiblefor loan forgiveness if they agreeto teach in a California nursingprogram
Nursing Education InitiativeThe Solution4. Develop new avenues to nursing careers The Administration supportscreating innovative ways to prepareindividuals for nursing careers Several projects are underconsideration, including:– Nursing Academies– Preparing medically trained veteransfor nursing careers
Nursing Education InitiativeThe Solution5. Seek additional funding sources Seeking changes in federal requirementsfor Workforce Investment Act funds thatmay limit nurse education expansion Seeking additional funds for nursingeducation from the federal government andprivate foundations
Nursing Education InitiativeThe Task ForceThe Governor issued an Executive Order to create anon-going taskforce to oversee implementation of theFive-Point Plan. The Taskforce consists of a Chair, aswell as the Secretaries from the following Agencies &Offices: Health & Human ServicesLabor & Workforce DevelopmentState & Consumer ServicesSecretary of EducationPresident, University of CA SystemChancellor, CA State University SystemChancellor, CA Community Colleges
Nursing Education InitiativeAdditional State Nursing Projects Workforce Investment Act Governor’sDiscretionary 15% grants 13.2 million allocated to local workforceinvestment areas, educational institutions andcommunity-based organizations in March 2005 An additional 8 million was released in August2005 to support the education of LVNs and RNs
Nursing Education InitiativeAdditional State Nursing Projects 10 million allocated to CommunityColleges in 2005-2006 budget One time allocation from Prop 98 funds toexpand enrollment capacity 560,000 allocated to California StateUniversity to supplement Entry-LevelMasters in Nursing programs
FutureGovernor’s Nursing Education Task Forcewill stay on task: UCCSUCCCPrivate SectorTime for Action is now
“Building Education Capacity”CPAC Forum: CA Nurse ShortageCalifornia Institute forNursing & Health CareAugust 23, 2005
California Institute for Nursing &Health Care What is it?A nonprofit independentorganization established to providea forum for diverse stakeholders toaddress state-wide nursing issuesthat impact the health ofCalifornians.
About CINHC Established by a group of nurses representingvaried interest, with a common concern aboutthe lack of comprehensive, strategic planningfor nursing shortageIncorporated December 2001Programs began 2004Funded by contributions and grantsEndorsed by 30 organizations
What is CINHC Doing? Building a coalition of stakeholders representing thestate’s varied voicesDeveloping a master plan for the nursing workforceProviding a “home” for nursing initiativesConvening, facilitating, serving as a catalyst for actionLinking efforts underway to implement the master planFocusing on improving the health of Californiansthrough nursing’s contributions
Nurse Shortage:California Nursing Workforce 297,039 RNs with Active California licenses–– 40,000 increase over 4 years14.3% (42,000) reside outside California87% working in California (223,000 RNs)Average age: 47.7 years45% educated outside CaliforniaCalifornia ranks next to last in RNs per capita–544 California, 782 national average
Nurse Shortage:Demand for Nurses Hospitals reporting 11 to 15% vacancy ratesCalifornia EDD projected need for nearly 110,000 newnurses between 2000 and 2010 to replace thoseretiring and for meeting population growth demandHRSA forecasts by 2010 demand will be 47,600 morethan supply 24% short fallHRSA forecasts by 2020 demand will be 116,000 morethan supply 45% short fall
Nurse Shortage:Educational Pipeline California schools have capacity to educate only ½ ofnurses neededSchools have increased capacity 10% in last 5 years,yet ability to educate nurses no better than in 1995Most of increase has been through hospitalscontributions to educationAttrition rates between 20% to 26%Less than 40% of qualified applicants are admitted
Nurse Shortage:What Must Be Done? Nursing shortage is not effectively beingaddressed there is lack of centralized andcomprehensive strategic planningCalifornia needs a statewide MASTER PLANfor the nursing workforce that:–––Defines where we’re goingCharts a course for getting thereProvides the markers along the way
Without a Master Plan: Growing and aging population compoundseverity of the shortageInsufficient numbers of qualified nursesavailable to replace those leaving workforceFaculty shortages worsenSchools in constant crisis modeLose critical cohort of motivated studentsNursing’s image as a career suffers
Without a Master Plan (cont): Unlinked projects result in fragmentation and risk ofduplication or competition for scarce resourcesFunding decisions made without best ROIGaps of unmet needs widenQuality & safety of patient care at riskAccess to care decreases, with greatest impact felt inthe underserved and underrepresented populationsCost of staffing inpatient care growsDivergent/competing voices politicize decision makingUnproductive spiral continues, leading to health crisis
Master Plan: OPPORTUNITIES Create a framework for planning, that iscomprehensive and strategically driven––– Across the continuumNurses with other healthcare providersInnovations that create a future based on new realitiesMove short-term interventions into long-term sustainingsolutionsProvide a roadmap for planners, funders, and policyand decision makersBuild upon and link work underwayIdentify, share, and replicate successful practices
Master Plan: OUTCOMES Balance the demand with the supplyIncrease capacity in schools of nursingIncrease workforce, with educationalpreparation neededBuild consensus create a COMMON VOICEfor addressing shortageShape the future of nursing
Master Plan: FOCUSED AREAS DATADIVERSITYEDUCATIONNURSING PRACTICERECRUITMENTWORK ENVIRONMENT
Goal 1: Building Educational Capacity July 2004 Workshop Identified barriers toexpanding eAttritionPre-requisites
Goal 1: Building Educational Capacity Nov 22-23, 2004 Workshop Action Steps toOvercome Barriers Developed became Goal 1Broad-base representation developed planShared with policy makers and others engaged inworkforce planning –––Governor’s PlanRegional planning effortsLegislators
Goal 1: Building Educational CapacityNext Steps Entities assuming responsibility for Action Steps,including Governor’s officeResponses to Chancellor’s Office RFAs beingdevelopedRegional efforts underwayCollaborate with policy makersLink efforts together, identify gaps; develop strategiesto close gapsData analysis that defines extent of shortage anddemand by region
Goal I: Building Educational CapacityObjective 1: Increase Funding Strategy 1: Set targets for expanding capacitythrough 2010; identify high shortage regionStrategy 2: Establish new funding initiativesStrategy 3: Create new schools of nursingStrategy 4: Establish fast track BSN programs
Goal I: Building Educational CapacityObjective 2: Increase Faculty Strategy 1: Set targets for increasing facultyStrategy 2: Establish increasing faculty as aCalifornia priorityStrategy 3: Address faculty salariesStrategy 4: Support students to becomefaculty provide incentivesStrategy 5: Address Education Coderegulations that create barriers
Goal I: Building Educational CapacityObjective 2: Increase Faculty (cont) Strategy 6: Expand ADN to BSN articulation,ease of transferring from CCC to CSU, andaccess to higher education for ADN graduatesStrategy 7: Increase number of programspreparing facultyStrategy 8: Share faculty amongst collegesStrategy 9: Provide for faculty development
Goal I: Building Educational CapacityObjective 3: Increase infrastructure Strategy 1: Implement alternate educationalvenues––––––Promote collaboration amongst schoolsOn-line, video conferencingClinical simulation labsSharing facultyWeekend/evening programsYear round programs
Goal I: Building Educational CapacityObjective 3: Increase Infrastructure (cont) Strategy 2: Implement web-based solutions to accessclinical sitesStrategy 3: Expand educational capacity/redesignnursing education through use of clinical simulationStrategy 4: Increase access to prerequisite coursesStrategy 5: Expedite approval of new programsStrategy 6: Increase access to nursing programs inunderserved areas
Goal I: Expanding Education CapacityObjective 4: Decrease attrition, improveNCLEX Scores Strategy I: Encourage use of model curriculumfor schools with low NCLEX scoresStrategy 2: Increase access to prerequisitesStrategy 3: Improve completion ratesStrategy 4: Provide NCLEX prep courses
Other CINHC Master Plan/Goal 1Activities Underway Consolidated BRN School Survey Oct 2005Regional Report Card Project Sept 2005Compendium Innovative Practices and PartnershipsBay Area Regional Shared Services:––– Computerized Clinical Placement SystemFaculty Resource CenterRegional Clinical Simulation CentersBRN Ed Program for clinical/adjunct faculty - September 23, 2005Diversity GrantHospital Survey December 2005
Contact InformationDeloras Jones, RN, MSExecutive Director1815 B Fourth StreetBerkeley, CA 94710(510) 486-0627deloras@cinhc.orgwww.cinhc.org
3:10 pm Building the Capacity to Educate the California Nursing Workforce . Deloras Jones, Executive Director, California Institute for Nursing and Health Care . 3:30 pm Discussion and Closing Remarks . 4:00 pm Adjourn . CALIFORNIA PROGRAM ON ACCESS TO CARE California Policy Research Center . University of California, Office of the President