Transcription
Rehabilitationafter braininjuryDr Simon Fleminger andDr Esme Worthingtonthe brain injury associationThis booklet has been written as a guide to brain injuryrehabilitation, its settings, aims and the professionals involved.It is intended primarily for the families and carers of brain injurysurvivors.
Rehabilitation after brain injuryThis e-booklet is an adaptation, created in September 2016, of the Headway printbooklet Rehabilitation after brain injury and may contain minor updates to the originalversion.published byHeadway – the brain injury associationBradbury House, 190 Bagnall RoadOld Basford, Nottingham NG6 8SFAuthors: Dr Simon Fleminger, Consultant Neuropsychiatrist,Maudsley Hospital, London, and Dr Esme Worthington.Editor: Tamsin Ahmad, Publications and Research Manager,Headway – the brain injury association. Previously edited byJoe Leadley and Richard Morris.All rights reserved. No part of this publication may be reproduced,stored in a retrieval system, or transmitted by any means, electronic,mechanical, photocopying, recording or otherwise, without priorpermission in writing from the copyright owner. Headway – the brain injury association, 2007Second edition, 2009. Reprinted 2011, 2014 & 2016.ISBN: 978-1-873889-60-2This booklet received a CommendedAward at the British Medical AssociationPatient Information Awards 2010
Headway – the brain injury association ContentsIntroduction . 2Accessing rehabilitation . 3Rehabilitation settings . 4What if no rehabilitation has been provided? . 5Timescales for recovery and rehabilitation . 6Headway Approved Provider scheme . 7The rehabilitation team . 8Psychological recovery . 12Returning to work . 13Support for families . 15Further reading . 16Clinical guidelines . 18Useful organisations . 19How to donate . 22Internal areas of the brain and their functions . 23The cerebral cortex . 24About Headway . 251
Rehabilitation after brain injuryIntroductionOnce a person with a brain injury is medically stable andany physical injuries have been treated, they may beready to be discharged from the hospital, or ‘acute care’,setting. However, many of these individuals are likely toexperience complex, longer-term physical, cognitive andbehavioural problems, which require a period of rehabilitation.Unlike most other cells in the body, brain cells do notregenerate when they are destroyed. However, this does notmean that no recovery can occur. The brain is somewhatflexible and is able to reorganise itself, to an extent, in order toregain lost function. This is known as brain plasticity. Duringrecovery, other areas of the brain take over the activities of thedamaged areas and new nerve pathways can be establishedusing undamaged ‘spare’ brain cells. Engaging in activity helpsthese alternative pathways to develop.Rehabilitation aims to help the brain learn alternative ways ofworking in order to minimise the long-term impact of the braininjury. Rehabilitation also helps the survivor and the family tocope successfully with any remaining disabilities. 2
Headway – the brain injury association Accessing rehabilitationThere are many rehabilitation services across the UK, runby the NHS or private firms. Choosing which rehabilitationunit to refer someone with a brain injury to should involve theclinical team, the patient and their family. Once a referral hasbeen made, the rehabilitation unit will usually carry out anassessment to make sure their service is suitable.Availability and funding for places varies. However, most units,including private ones, accept NHS referrals and will befunded by the NHS. Other possible sources of fundinginclude local authority social services, medical insurance,compensation claims and self-funding.It is important to ensure that whoever is likely to have to fundthe rehabilitation is aware that a referral has been made. Therehabilitation service will not be able to accept an admissionuntil funding has been authorised. Many services acceptreferrals from outside their own area, but there are oftenlimited places available and long waiting lists. Specific detailsabout the referral process, funding options and availability ofplaces will be available from the unit.Taking up a rehabilitation placement is an importantcommitment, and it is wise to explore all the options, visitdifferent rehabilitation settings, and ask as many questionsas possible before a placement is confirmed.3
Rehabilitation after brain injuryRehabilitation settingsRehabilitation occurs in the following settings. Mostrehabilitation units provide one or more of these services:Post–acute rehabilitation: Intensive specialist rehabilitationfor people who are not yet ready to return home afterdischarge from hospital. Neurological rehabilitation centresprovide an ideal setting for further treatment, with a structuredrehabilitation programme in place throughout the day.Rehabilitation back into the community: Following aninpatient rehabilitation stay, some patients may be transferredto a residential transitional living unit. Here the patient willdevelop their independent living skills so that when they leavethey are able to live in a place of their own. Other patients willgo straight back to their homes, with community rehabilitationteams or outreach teams helping them to make furtherprogress; this may involve therapists coming to visit the personin their home or hostel.Outpatient rehabilitation: Some patients may be well enoughto return home and receive further treatment as an outpatient,either at a local hospital or at a separate rehabilitation centre.Slow-stream rehabilitation: Some patients who no longerrequire intensive post-acute rehabilitation may still not beready to return home. These people may require long-termresidential care.Severely injured patients may still have the potential to makecontinued progress, even several years after the injury,although this may be slow. Therefore, it is important that their 4
Headway – the brain injury association rehabilitation is not cut short. Many brain injury residential careunits provide what is known as ‘slow-stream rehabilitation’ andif somebody with a brain injury can potentially benefit from thisapproach it is important they are given the opportunity.All residential care services should be registered with the CareQuality Commission (CQC). You can check whether aparticular unit is registered and view reports on the service bycontacting the CQC on 03000 616161, or by visiting theirwebsite.What if no rehabilitation has been provided?If your relative has been discharged home without any access torehabilitation, and you have reason to believe that they wouldbenefit from it, there are still options available.You are perfectly within your rights to actively seek rehabilitationservices, even if you have been told that there are none availableor needed. The first thing to do is discuss the matter with yourrelative’s GP and/or consultant. They may be able to provide areferral.You can also contact rehabilitation services directly. TheHeadway helpline can provide information on specialist braininjury rehabilitation centres across the UK. For furtherinformation, call the helpline on 0808 800 2244.You can find a directory of rehabilitation services across theUK on the Brain Nav – The National Brain Injury ServiceDirectory website. It is advisable to contact several units andvisit them to assess their suitability before making a decision.5
Rehabilitation after brain injuryTimescales for recoveryand rehabilitationIn the first month or two after a severe brain injury it is onlypossible to guess at the length of time that recovery willtake and the likely outcome. All that is certain is that recoveryis a slow process and will take months or years rather thanweeks.Six months after the injury the picture will be clearer, but it iswise to wait until about a year after the accident beforemaking any important decisions regarding the future. After ayear or so one can be reasonably certain about the eventualdegree of physical recovery. However, psychological recoverycan take considerably longer and it is usually the cognitive(thinking), emotional and behavioural problems that causelonger-term difficulties, particularly for family members.People do sometimes talk about there being a limited‘window’ for recovery after brain injury, for example, thatrecovery ceases to take place beyond two years. However,this is now known not to be the case and people may actuallycontinue to improve for a number of years after brain injury.Indeed, many people say that they never stop regaining theskills that they lost following the injury.Nevertheless, the greatest visible progress does occur in thefirst six months or so post-injury and after this improvement isoften less obvious. 6
Headway – the brain injury association Factors which may affect the rate of the person’srecovery include:llllllType, severity and location of the person’s brain injuryAge (younger adults tend to do better)Pre-injury healthPre-injury personality, intelligence and lifestyleSocial support from family and friendsOther issues, such as alcohol or drug misuse.Depending on the individual’s specific difficulties and theirpotential for recovery as assessed by rehabilitation staff, aprogramme of rehabilitation may last for a few weeks or maycontinue for months or years.Headway Approved Provider schemeHeadway has developed the Approved Provider scheme, anaccreditation scheme appropriate for NHS and independent caresettings, including hospitals and neuro-rehabilitation units,residential care homes, nursing homes and respite facilitiesspecialising in ABI.The units on the Approved Provider list have been assessedagainst standards devised by Headway to ensure they provideappropriate specialist care for brain injury survivors with complexphysical and cognitive impairment. Further information and a listof Approved Providers can be accessed on the Headwaywebsite.7
Rehabilitation after brain injuryThe rehabilitation teamIn a specialist rehabilitation setting, a ‘multidisciplinary’ teamof professionals will work closely with the person with abrain injury.Initially, each therapist will carry out detailed assessments toexplore the extent of the difficulties caused by the brain injury,including physical, cognitive, emotional, behavioural and socialdifficulties.Following the assessment process, the team will discuss withthe client and the family what their priorities and goals for theperiod ahead might be and what they hope to achieve. Basedon this, the rehabilitation goals – both short and long-term –will be agreed and the rehabilitation programme will beplanned. In devising the rehabilitation programme, the teamwill want to set goals that take into account each patient’sindividual views and needs, their cultural background, andpre-injury lifestyle and interests.The different therapists who may be involved in therehabilitation process, and their areas of expertise, areoutlined below:Clinical neuropsychologistA clinical neuropsychologist is a psychologist who specialises inthe assessment and treatment of behavioural, emotional andcognitive (thinking) problems following brain injury. Aneuropsychologist can advise on how to build upon theperson’s existing skills and abilities and how to reduce some oftheir difficulties. 8
Headway – the brain injury association Occupational therapist (OT)OTs help people to develop independence in carrying out dailytasks such as dressing, washing, cooking and leisure activities.An OT will also help the person to develop the skills thatunderlie these activities, such as budgeting and planning, andhelp to find ways around any remaining problems. At a laterstage, the OT may help and advise on difficulties that may beencountered in the home environment and advise on anyadaptations that may need to be made. They will also beinvolved in planning for returning to work. There are OTs workingwithin both the NHS and social services.Speech and language therapistA speech and language therapist (sometimes referred to as aSALT or SLT) helps people to improve their communicationskills. This may include understanding and expressing bothwritten and spoken language and improving speech clarity. Thespeech and language therapist will work with family members tohelp the person to communicate as best they can in their dailylife and will identify any communication aids that may be helpful.They may also be required to assess swallowing difficulties andprovide guidance on how this should be managed safely.Further information on this subject can be found in theHeadway booklet Coping with communication problems afterbrain injury.PhysiotherapistA physiotherapist helps people to regain the use of their musclesand joints after injury and helps with balance and9
Rehabilitation after brain injurymovement problems. A ‘physio’ will, for example, suggestexercises to help the person improve their physical ability andenable them to become as mobile and independent as possible.NurseNurses help the therapists to implement many of therehabilitation strategies. In many in-patient rehabilitation units thecare provided by the nursing team is the foundation for therehabilitation programme provided by the multidisciplinary team.On in-patient units and in the community there may be specialistnurses who take on specific roles, such as the management ofepilepsy or behavioural programmes.Social workerSocial workers provide practical advice on issues such asbenefits, housing, transport and assistance at home. They arealso trained to offer emotional support to individuals and theirfamilies.Case managerA case manager is responsible for overseeing and managing theoverall care of the person with a brain injury. They will preparean individually-tailored care plan or treatment programme foreach client, which is designed to meet the person’s specifichealth, social and emotional needs. Case managers can comefrom a variety of professional backgrounds, such as social work,occupational therapy, or nursing. Brain injury case managers areusually only available through private referrals and interimcompensation payments. 10
Headway – the brain injury association Family membersFamily members have a very important role to play in helping thesurvivor make as full a recovery as possible. A good workingrelationship between the family and the rehabilitation team isessential in making sure that rehabilitation programmes arefollowed correctly. Research suggests that the patients whomake the best recovery are those whose family is activelyinvolved and can maintain the skills learned in rehabilitation oncethe patient has gone home.Sometimes relatives will need to learn new skills so that theycan help to provide the best support. However, it is importantthat the family member does not become a ‘therapist’ and thatthey are encouraged to focus primarily on their role assomebody who provides love and affection. Family members areusually invited to participate in formal meetings with staffmembers to keep them informed of their relative’s progress.Sometimes the family will need to act as an advocate for thesurvivor when the survivor lacks the capacity to make decisionsfor themselves.There are many rehabilitation professionals working in privatepractice. If little or no rehabilitation has been provided by theNHS or social services then one option can be to contactprofessionals independently. It may still be possible to obtainan NHS or social sevices referral, or it may be necessary topay privately. You can find details of organisations whoprovide directories of chartered rehabilitation professionals inprivate practice in the ‘Useful organisations’ section at theback of the booklet.11
Rehabilitation after brain injuryPsychological recoveryAwide variety of cognitive, behavioural and emotionalproblems can occur after brain injury and may impactsignificantly on work and family relationships. Even after minorinjury some people have persistent problems for months oreven years.Problems may not be immediately obvious after the injury, butmay become apparent some weeks or months later as theperson engages in more activities. Nevertheless, particularlyfor those with severe injuries, slow but steady improvementtends to occur in psychological symptoms over a period ofmonths or years.Many cognitive, behavioural and emotional problems can behelped by treatment from a clinical neuropsychologist. Forexample, if problematic behaviours develop after brain injury(such as verbal or physical aggression, or inappropriate sexualbehaviour) behavioural modification programmes may beused to raise the patient’s awareness of their behaviours andencourage more appropriate responses. Cognitiverehabilitation may also be used to help improve attention,memory, and language abilities. Finally, various psychotherapyapproaches may also be used, such as cognitive behaviouraltherapy (CBT), which help patients to learn to cope emotionallywith their disabilities and to re-establish meaning in their life.There are a number of publications available fromHeadway that give detailed information on psychologicaldifficulties after brain injury. See ‘Further reading’ for moreinformation. 12
Headway – the brain injury association Returning to workOnce the person is able to look after their personal needs,to travel around from place to place and to managesocial contacts reasonably well, they may be able to considerreturning to work. This will depend largely on the degree ofrecovery that has been made, what the person’s previous jobwas and what employment opportunities may now beavailable. For those with less severe injuries, return to workwithin a few weeks or months is often achievable.However, it is important not to rush back to work too quickly.If this happens, some problems that had seemed to beresolved may reappear. The person may, for example,suddenly find that their concentration or energy levels, whichseemed fine at home when convalescing, are not as good asthey thought. It is often wise to look at a phased return towork, so that the way in which the person is coping with thetransition can be gently tested out. Some people will be ableto return to their old job, while others may need to consider aless demanding role. A period of retraining may be requiredand adaptations to the workplace may be needed.Ideally, a specialist brain injury vocational rehabilitation servicewill be able to provide assessment and rehabilitationprogrammes that will enhance the potential to return to work.Vocational rehabilitation involves professionals such asneuropsychologists and occupational therapists, who can helppeople to understand the type of work they can now do andsupport them to achieve their goals.13
Rehabilitation after brain injuryOnly a small number of specialist vocational rehabilitationservices are available, although many units and communitybrain injury teams provide similar services. The Headwaywebsite provides details of the services available in the UKand the information in the ‘Accessing rehabilitation’ and‘What if no rehabilitation has been provided?’ sections of thisbooklet also applies to these services.If the injury has been very severe, the person may not be ableto return to paid employment. In this case, it is important thata plan is worked out to give the person a regular, satisfyingway of spending their time. Access to leisure activities, socialinteractions and other meaningful activities such asvolunteering will be important to provide structure in their life,as well as a sense of purpose and achievement. LocalHeadway groups and branches, as well as social services daycentres and other voluntary and statutory sectororganisations, may be able to provide facilities toaccommodate these needs.For further information on returning to work, including a rangeof freely downloadable factsheets, visit the website. 14
Headway – the brain injury association Support for familiesThe various difficulties that can occur after brain injury, inparticular behavioural and emotional problems, can have abig impact on family members. There may well be additionalsocial or financial difficulties for the family, and relatives mayneed as much help and support as possible.Studies have shown that family support and counselling areneeded, not just in the early days but for a long timeafterwards. The children of a brain injured parent can also beeasily overlooked. It is very important that the relativesacknowledge the difficulties they are experiencing and ask forhelp when they need it.The GP is normally the first point of contact, who, in turn, mayadvise seeking help from a clinical psychologist, social worker,counsellor, or others as appropriate and available. LocalHeadway groups and the Headway freephone helpline canalso be useful in supporting both the person with the injuryand their relatives and friends. (See contact details forHeadway on the inside back cover).15
Rehabilitation after brain injuryFurther readingThe following books are available from Headway andprovide a good introduction to brain injury and its effects:n Clare, L. & Wilson, B.A. (1997) Coping with MemoryProblems: A practical guide for people with memoryimpairments, their relatives, friends and carers.London: Pearson Assessment.n Daisley, A., Tams, R. and Kischka, U. (2008)Head Injury: The Facts. Oxford: Oxford University Press.n Hedley, N (2011) Living with an Acquired Brain Injury:The Practical Life Skills Workbook.Milton Keynes: Speechmark Publishing Ltd.n Johnson, J. (2013) My Dad Makes the Best Boats.Milton Keynes: Speechmark Publishing Ltd.n Johnson, J. (2013) My Mum Makes the Best Cakes.Milton Keynes: Speechmark Publishing Ltd.n Johnson, J. (2011) “My Parent has a Brain Injury.”.a Guide for Young People. Self-published.n Powell, T (2013) The Brain Injury Workbook:Exercises for Cognitive Rehabilitation.Milton Keynes: Speechmark Publishing Ltd.n Powell, T. (2004) Head Injury: A Practical Guide.Milton Keynes: Speechmark Publishing Ltd. 16
Headway – the brain injury association Headway also produces an extensive range of bookletsand freely downloadable e-booklets and factsheets.For more information, please visit our website atwww.headway.org.uk/information-library, or telephone0115 924 0800. Brain injury survivors and carers canreceive free print copies of appropriate booklets from theHeadway helpline on 0808 800 2244.Headway’s Amazon shop sells a wide range of bookson the subject of brain injury and brain function. Visitastore.amazon.co.uk/headwathebrai-2117
Rehabilitation after brain injuryClinical guidelinesThe following guidelines have been produced in order toimprove rehabilitation services for adults with acquiredbrain injury and their families and carers.n British Society of Rehabilitation Medicine (2009). BSRMStandards for Rehabilitation Services, Mapped onto theNational Service Framework for Long-Term Conditions.London: BSRM, 2009.n Royal College of Physicians and British Society ofRehabilitation Medicine. Rehabilitation following acquiredbrain injury: national clinical guidelines (Turner-Stokes, L., ed).London: RCP, BSRM, 2003.n Royal College of Physicians, British Society ofRehabilitation Medicine and Department for Work andPensions. Vocational assessment and rehabilitation afteracquired brain injury: inter-agency guidelines (Tyerman, A.& Meehan, M., eds). London: RCP, BSRM, 2004.The first report listed is available to download free of chargefrom the British Society of Rehabilitation Medicine’s websiteat www.bsrm.co.uk. Go to the ‘Publications’ section.The other two reports are available to download free ofcharge from the Royal College of Physicians (RCP) website atwww.rcplondon.ac.uk. Go to the ‘Shop’ section, click on‘Explore our bookshop’ and search the A-Z list. 18
Headway – the brain injury association Useful organisationsAfasicHelpline: 0300 666 9410Web: www.afasic.org.ukASSIST Trauma CareHelpline: 01788 560 800Web: www.assisttraumacare.org.ukBrain and Spinal Injury Charity(BASIC)Helpline: 0870 750 0000Email: enquiries@basiccharity.org.ukWeb: www.basiccharity.org.ukBrain and Spine FoundationHelpline: 0808 808 1000Email: helpline@brainandspine.org.ukWeb: www.brainandspine.org.ukBrain Tumour Charity, TheHelpline: 0808 800 0004Email: support@thebraintumourcharity.orgWeb: www.thebraintumourcharity.orgCarers UKHelpline: 0808 808 7777Email: advice@carersuk.orgWeb: www.carersuk.orgCerebraHelpline: 0800 328 1159Email: info@cerebra.org.ukWeb: www.cerebra.org.ukChild Brain Injury TrustHelpline: 0303 303 2248Email: helpline@cbituk.orgWeb: www.childbraininjurytrust.org.ukConnect – the communicationdisability networkTel: 020 7367 0840Email: info@ukconnect.orgWeb: www.ukconnect.orgDifferent StrokesHelpline: 0845 130 7172Email: info@differentstrokes.co.ukWeb: www.differentstrokes.co.ukEncephalitis SocietyHelpline: 01653 699 599Web: www.encephalitis.infoEpilepsy ActionHelpline: 0808 800 5050Email: helpline@epilepsy.org.ukWeb: www.epilepsy.org.uk19
Rehabilitation after brain injuryEpilepsy SocietyHelpline: 01494 601 400Web: www.epilepsysociety.org.ukMeningitis NowHelpline: 0808 80 10 388Email: info@meningitisnow.orgWeb: www.meningitisnow.orgMeningitis Research FoundationHelpline (24hr): 0808 800 3344Email: info@meningitis.orgWeb: www.meningitis.orgPituitary Foundation, TheHelpline: 0845 450 0375Email: helpline@pituitary.org.ukWeb: www.pituitary.org.ukStroke AssociationHelpline: 0303 3033 100Email: info@stroke.org.ukWeb: www.stroke.org.ukRehabilitation and counsellingservicesThe following organisations provideinformation on rehabilitation, carehomes or counselling services in theUK. Some have online directories ofprofessionals in NHS or privatepractice. Headway does notrecommend any specific services andit is suggested that you contact morethan one before making a decision.Association for the Rehabilitationof Communication and Oral Skills(ARCOS)Helpline: 01684 576 795Email: admin@arcos.org.ukWeb: www.arcos.org.ukAssociation of Speech andLanguage Therapists inIndependent PracticeTel: 01494 488 306Web: www.helpwithtalking.comBrainNav – The National BrainInjury Service DirectoryWeb: www.brainnav.info 20
Headway – the brain injury association British Association for Behaviouraland Cognitive Psychotherapies(BABCP)Tel: 0161 705 4304Email: babcp@babcp.comWeb: www.babcp.comBritish Association forCounselling and PsychotherapyTel: 01455 883 300Email: bacp@bacp.co.ukWeb: www.bacp.co.ukBritish Association of Brain InjuryCase Managers (BABICM)Tel: 0161 764 0602Email: secretary@babicm.orgWeb: www.babicm.orgBritish Association of OccupationalTherapists and College ofOccupational TherapistsTel: 020 7357 6480Email: reception@cot.co.ukWeb: www.cot.co.ukBritish Psychological Society (BPS)Tel: 0116 254 9568Email: enquiries@bps.org.ukWeb: www.bps.org.ukCare Quality Commission (CQC)Tel: 03000 616161Web: www.cqc.org.ukChartered Society of PhysiotherapyTel: 020 7306 6666Web: www.csp.org.ukCollege of Sexual andRelationship TherapistsTel: 020 8543 2707Email: info@cosrt.org.ukWeb: www.cosrt.org.ukCounselling DirectoryTel: 0333 3447 990Web: www.counsellingdirectory.org.ukUK Council for PsychotherapyTel: 020 7014 9955Email: info@ukcp.org.ukWeb: www.ukcp.org.ukPhysio FirstTel: 01604 684 960Email: minerva@physiofirst.org.ukWeb: www.physiofirst.org.uk21
Rehabilitation after brain injuryRelate – the relationship peopleTel: 0300 100 1234Web: www.relate.org.ukRoyal College of Speech andLanguage Therapists (RCSLT)Tel: 020 7378 1200Email: info@rcslt.orgWeb: www.rcslt.orgUK Council for PsychotherapyTel: 020 7014 9955Email: info@ukcp.org.ukWeb: www.psychotherapy.org.ukUnited Kingdom AcquiredBrain Injury Forum (UKABIF)Tel: 0845 608 0788Email: info@ukabif.org.ukWeb: www.ukabif.org.ukHow to donateHeadway – the brain injury association is a registeredcharity (1025852) and relies upon voluntary support tofund its work.If you would like to help Headway by making a donationyou can do so by donating online at www.headway.org.uk,contacting the Fundraising Team on 0115 924 0800, orsending a cheque to:Headway – the brain injury associationBradbury House190 Bagnall RoadOld BasfordNottingham NG6 8SF 22
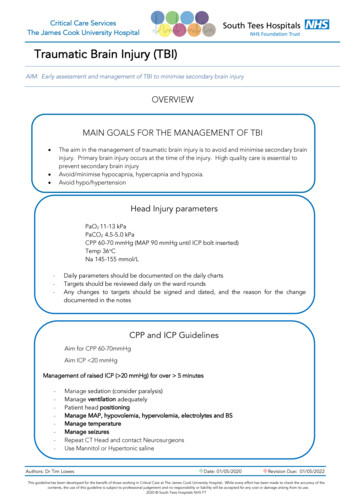
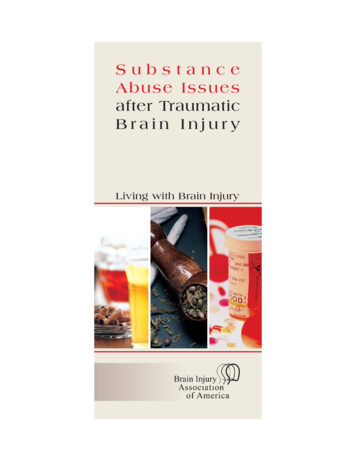
Headway – the brain injury association Internal areas of the brainand their functionCerebral cortex(see overleaf)Corpus callosumpasses informationbetween the left andright hemispheresVentriclescontaincerebrospinal fluidThalamuspasses sensoryinformationto the cerebralcortexPituitary glandregulates the body’shormone productionCerebellumcontrolsco-ordinationof movementHypothalamuscontrols the pituitary gland in order toregulate temperature, blood pressure,appetite, wakefulness and sexual arousalBrain stemincludes the midbrain, medulla and pons, controlling breathing,heart rate, consciousness, blood circulation, basic motor responses,relaying sensory information and regulating the sleep-wake cycle23
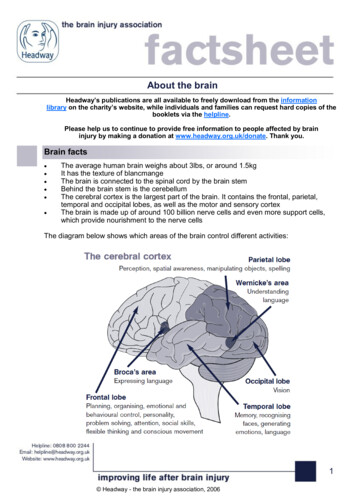
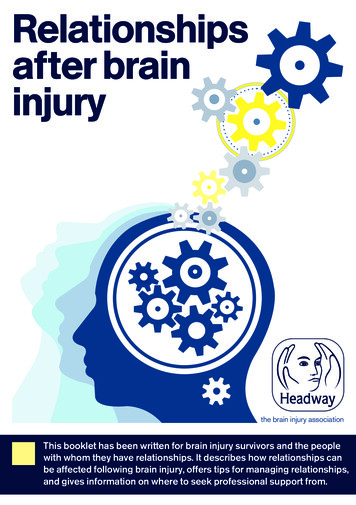
Rehabilitation after brain injuryThe cerebral cortexParietal lobePerception, spatial awareness, manipulating objects, spellingWernicke’s areaUnderstandinglanguageBroca’s areaExpressing languageFrontal lobePlanning, orga
discharge from hospital. Neurological rehabilitation centres provide an ideal setting for further treatment, with a structured rehabilitation programme in place throughout the day. Rehabilitation back into the community:Following an inpatient rehabilitation stay, some patients may be transferred to a residential transitional living unit.