Transcription
PThe Premium IOL Channel:itfalls &rospectsSTEVEN J. DELL, MD, COMODERATOR Medical Director, Dell Laser Consultants, Austin, Texasn C hief Medical Editor, CRSTn s teven@dellmd.comn F inancial disclosure: Consultant (Bausch Lomb, Johnson & Johnson Vision, Optical Express,Presbyopia Therapies, Tracey Technologies)GUY M. KEZIRIAN, MDn P resident, SurgiVision Consultants,Scottsdale, Arizonan F ounder, Refractive Surgery Alliancen M ember, CRST Editorial Advisory Boardn g uy1000@surgivision.netn F inancial disclosure: None acknowledgedSTEPHEN G. SLADE, MD, FACS, COMODERATORn P rivate practice, Slade and Baker Vision,Houston, Texasn E ditor Emeritus, CRSTn s gs@visiontexas.comn F inancial disclosure: Consultant (Alcon,Carl Zeiss Meditec)VANCE THOMPSON, MD, FACSn F ounder, Vance Thompson Vision, Sioux Falls,South DakotanC RST Executive Advisorn v ance.thompson@vancethompsonvision.comn Financial disclosure: Consultant (AcuFocus, Alcon,Bausch Lomb, Carl Zeiss Meditec, Johnson &Johnson Vision, Mynosys, RxSight), Equity owner(AcuFocus), Lecture fees (AcuFocus, Alcon, CarlZeiss Meditec, Johnson & Johnson Vision, Mynosys)nEXCLUSIVECONTENTFROM THEAECOS WINTERSYMPOSIUM.J. ANDY CORLEYn C ofounder, Eyeonics (now Bausch Lomb)n P artner, Flying L Partnersn F inancial disclosure: Chairman of the Board(Equinox, EyeBrain Medical, RxSight)JOHN F. DOANE, MDn P rivate practice, Discover Vision Centers,Kansas City, Missourin C linical Assistant Professor, Department ofOphthalmology, Kansas University MedicalCenter, Kansas City, Kansasn E ditor Emeritus, CRSTn j doane@discovervision.comn Financial disclosure: Consultant (Carl Zeiss Meditec,RxSight), Shareholder (Presbyopia Therapies)KENDALL E. DONALDSON, MD, MSn A ssociate Professor of Ophthalmology, Cornea/External Disease/Refractive Surgeon, andMedical Director, Bascom Palmer Eye Institute,Plantation, Floridan M ember, CRST Editorial Advisory Boardn K Donaldson@med.miami.edun F inancial disclosure: Consultant (Alcon, Bausch Lomb, Johnson & Johnson)50 CATARACT & REFRACTIVE SURGERY TODAY MAY 2018KENNETH J. ROSENTHAL, MD, FACSn S urgeon Director, Rosenthal Eye and FacialPlastic Surgery & Fifth Avenue Eye Care andSurgery, New York City, New Yorkn A ssociate Professor of Ophthalmology, Universityof Utah Medical School, Salt Lake Cityn k r@eyesurgery.orgn Financial disclosure: Honoraria and speaker support(Bausch Lomb, Johnson & Johnson Vision)BENNETT WALTON, MD, MBAn S lade & Baker Vision, Houston, Texasn d rwalton@visiontexas.comn F inancial disclosure: Consultant (Alcon,RxSight), Lecture fees (STAAR Surgical)WILLIAM F. WILEY, MDn P rivate practice, Cleveland Eye Clinic, Ohion w iley@cle2020.comnC RST Executive Advisorn F inancial disclosure: Consultant (Alcon, Bausch Lomb, Carl Zeiss Meditec, Johnson & JohnsonVision, Omega Ophthalmics)
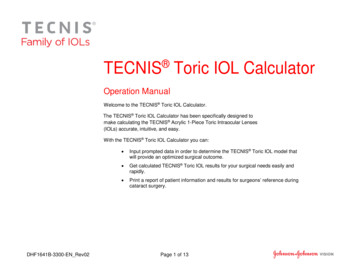
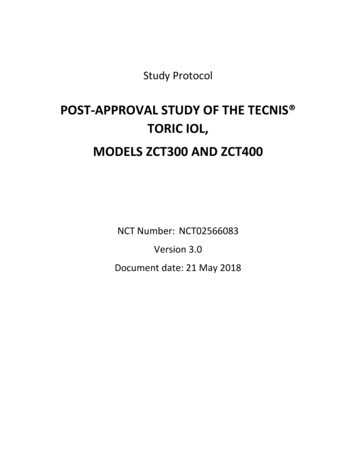
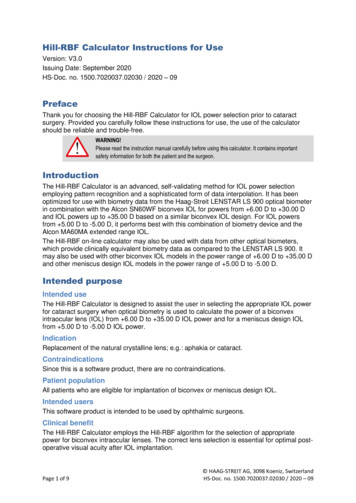
INTRODUCTIONIn February, more than 200 physicians andindustry leaders gathered in Aspen, Colorado, forthe American-European Congress of OphthalmicSurgery (AECOS) Winter Symposium and discussedtrends and innovations in ophthalmology. Thepremium IOL channel always makes the list ofhot topics. A variety of premium presbyopia- andastigmatism-correcting IOLs is available inthe United States, and many ophthalmologistsrecognize that these IOLs can offer advantages thatstandard IOLs cannot, including greater chance forspectacle independence, better visual acuity, andastigmatism correction when using toric IOLs.It remains puzzling why the market has beenstagnant (Figures 1 and 2), rising from 6.8% market share in 2009 to 7.4% market share in 2017, asreported by Market Scope. 1,2 This panel discussion examines why the premium IOL channel hasremained relatively flat during the past 10 yearsand what it will take to increase the marketpenetration.—Stephen G. Slade, MD, FACS;and Steven J. Dell, MDImages courtesy of Market ScopeFigure 1. US market share in the premium IOL channel in 2017.(Abbreviation: PC-IOL, presbyopia-correcting IOL)SNAPSHOT OF THE REFRACTIVE IOLMARKETPLACE: 2009 TO 2017J. Andy Corley: In 2009, after 5 yearsImage courtesy of J. Andy Corleyof existence of refractive presbyopiacorrecting IOL technologies, cataractsurgeons only achieved about 6.8%market penetration,1 when we allbelieved by that point that it would becloser to 20% to 25%. We postulatedFigure 3. US premium IOL channel market share in 2017.Figure 2. US surgeon adoption of premium IOLs in 2017.(Abbreviation: PC-IOL, presbyopia-correcting IOL)that either the lenses or the surgeonswere not good enough, but neitherwas true. What was more true wasthat asking a patient for money,promising an outcome, and thenhaving to deliver on that promise wasvery discomforting to a large segmentof the surgeon population.Fast forward to 2017, and more than600,000 premium cataract procedureswere performed in the United States(Figure 3).2 The overall market hasgrown, but the presbyopia-correctingIOL market has remained flat at only7.4% market share.2Ten years ago, only 25% of surgeons offered premium IOLs to theirpatients;1 now 80% do.2 However,75% of that group implant fewerthan 40 premium IOLs per year.2In other words, the majority ofpractitioners are premium-channelsurgeons, but only a minority fullyembrace the commitment requiredof premium lens offerings. In reality,the number of dedicated premiumchannel surgeons has not increasedin 10 years.So where are we now? We havebetter diagnostics, formulas, and IOLs,and we also have femtosecond lasersand aberrometry technology. We alsohave the toric IOL category, whichhas helped to double the penetrationMAY 2018 CATARACT & REFRACTIVE SURGERY TODAY 51sIS LENS SURGERY THE NEW LASIK?
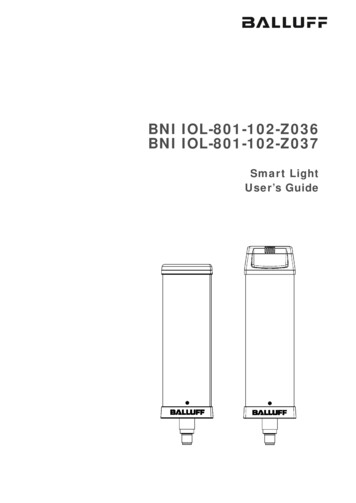
sIS LENS SURGERY THE NEW LASIK?of the premium IOL channel in theoverall cataract market.The questions for today’s panelare these: Will the premium channeldouble again in the next 10 years? Ifso, what are some of the opportunities? Is monovision an opportunity?Have we fully examined the toricopportunity? (Only 8% of patientsreceive toric IOLs, yet 70% of patientshave enough astigmatism to qualifyfor a toric procedure.2) In 2025, wewill hopefully have new presbyopiacorrecting toric IOLs, new generationsof femtosecond lasers, exchangeableand adjustable IOLs, and maybe evenoffice-based surgery. How will thisaffect the premium IOL market?Figure 4. Current premium IOL procedure market share in the United States (blue and green lines on the plot chart)compared with premium IOL market share at Vance Thompson Vision (red arrow).Images courtesy of Vance Thompson, MD, FACSTHE FUTURE OF THE PREMIUM IOLVance Thompson, MD, FACS: Frommy viewpoint, the future of thepremium IOL is bright. The idea ofpremium cataract surgery and what ishappening right now in this space hashad a major impact on my practice.Today, presbyopia-correcting implantsaccount for 40% of the lenses Iimplant, and that doesn’t include toricIOLs (Figure 4). The impact of theselens technologies has been astounding.The list of available IOL optionsnow includes multifocal, extendeddepth of focus, accommodating, andlight adjustable (Figure 5). But wealso know that our refractive precision needs to improve. Posteriorcorneal astigmatism, postoperativecorneal healing, and effective lensposition all can reduce the level ofrefractive accuracy.The most basic and importantelements needed to be a premiumcataract surgeon are an implant andan enhancement plan. It amazes mehow many doctors don’t have a planfor the refractive enhancement. Ithink the hope to optimize patientsatisfaction is one of the main reasons why many surgeons have triedpremium IOLs, and the main reasonwhy many surgeons have abandoned52 CATARACT & REFRACTIVE SURGERY TODAY MAY 2018Figure 5. A partial list of premium IOL implant options. (Abbreviation: EDOF, extended depth of focus)*The AT LISA (Carl Zeiss Meditec), AT LARA (Carl Zeiss Meditec), and IC-8 (AcuFocus) IOLs are not approved for use in the United States.them is patient dissatisfaction. Thisis because the surgeon didn’t knowhow to enhance the postoperativeUCVA. Right now, enhancing premium cataract surgery involves cornealrefractive surgery, and there are manysurgeons who don’t want to learn thenecessary skills in corneal refractivesurgery, and there are many patientswho don’t want to have PRK or LASIKafter premium cataract surgery.If I was a company trying to determine how to move the needle andbreak through this barrier of how toimprove premium cataract surgery, Iwould be looking closely at this issueand educating everyone on whatwe have learned with LASIK patientsatisfaction: UCVA drives patient satisfaction. If you look at a 2016 studyby Steven C. Schallhorn, MD,3 19% ofpatients with 20/25 UCVA after LASIKreported that they were unsatisfied.We need to be targeting 20/20 orbetter in premium cataract surgery.Surgeons who are trying to enter thepremium market rely on preoperative testing technologies to determineif someone is not a good candidatefor a corneal enhancement postoperatively, or maybe they are a reallygood candidate with low cornealmultifocality. They are intimidatedby determining who is a candidatefor a laser fine-tune of their cornea,and they are intimidated by the prospect of performing corneal refractivesurgery after premium IOL surgery.And, besides that, they are busy.When you are educating the patienton which IOL to choose, refractivesurgeons approach this differently
IS CONSUMER ADVERTISING THE ANSWER?STEVEN J. DELL, MDn M edical Director, Dell Laser Consultants,Austin, Texasn C hief Medical Editor, CRSTn s teven@dellmd.comn F inancial disclosure: Consultant (Bausch Lomb, Johnson & Johnson Vision, OpticalExpress, Presbyopia Therapies, TraceyTechnologies)STEPHEN G. SLADE, MD, FACSn P rivate practice, Slade and Baker Vision,Houston, Texasn E ditor Emeritus, CRSTn s gs@visiontexas.comn F inancial disclosure: Consultant (Alcon,Carl Zeiss Meditec)J. ANDY CORLEYn C ofounder, Eyeonics (now Bausch Lomb)n P artner, Flying L Partnersn F inancial disclosure: Chairman of the Board(Equinox, eyeBrain Medical, RxSight)BRIAN O’NEALn H ead of US Marketing, Alcon Surgicaln b rian.oneal@alcon.comn F inancial disclosure: Employee (Alcon)SANDY T. FELDMAN, MD, MSn C learview Eye and Laser Medical Center,San Diego, Californian s feldman@clearvieweyes.comn F inancial disclosure: Consultant (Carl ZeissMeditec, Johnson & Johnson Vision)than cataract surgeons. We needto teach cataract surgeons who aregoing into refractive cataract surgeryhow to educate patients on advancedimplant technologies.If we are going to break this barrier and see premium implants growin our world, we need to educatesurgeons who desire to add or growthis area of their practice on what ittakes to build a modern day refractiveSandy T. Feldman, MD, MS: Why don’tcompanies educate consumers throughadvertising? It would be easier for patients tomake decisions about having premium lensesif they had already heard about them or knew afriend who had them.Since this information is new to manypatients, a lot of education is done byphysicians and their staff. If the consumeralready knows that IOLs that enable betterdistance and near UCVA are available, thatmight drive the market, as the physician andtheir staff are recommending something thatis already familiar. Today’s lenses are differentthan prior generations of implants.Brian O’Neal: Alcon is doing direct-to-consumer marketing. About 1 year ago, we launchedthe website MyCataracts.com. It is completelyunbranded and has no specific lens types mentioned. It is a significant digital effort; it is 100%digital with mostly paid search. You are right:Online is exactly where these patients or caregivers are today.J. Andy Corley: When you advertise tothe general public and only a segment of thechannel is available to deliver the service youare promoting, it’s not a good investment. Wetried it with the Crystalens (Bausch Lomb)with mixed results.O’Neal: It is about 1,500 to 1,600 (data on filewith Alcon).Feldman: But advertising has changed,and targeting has changed with digital media.There are ways to drive things digitally.Additionally, the lenses have changed, andthey deliver better results than prior generations of lenses.Stephen G. Slade, MD, FACS: Is any lens company currently doing direct-to-consumer marketing, digitally or through traditional marketing, toeducate patients about these technologies?cataract surgery practice. (To find outDr. Thompson’s top five tips for building a modern practice, see First Stepsto Beginning With Premium IOLSurgery.) Ways to adjust an implant’spower postoperatively, inside the eye,will be available in the future. We willsoon have the ability to take an optic(that is inside the patient’s eye!) andactually change the polymer in a waythat is going to allow a patient toSteven J. Dell, MD: That is to be applauded,and it is an excellent thing that you are doing.The challenge associated with it is that we havegot all of these cataract surgeons in the UnitedStates, but how many are regularly offeringpresbyopia-correcting IOLs?Dell: That is the number who are offering it,but the number who are actually doing morethan a couple of presbyopia-correcting IOLs amonth is shockingly small; it is probably in therange of 300 to 400. The problem is that you arebroadcasting premium IOLs to these patientsthrough targeted search information, and thatpatient may wind up in a surgeon’s office who isnot going to close the loop and seal the deal.O’Neal: You are right. As Mr. Corley stated,that has been the issue for a long time. You caneducate the patient and drive them into theoffice, but are they going to the right place? Thatis a difficult thing to control.choose exactly what sort of vision heor she wants. This is exciting becausefor the first time we will be able tosimulate it for them postoperatively.Currently, patients with cataractevaluations have blurry vision, andwe can’t show them different types ofvision, such as monovision, becausethey are blurry. When we can putin a light adjustable lens, we can tellpatients not to worry about whereMAY 2018 CATARACT & REFRACTIVE SURGERY TODAY 53sIS LENS SURGERY THE NEW LASIK?
sIS LENS SURGERY THE NEW LASIK?exactly they want their vision focusedafter surgery; rather, we can showthem the various options when theyhave clear vision at about 3 weekspostoperatively. I think this is going tostimulate this premium lens markettremendously. I think patients wouldrather have their implant adjustedthan their cornea adjusted. The easeof adjusting the refractive state of theeye by adjusting implant power insidethe eye is going to be huge.DEFINING ADOPTIONStephen G. Slade, MD, FACS: If wedefine premium IOLs as presbyopiacorrecting and astigmatism-correctingtoric IOLs, 60% of the IOLs we implantat our practice are presbyopiacorrecting and 20% are toric. Intotal, therefore, we are implanting apremium IOL in 80% of our patients.How does this measure up to others?Steven J. Dell, MD: Ten years ago, ourpractice was implanting a premiumIOL in 60% to 70% of patients, and it isstill 60% to 70% today.Slade: Why do physicians accept toricIOLs, as there has been growth in thatmarket, but the presbyopia-correctinglens market is about the same? Let’ssolve that problem.John F. Doane, MD: I think there are tworeasons that market hasn’t grown. Thefirst, for our practice, is that a certainpercentage of physicians simply don’twant to ask patients for money. Eitherit is a moral or ethical reason, but theydon’t feel comfortable talking about thecost of the premium IOL. The secondis that we have had surgeons who havegone down the multifocal pathway buthave had issues with patient complaints.What I have found over the years is thatif the surgeon has a bad experience withone lens, he or she tends to discontinueusing all premium lenses. I think thebiggest barriers to better adoptionof premium IOLs include a lack ofavailability of technology to enhancevision postoperatively, not wantingto talk about the cost with patients,and previous negative experienceswith a lens.Donaldson: It is a challenge, and itSlade: I agree, and I would definethe presbyopia component of thechannel? The lenses are better today,and doctors are better trained thanthey were at the outset of premiumIOL surgery. We started the premiumchannel with immersion A-scans, andnow we have so many new devices. Itis curious to me why the presbyopiacorrecting IOL category has remainedflat in light of this. John, what are yourthoughts?negative experience as explant rate.Kendall E. Donaldson, MD, MS: I thinkthere are two types of cataractsurgeons: traditional cataractsurgeons and refractive cataractsurgeons. In order to be a refractivecataract surgeon, you must have theinfrastructure in your practice tocreate a successful premium practice.Practices need to be designedtoward the propagation of the premium channel, and you need to have theright staff in place. Premium cataractsurgeons have technology to help usprovide the best refractive outcomespossible, but the average cataract surgeon may not be in that situation.Slade: Are you successful withpremium IOLs in your universitysetting at Bascom Palmer?is time-consuming. We are alwaysfighting to put the right staff in place.But if I had a concierge practice, whichis hard to do in an academic center,it could be easier. I would have theright staff to properly educate patientsand guide them through the pre- andpostoperative experiences.This time-consuming process couldthen be removed from the physicianand allocated to someone else. Youneed to have the infrastructure, thetime, and the ability to do all of thesethings successfully in order to cater topremium IOL patients.Corley: Can we be more granular onDoane: You are preaching to thechoir with this group of surgeons.Ophthalmologists send patients downthe road to the optical shop; theyaren’t doing the transaction, and theyaren’t asking for money. I have mydiscussion with the patient, and staffeducators talk money.Slade: That is a good point. Eventhough we have a high conversionsss54 CATARACT & REFRACTIVE SURGERY TODAY MAY 2018ssN o. 1: Network with other refractive cataract surgeons. (Example: Ourcenter hosts surgeons from around the world who are looking to addpremium cataract surgery to their practice.)N o. 2: Understand the various types of IOLs that are available, such asextended depth of focus, low-add multifocals, accommodating, toric, andmonofocals.sFIRST STEPS TO BEGINNING WITH PREMIUM IOL SURGERY BY VANCE THOMPSON, MD, FACS No. 3: Establish a laser enhancement plan if the patient experiences blurpostoperatively.N o. 4: Form a teaching plan to educate your team, your referring doctors,and your community.N o. 5: Obtain the right patient education materials (print and online) foryour team to hand out to your patients.
rate in our practice, I don’t talk moneyto the patients. Everybody tells meI should.Dell: Who has a partner who doeshigh-volume cataract surgery butdoesn’t want any part in premiumIOLs? When you are trying to coexistwithin your refractive cataract surgerypractice, as Kendall mentioned, it is aninfrastructure challenge because yourwaiting room is a zoo. They are runninga large volume of people through theoffice, and when you try to establish aconcierge experience where the patientis offered refreshments and waits5 minutes to see the doctor, that is adifficult thing to do in the environmentI described.Guy M. Kezirian, MD: Andy and I workedon this years ago, and I think wehave diagnosed the problem prettywell. If a lens surgeon is not arefractive lens surgeon in 2018, thereis only one reason: It is because heor she doesn’t want to be. Whenthis IOL category rolled out, wetargeted cataract surgeons, thinkingthey would be enthusiastic refractivesurgeons, and the reality is that theyare not.The culture change it is going totake to grow this market sector isprobably not possible with existingsurgeons. We need to focus on theyounger surgeons who accept this asbeing normal and who will embracethe concept of being a refractive cataract surgeon.Kenneth J. Rosenthal, MD, FACS: I thinkthat now, in New York, there aremany surgeons who do not offeradvanced-technology lenses, and thereason why is simple: They haven’tlearned techniques necessary toperform this type of surgery, andthey don’t want to refer patients outfor it. The surgeon will say to thepatient: “You need cataract surgery.Please see my surgical coordinator,”and that is the end of the discussion.The discussion should be: “Advancedtechniques and lenses are available,and you may benefit from one. I don’tperform this surgery, but I can referyou to someone who can.”There is an economic disincentive to refer patients out if you don’tperform a procedure, and I think thisis wrong-minded. Informed consentconsists of providing the patient withall risks, benefits, and options available. If there is something out therethat could benefit a patient, and youdon’t tell the patient about it, I thinkthere is a disconnect with good clinical practice.What is the solution? Maybe partof the solution is for those doctors toknow they must disclose the otherchoices. I think it is a huge problem,and I often see patients postoperatively who are referred to me becausethey are unhappy with their UCVAand have now heard they could havehad a different type of surgery to correct their vision.William F. Wiley, MD: One thing I seemissing is buy-in from optometry. Ithink we need better education inthat community. I think optometristsare often the gatekeepers to thesetechnologies. If the optometristdoesn’t recommend a premiumtechnology, it is harder for a surgeonto recommend it.Slade: It is a wonderful strategy tohave an optometrist who you canpartner with in your office. That ODcan talk to the patient and introducethe idea of a premium IOL before thepatient sees you.In terms of IOL technology, it isdifficult to make a recommendationto someone for a lens that can’t bechanged in the future. Many of mypatients aged 50 or older will ask me,“If something better comes along, canI have that?” And in truth, I have totell them no.One small piece of the puzzle isthat refractive cataract surgeonsare the people who are doing manyof these procedures. By definition, those surgeons have manypostrefractive surgery (LASIK, RK,and PRK) patients in their practice.The plea to the industry is to giveus lenses that are compatible withpostrefractive patients. In my experience, the Crystalens (Bausch Lomb)is as compatible as a monofocal, andit is one of the reasons why we havehad so much success with it.Dell: I think the financial componentof it is a big part of the story. Let’simagine that cataract surgery wasnot a covered service in the UnitedStates. Someone came to you for amonofocal, and he or she had to pay 5,000. Think about the FDA gridon every monofocal IOL that youhave ever seen and the percentageof patients who would not have thesame IOL again; there is always 2% to3% of patients who say, “I receivedthis lens for free because I was in aclinical trial, but I wouldn’t choosethis lens again.” If monofocal IOLswere 5,000, I think the number ofpeople who are dissatisfied with themwould be significant. There wouldbe 3% to 4% of patients who wouldsay, “I don’t like the way I see withthis lens.”Slade: Vance, you have hadexperience with the Light AdjustableLens (RxLAL, RxSight), but that wasin a clinical trial setting. Patientsdon’t experience the benefit rightaway, so how do you sell thattechnology to patients?Thompson: One of the benefits ofmonovision is that, if someone isunhappy in certain situations, suchas nighttime driving, he or she canput on a pair of glasses and clear itup beautifully.But we also know that, in thedominant eye, or at least the distance eye, achieving as close to planoas possible is important for optimalMAY 2018 CATARACT & REFRACTIVE SURGERY TODAY 55sIS LENS SURGERY THE NEW LASIK?
sIS LENS SURGERY THE NEW LASIK?Slade: But what is going to be yourdiscussion? Talk to me like a patient.Thompson: I think it motivates patientswhen I tell them, “We do thesepreoperative measurements to figureout the best implant power for you,but this implant is not specificallymade for your eye. We won’t knowthe exact implant you need untilwe see you postoperatively due toa variety of factors, such as the finalresting position of your implantor any astigmatism that may haveincreased or decreased with healing.What is beautiful about this advancedpremium implant is that we still doall of those same measurements thatwe do with every implant, but thenwe put it into your eye, and whenit settles into position at 3 weekspostoperatively, we can get bettermeasurements. We can then use alaser to truly, for the first time in thehistory of cataract surgery, adjust itspower to your eye and your desires.It will be an implant made specificallyfor you and customized inside youreye. It is like a dream come true.”Donaldson: I think we have toremember that the surgeonsparticipating in this discussion aresometimes more willing to adoptnew technologies than others. I knowVance has a wonderful practice, andmost of us here have great practicesthat are designed around refractivetechnology. But I have a colleaguewho won’t put any premium lensesin patients, and she says, “You haveall of these premium lens options,but clearly you haven’t gotten itright yet.”56 CATARACT & REFRACTIVE SURGERY TODAY MAY 2018Bennett Walton, MD, MBA: I think weshould consider not calling it apremium lens when discussingoptions with patients. First of all,what we have isn’t really goodenough to label it with such a valueadd word. We are still not fullyrestoring vision to a young, healthystate. I don’t believe what we haveis good enough to call it premium,but it is certainly good enoughto change a lifestyle with, and itmakes a difference to patients whoselect advanced lenses. I think theverbiage is crucial here; premiumcan be a surrogate for fancy or bellsand whistles, leading to a negativeconnotation in some markets.Thompson: One thing that is sowonderful about a traditionalcataract surgery with a monofocalimplant is that after surgery thepatient leaves, they receive glasses1 month postoperatively, and youoftentimes never hear from themagain because they are satisfied. Oneof the things we do with every singleadvanced implant we perform isto contact the patient at 1 monthpostoperative to gauge how they areresponding to the surgery. I receivea report every week that includes alist of patients who are 1 month out,and we track their satisfaction. If Isee anyone who is not satisfied, I callthem personally.At 3 months, we examine eachpatient in person because we wantto make sure he or she is satisfied,and if he or she is not, we will perform a laser fine-tune. It is importantto have patients understand whathealing blur is and to realize thatmost cataract surgery proceduresneed a fine-tune postoperatively;with traditional cataract surgery,the fine-tune is glasses at 1 monthand with advanced cataract surgerythe fine-tune is a laser touchup oftheir cornea at 3 months. With lightadjustability, the fine-tune will be alaser adjustment of their implant atsmonovision success. I like to callthis precision monovision. This ideaof not only monovision, but precision monovision, is going to be moreinteresting to all cataract surgeons,even to those of us who do a highvolume of multifocal and extendeddepth of focus procedures.WATCH IT NOWBIT.LY/AECOS05183 weeks postoperative. I tell them tocount on requiring a fine-tune, andif they don’t need it because theyare seeing crystal clear, then we lovethat too.Slade: Great idea. Andy, you had thefirst comment in this discussion, sowhy don’t you also have the last.Corley: I do believe future IOLtechnology will expand the premiumchannel, and I do believe the premiumchannel will double again in the next10 years. The motivations and theincentives for all of us are high, andit provides ancillary benefits like theincentive to fund other technologies.We spent time today on how wetalk to patients, and I think that issomething industry can play a bigger role in, trying to be helpful to ourphysician community (see Is ConsumerAdvertising the Answer?).We hear people say: “People loveto buy and hate to be sold.” If we cancontinue to improve the outcomespatients achieve after cataract surgerywith a premium lens and find theproper ways to educate patients withthe right information, I believe patientswill continue to buy into premiumofferings.Slade: Thank you, everyone. That wasone of the best discussions we havehad in a while. n1. 2009 Global IOL Report. Market Scope. Published 2009. Data on file.2. 2017 Annual US Cataract Surgeon Survey Report. Market Scope. . Published May 2017. Accessed April 4, 2018.3. Schallhorn S. Lessons learned in refractive surgery. Paper presented at: theAECOS 2016 Winter Symposium; Aspen, Colorado; February 28-March 2, 2016.
Medical Director, Bascom Palmer Eye Institute, Plantation, Florida n Member, CRST Editorial Advisory Board n KDonaldson@med.miami.edu n Financial disclosure: Consultant (Alcon, Bausch . (that is inside the patient's eye!) and actually change the polymer in a way that is going to allow a patient to choose exactly what sort of vision he