Transcription
This report may be used, in whole or in part, as the basis for development of clinical practiceguidelines and other quality enhancement tools, or a basis for reimbursement and coveragepolicies. AHRQ or U.S. Department of Health and Human Services endorsement of suchderivative products may not be stated or implied.AHRQ is the lead Federal agency charged with supporting research designed to improve thequality of health care, reduce its cost, address patient safety and medical errors, and broadenaccess to essential services. AHRQ sponsors and conducts research that provides evidence-basedinformation on health care outcomes; quality; and cost, use, and access. The information helpshealth care decisionmakers—patients and clinicians, health system leaders, and policymakers—make more informed decisions and improve the quality of health care services.i
Systematic Evidence ReviewNumber 21Screening and Interventions for Overweight andObesity in AdultsPrepared for:Agency for Healthcare Research and QualityU.S. Department of Health and Human Services540 Gaither RoadRockville, MD 20850http://www.ahrq.govContract No. 290-97-0011Task No. 3Technical Support of the U.S. Preventive Services Task ForcePrepared by:Research Triangle Institute3040 Cornwallis RoadP.O. Box 12194Research Triangle Park, NC 27709Kathleen McTigue, MD, MPHRussell Harris, MD, MPHM. Brian Hemphill, MDAudrina J. Bunton, BALinda J. Lux, MPASonya Sutton, BSPHKathleen N. Lohr, PhDDecember 2003i
PrefaceThe Agency for Healthcare Research and Quality (AHRQ) sponsors the development ofSystematic Evidence Reviews (SERs) through its Evidence-based Practice Program. Withguidance from the U.S. Preventive Services Task Force (USPSTF) and input from Federalpartners and primary care specialty societies, the Evidence-based Practice Center at the OregonHealth Sciences University systematically review the evidence of the effectiveness of a widerange of clinical preventive services, including screening, counseling, and chemoprevention, inthe primary care setting. The SERs—comprehensive reviews of the scientific evidence on theeffectiveness of particular clinical preventive services—serve as the foundation for therecommendations of the USPSTF, which provide age- and risk-factor-specific recommendationsfor the delivery of these services in the primary care setting. Details of the process of identifyingand evaluating relevant scientific evidence are described in the “Methods” section of each SER.The SERs document the evidence regarding the benefits, limitations, and cost-effectiveness of abroad range of clinical preventive services and will help further awareness, delivery, and coverage ofpreventive care as an integral part of quality primary health care.AHRQ also disseminates the SERs on the AHRQ Web site(http://www.ahrq.gov/clinic/uspstfix.htm) and disseminates summaries of the evidence (summaries ofthe SERs) and recommendations of the USPSTF in print and on the Web. These are available throughthe AHRQ Web site and through the National Guideline Clearinghouse (http://www.ncg.gov).We welcome written comments on this SER. Comments may be sent to: Director, Center forPractice and Technology Assessment, Agency for Healthcare Research and Quality, 540 Gaither Road,Suite 3000, Rockville, MD 20850.Carolyn Clancy, M.D.DirectorAgency for Healthcare Reseach and QualityJean Slutsky, P.A., M.S.P.H.Acting Director, Center for Practice andTechnology AssessmentAgency for Healthcare Research and Quality The USPSTF is an independent panel of experts in primary care and prevention first convened by the U.S. PublicHealth Service in 1984. The USPSTF systematically reviews the evidence on the effectiveness of providing clinicalpreventive services--including screening, counseling, and chemoprevention--in the primary care setting. AHRQconvened the USPSTF in November 1998 to update existing Task Force recommendations and to address newtopics.i
i
AcknowledgmentsThis study was supported by Contract 290-97-0011 from the Agency of HealthcareResearch and Quality (Task No. 3). We acknowledge at AHRQ the continuing support ofJacqueline Besteman, JD, MA, Director for the Evidence-based Practice Center program; DavidAtkins, MD, MPH, Chief Medical Officer of the AHRQ Center for Practice and TechnologyAssessment; and Jean Slutsky, PA, MSPH, the Task Order Officer for this project. We wouldalso like to acknowledge the guidance and assistance from our US Preventive Services TaskForce liaisons, Janet Allan, PhD, RN, CS, FAAN and Mark Johnson, MD, MPH.The investigators deeply appreciate the contributions of Loraine Monroe at RTI, forsuperior secretarial assistance. In addition, we are indebted to Timothy S. Carey, MD, MPH,Co-Director of the RTI-UNC Evidence-based Practice Center at the University of North CarolinaCecil G. Sheps Center for Health Services Research.We also owe our thanks to the following external peer reviewers, who providedconstructive feedback and insightful suggestions for improvement of this systematic evidencereview: David Arterburn, MD, University of Washington, Seattle, WA; James D. Douketis, MD,McMaster University, Hamilton, Onatario, Canada; Evelyn L. Lewis-Clark, MD Bowie, MD,representing the American Academy of Family Physicians; F. Xavier Pi-Sunyer, MD, MPH, StLuke’s/Roosevelt Hospital Center, New York, NY; Walter J. Pories, MD, East Carolina Schoolof Medicine, Greenville, NC; Bruce A. Reeder, University of Saskatchewan, Saskatoon, Canadaand representing the Canadian Task Force on Preventive Health Care; and Vincenza Snow, MD,American College of Physicians-American Society of Internal Medicine, Philadelphia, PA.vi
Structured AbstractBackgroundObesity, a condition characterized by excess body fat, carries substantial healthimplications for both chronic disease and mortality. This fact and its increasing prevalence makeobesity an important health problem.PurposeTo examine the evidence of the benefits and harms of screening and earlier treatment inreducing morbidity and mortality from overweight and obesity.Data SourcesWe developed an analytic framework and 6 key questions that represent a logical chainbetween screening and sustained weight reduction and reduced morbidity and mortality. Wesearched MEDLINE from January 1, 1994 (the end date for prior USPSTF searches), to July 31,2001, using the Medical Subject Heading obesity and overweight and combining this term withpredefined strategies to identify relevant English-language studies. We also searched theCochrane Library, contacted experts, and scanned review bibliographies. We found 4 recent,well-conducted systematic reviews and relied on their analyses of the studies they included.vii
Study SelectionWe included: (1) large, population-based surveys of the prevalence of overweight andobesity; (2) randomized controlled trials (RCTs) with at least 1 year follow-up (6 months forpharmacological studies) reporting weight reduction or health outcomes for treatment and harmsquestions. The shorter follow-up period for pharmacological studies was driven by the availableliterature: weight loss trials were frequently only of 6 months’ duration but were complementedby studies designed specifically to evaluate maintenance of that loss. When we found few or noRCTs, we examined cohort studies concerning the efficacy or harms of treatment. Tworeviewers examined all abstracts and articles to determine which met inclusion criteria.Data ExtractionTwo reviewers abstracted relevant information from each article, using standardizedabstraction forms. We graded the quality of all included articles according to criteria establishedby the U.S. Preventive Services Task Force.Data SynthesisNo RCT of screening for obesity has been performed. Obesity is most commonlymeasured as body mass index (BMI, weight in kilograms [kg] divided by height in meterssquared). Although other measures have been developed, BMI is the most consistently used inthe literature, and so we focused on it as the preferred screening tool. The prevalence of obesity(BMI 30) has been increasing; currently; at least 27% of the adult population is obese. Theprevalence of overweight (BMI 25-29.9) is about 34%. Among people with BMI of about 30 orvii
greater, intensive counseling and behavioral treatment for obesity is effective in reducing meanweight by about 3 kg to 5 kg after 1 year. Pharmacotherapy with sibutramine or orlistat is alsoeffective in reducing mean weight by about 3 to 5 kg. For people with BMI of 35 or greater,surgical therapy leads to dramatic reductions in weight of 20 kg or more.Both counseling-based and drug-based maintenance interventions were helpful inretaining weight loss. Weight reduction of 5% to 7% body weight is associated with lowerincidence of diabetes, reduced blood pressure, and improved dyslipidemia. Larger weight losshas been linked with more dramatic improvements in glycemic control and lipids in limitedsurgical outcomes data.We did not find evidence evaluating potential harms of counseling-based interventions.Sibutramine is sometimes associated with increased blood pressure (mean increase of 0-3.5 mmHg); orlistat causes gastrointestinal distress in 15% to 37% of people taking the drug. Surgicalprocedures lead to mortality in less than 1% of patients in pooled samples, but in up to 25%patients re-operation is necessary over 5 years.ConclusionsScreening with BMI would detect a large percentage of adults who are obese oroverweight. Limited evidence suggests that counseling interventions may promote modestweight loss in the overweight (BMI 25-29.9). Effective treatments for people with BMI 30include intensive counseling and behavioral interventions for lifestyle change, andpharmacotherapy. Surgery is effective in reducing weight for people with BMI of 35 or greater.Adverse effects include increased blood pressure and gastrointestinal distress with drugs and asmall percentage of serious side effects with surgeryviiiviii
Table of ContentsixContentsSystematic Evidence ReviewChapter 1. Introduction .1Background .1Cost of Obesity and Overweight . 5Prior Recommendations About Obesity Screening. 6Organization of This Review. 7Chapter 2. Methods. 13Analytic Framework and Key Questions .13Analytic Framework .13Key Questions. 14Literature Search Strategy and Synthesis . 14Search Terms . 14Inclusion and Exclusion Criteria. 15Article Review and Data Abstraction. 15Preparation of this Systematic Evidence Review . 16Chapter 3. Results . 21Key Question No. 1: Does Screening for Overweight and Obesity Affect Health Outcomes? . 21Key Question No. 2: What is the Prevalence of Overweight and Obesity? . 21Key Question No. 3: Is There a Reliable and Valid Screening Test?. 22Key Question No. 4a: Do Any Interventions Lead to Sustained Weight Reduction? . 24Counseling and Behavioral Interventions. 24Pharmacotherapy Interventions . 31Surgical Approaches . 37Key Question No. 4b: Do Interventions Improve Other Intermediate Health Outcomes?. 40Key Question No. 5: Do Interventions Improve Final Health Outcomes?. 43Key Question No. 6: What are the Harms of Screening and Treatment?. 44Screening or Counseling and Behavioral Interventions. 44Medications. 44Surgical Approaches . 46Chapter 4. Discussion . 51General Conclusions. 51Cross-cutting Findings and Future Research Issues . 53References. 58AppendicesAppendix A. Evidence Tables . A-1Appendix B. Counseling Intervention Descriptions.B-1Appendix C. Descriptions of Intensive Counseling and Behavioral Intervention Studies .C-1ix
Table of ContentsxFiguresFigure 1.Figure 2.Figure 3.Figure 4.Figure 5.Figure 6.Figure 7.Figure 8.Cardiovascular Morbidity in Men.9Cardiovascular Morbidity in Women .10All-cause Mortality in Men: Studies with Race Differentials .11All-cause Mortality in Women: Studies with Race Differentials .12Analytic Framework: Screening and Interventions for Overweight and Obesityin Adults.20Differences in Mean Weight Loss between Intervention and Control Groups forCounseling and Behavioral Interventions.48Differences in Mean Weight Loss Between Intervention and Control Groups forPharmacotherapy Interventions .49Frequency of 10% Weight Loss for Pharmacotherapy Interventions (Sibutramineand Orlistat) .50TablesTable 1.Table 2.Table 3.Table 4.Ranges of Body Mass Index with Minimal Absolute Risk for Mortality inMen and Women.8Screening for Obesity: Key Questions.17Screening for Obesity: Inclusion Criteria and Results of Searches .18Summary of Findings from Prior Systematic Reviews and Our Updated Searchesof Obesity Treatment Efficacy.19x
Table of Contentsxixi
Structured Abstract1. IntroductionBackgroundObesity, a condition characterized by excess body fat, carries significant healthimplications for both chronic disease and mortality. In the setting of escalating prevalence, theimportance of obesity as a health problem in the United States is increasingly evident – asemphasized by the recent Surgeon General’s “Call to Action to Prevent and DecreaseOverweight and Obesity.”1Obesity is usually defined in terms of the body mass index (BMI, calculated by dividingkilograms of weight by meters of height squared), which is a measure of weight adjusted forheight. Although numerous techniques are available for evaluating body fat, the variables forBMI are easy to measure. BMI has been shown to correlate closely with body fat content inadults and children.2Adults with a BMI of 25 to 29.9 are identified as overweight and those with a BMI 30as obese. These cutoffs are based on epidemiologic evidence of discernible, then substantial,increases in mortality.3 For example, if a 5'6" women weighs 155 pounds, her BMI is 25(overweight); if she weighs 186 pounds, her BMI is 30 (obese). BMI calculations can betedious, so electronic BMI calculators (eg, from the National Institutes of Health [NIH],http://www.nhlbisupport.com/bmi/) or tables of BMI by height and weight (eg, from i tbl.htm) may be useful tools for clinicians andpatients. Waist circumference and the waist-to-hip ratio are common adjuvant measures used to1
Structured Abstractclassify the distribution of body fat in people who are overweight, as obesity-relatedcomplications are most closely correlated with abdominal fat distribution.4-62
Chapter 1. BackgroundThe prevalence of obesity is increasing. Data from the National Center for HealthStatistics show that, over the past 40 years, obesity prevalence increased from 13% to 27% of theU.S. adult population; the prevalence of the less severe overweight category increased from 31%to 34%.7,8 Concurrently, a rise in prevalence of obesity has been noted in adolescent andpediatric populations.9,10 Self-report data from the Behavioral Risk Factor Surveillance Survey(BRFSS) show the increase in prevalence continuing into the year 2000.11Obesity prevalence is higher in women; overweight is more common in men.7 Obesity isespecially common in certain minority ethnic groups, including African Americans, someHispanic populations, Native Americans, and Native Hawaiians.All classes of excess body weight have substantial prevalence among U.S. adults. In theNational Health and Nutrition Examination Survey III (NHANES III, 1988-1994), theprevalence of BMI 25 to 29.9 was 44% for people ages 55 years and older and 41% for peopleages 25 to 54.9 years.12,13 For these older (55 years of age and older) and younger (25-54.9years) groups, the prevalence of BMI 30 to 34.9 was 18% and 14%, respectively. Theprevalence of BMI 35 to 39.9 was 4% and 3%, respectively, and for BMI 40 or above, 1% and2%.Obesity is a risk factor for major causes of death, including cardiovascular disease, somecancers, and diabetes. Obesity has also been linked with many sources of morbidity, includingosteoarthritis, gall bladder disease, sleep apnea, and respiratory impairment. Excess weight is arisk factor for cancers of the colon, rectum, prostate, gall bladder, biliary tract, breast, cervix,endometrium, and ovary.2 It is associated with concerns of quality of life, including diminishedmobility and social stigmatization.142
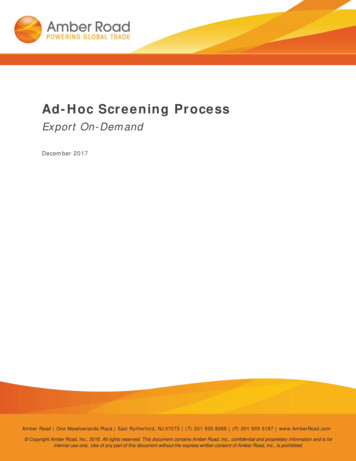
Chapter 1. BackgroundMost studies have found that mortality assumes a J-shaped or U-shaped relationship withBMI, with elevated risk at low BMI being attributable, at least in part, to the effect of smoking orconcurrent disease. The BMI associated with the lowest risk varies among studies andpopulations. For example, in our review of cohort studies with at least 10 years of follow-updata,15-26 the BMI range associated with the lowest overall mortality risk was generally withinthe “normal” BMI range for men, but in the normal-to-overweight range for women (Table 1).Risk associated with specific morbidity tends to increase more linearly with BMI than therisk associated with total mortality. This trend has been demonstrated most frequently forcardiovascular disorders, so we focus on those health outcomes in this systematic evidencereview (SER). In a study of a British cohort of men, the incidence of major coronary events was9.1 per 1,000 person-years for those with a baseline BMI of 24 to 25.9.18 By contrast, coronaryheart disease incidence in Framingham heart participants was 18 per 1,000 person-years for menwith a baseline BMI of 23.8 to 25.9.27 In both these cohorts, and in a third from Sweden,24cardiovascular risk generally increased with increasing baseline BMI for men (Figure 1). Asimilar rise in cardiovascular health risk is seen with increasing baseline BMI in cohort studies ofwomen (Figure 2).Excess body weight has been linked to increased mortality for patients up to 74 years inage. The risk lessens with age:28 however, the relationship between weight and health risk isunclear beyond that point.3,29The association between obesity and health outcomes may vary by ethnic group. Figures3 and 4 present data from 2 long ( 10 year) cohort studies that reported data on more than 1racial group.22,23 These studies suggested that the association between excess body weight andmortality may be weaker for black populations than for white. One review of these and other3
Chapter 1. Backgroundstudies found that only tentative conclusions could be reached about mortality at elevated levelsof BMI in black men, with the best evidence showing only modest increases in risk.30 Likewise,the BMI-mortality association appears weaker in black women than in white women. Theseethnic-specific studies assessed only all-cause mortality, not disease-specific mortality ormorbidity. Evidence about obesity and other outcomes for black populations and about theassociation of obesity and health outcomes in general in other ethnic groups is insufficient todraw conclusions.Weight cycling – cycles of weight loss followed by weight regain – potentially carrieshealth risk, but the relationship has not been clearly established. Weight cycling has been linkedwith increases of mortality;31-34 this association is not, however, found consistently,35 and thesestudies do not distinguish between intentional and unintentional weight loss. The evidence ismixed about the relationship between weight cycling associated with intentional weight loss (onthe one hand) and coronary artery disease risk factors (on the other). One observational studyshowed 7% lower high-density lipoprotein (HDL) cholesterol levels among women withcoronary risk factors,36 and another showed a 4-fold increased risk of hypertension (odds ratio[OR], 4.1; confidence interval [CI], 2.4 – 6.9) in Italian women.37 However, in 46,224 women ofthe Nurses Health Study II, adjusting for BMI and weight gain, mild or severe weight cyclingwas not associated with increased risk of hypertension incidence.38 Likewise, in a large cohortof men, those who weight cycled did not have smaller improvements in total cholesterol, HDL,or blood pressure compared with noncyclers.39 The psychological impact of weight cycling isalso unclear: weight fluctuation has been linked with covert hostility40 in one study and notassociated with measures of depression, stress, anxiety, and anger in another.414
Chapter 1. BackgroundCost of Obesity and OverweightFinancially, obesity incurs substantial cost. Recent analyses estimate that direct costs ofobesity are 5.7% of total U.S. health expenditures42 and 2.4% of the total health care budget ofCanada.43 A U.S.-based study looking at the impact of obesity on the cost of expected lifetimemedical care on 5 diseases (hypertension, hypercholesterolemia, diabetes mellitus, coronaryheart disease, and stroke) found that costs increased by 20% with mild obesity, by 50% withmoderate obesity, and nearly 200% with severe obesity.44At least 2 types of interventions might be considered for reducing the burden of sufferingfrom obesity: public health measures for the population at large or screening and intervention inthe individual patient’s clinical encounter. This systematic evidence review considers thequestion of efficacy and effectiveness of screening and intervention in the clinical setting.Some might ask why the issue of screening for obesity arises at all, as the diagnosis ofobesity may seem obvious. Clinicians, however, frequently do not address the issue of obesitywith obese patients. In a large national study of adults with a BMI of 30 or greater, for example,only 42% reported that their health care professional advised them to lose weight.45 Thus, byscreening we refer here to the conscious measurement of BMI by the clinician, with the purposeof addressing body weight in the clinical setting.Obesity is a difficult problem to treat. This difficulty is the main concern that led priorsystematic reviews to have reservations about screening for obesity. Our SER focuses primarilyon the efficacy of potential interventions that might be initiated within the clinical setting. Theseinterventions include counseling and behavioral therapy for calorie reduction and increasingphysical activity, pharmacotherapy, and surgical approaches.5
Chapter 1. BackgroundPrior Recommendations about Obesity ScreeningIn 1996, the U.S. Preventive Services Task Force (USPSTF) recommended periodicmeasurement of height and weight for all patients.2 Since then, 3 large systematic reviews haveexamined screening for obesity; they are evidence reports from National Institutes of Health(NIH),3 the Canadian Task Force on Preventive Health Care,46and the University of York for theUK National Health Service (NHS).47Although all 3 reviews promoted clinical attention to obesity, their specificrecommendations varied. Since their completion, the prevalence of obesity has continued toclimb precipitously, new medications have become available, and more studies have addressedthe role of weight loss on health outcomes. To assist the USPSTF in updating itsrecommendation, the RTI-UNC Evidence-based Practice Center undertook a systematic reviewof the evidence concerning screening for obesity. In our analysis, we combined the findings ofthe prior reviews with an assessment of more recent or not previously covered studies of fair togood quality.In our SER, we address screening for adult populations. Obesity in childhood andadolescence is a significant and compelling issue that requires an evidence review dedicated tothat age group.9,10 The USPSTF regards the issue as sufficiently important that it expects toreview screening for obesity in children and adolescents separately in the future.6
Chapter 1. BackgroundOrganization of This ReviewChapter 2 of the SER documents our methods. Results appear in Chapter 3; Chapter 4discusses the implications of our findings and offers suggestions about future research. Figuresand tables are found at the end of chapters where they are first called out. Appendix Aacknowledges the assistance of USPSTF liaisons to this project, the work of EPC staff, and thehelpful comments from external peer reviewers. Evidence tables are presented in Appendix B.7
Chapter 1: BackgroundTable 1.Ranges of Body Mass Index with Minimal Absolute Risk for Mortality in Men and WomenMenBMI Range2322.0-23.42323.5-24.9Calle et al, 1999 Healthy nonsmoking U.S. white menCalle et al, 1999 Healthy nonsmoking U.S. black men19Chyou et al, 1997 Japanese American men, age zu et al, 1998 NHEFS* white men, age adjustedDurazo-Arvizu et al, 1998 NHFES black men, age adjustedRosengren et al, 1999 Swedish men2422.5-25.0Shaper et al, 1997 British men, age adjusted1822.0-23.926Song and Sung, 2001 Korean men24.0-25.01524.3-25.7Sorkin et al, 1994 Seventh Day Adventist men20Wannamethee et al, 1998 British men22.0-23.9Women16Manson et al, 1995 U.S. nurses without cardiovascular disease or cancer25Folsom et al, 2000 Healthy Iowans19-21.926.2-30.21725-28.9Calle et al, 1999 Healthy nonsmoking U.S. white women2322-23.42325-26.4Laara and Rantakallio, 1996 Finnish womenCalle et al, 1999 Healthy nonsmoking U.S. black women22Durazo-Arvizu et al, 1998 NHEFS white women, age adjusted22Durazo-Arvizu, et al, 1998 NHFES black women, age adjusted23.1-25.426.6-28.8*NHEFS: National Health and Nutrition Epidemiolic Survey-I (NHANES-1) epidemiologic follow-up study.8
Cardiovascular Morbidity in MenChapter 1. BackgroundFigure 1.30Per 1000 Person YearsScreening and Interventions for Overweight and Obesity in AdultsFebruary 27, 200325201510501520253035Body Mass Index Shaper et al18 – Major coronary event in British men Shaper et al18 – Diabetes in British men Kim et al27 – Coronary heart disease in Framingham heart participants Shaper et al18 – Major stroke event in British men Rosengren et al24 – Coronary disease in Swedish men99
Cardiovascular Morbidity in WomenChapter 1. BackgroundFigure 2.30Screening and Interventions for Overweight and Obesity in AdultsFebruary 27, 2003Per 1000 Person Years2520151050152025303540Body Mass Index Colditz et al48 – Incidence of diabetes in healthy Nurses’ Health Study participants Willet et al49 – Onset of coronary heart disease in Nurses’ Health Study participants (by BMI in 1976) Kim et al27 – Incidence of coronary heart disease in Framingham heart participants Huang et al21 – Hypertension in Nurses’ Health Study participants1010
All-cause Mortality in Men: Studies with Race DifferentialsChapter 1. BackgroundFigure 3.Screening and Interventions for Overweight and Obesity in Ad
Background Obesity, a condition characterized by excess body fat, carries substantial health implications for both chronic disease and mortality. This fact and its increasing prevalence make obesity an important health problem. Purpose To examine the evidence of the benefits and harms of screening and earlier treatment in