Transcription
Providing Support to PatientsDiagnosed with HypertensionTiana Wyrick, RN, BSNProgram Manager, Heart Disease and Stroke PreventionBureau of Community Chronic Disease Prevention09/13/2017Kristine Mesler, RN, MPADirector, Bureau of Women, Infant and Adolescent Health
2Purpose Define hypertension and identify the burden if untreatedDefine undiagnosed hypertensionIdentify the modifiable/unmodifiable risk factors for hypertensionIdentify the lifestyle changes and resources that improvehypertension control Discuss the role home BP monitoring plays in improvinghypertension control Review the role Health Home Care Manager can play with assistingpatients Provide guidance on special consideration for women ofreproductive age (up to 55 years old)
3Blood Pressure Stages Blood pressure is the force thatmoves blood through our arteries.High Blood Pressure (BP) occurswhen the force of the blood isconsistently greater than 140/90 mmHg.Hypertension diagnosis occurs whentwo separate readings at twoseparate visits is greater than orequal to 140/90 mmHgUncontrolled hypertension is definedas BP readings greater than orequal to 140 and or 90 mm Hg
4Burden of HypertensionUnited StatesNew York State 4.8 Million adults (31.5%) 1 of every 3 adults Only 63% have their BPcontrolled75 million adults (30.9%)1 of every 3 adultsOnly half (54%) are controlledCost: 46 billion each yr.(health care services, meds,missed work days)Merai R, Siegel C, Rakotz M, Basch P, Wright J, Wong B; DHSc., Thorpe P. CDC Grand Rounds: A Public Health Approach to Detect and ControlHypertension. MMWR Morb Mortal Wkly Rep. 2016 Nov 18;65(45):1261-1264
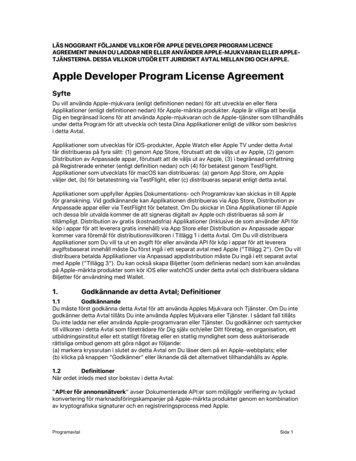
5Burden of HypertensionAge and GenderRace and Ethnicity
6Undiagnosed HTNWhat is it? There are about 11.5 millionpeople in the U.S. who don’t realize theyhave hypertension. This person has BPreadings above 140/90 mmHg but havenever been told they have hypertension.How is it identified: Any patient with twoor more readings above 140 and or 90mmHg during two separate office visitsduring the past year.Next steps: Identify these patients throughthe use of patient registries and follow-upfor reevaluation and possible diagnosis. HH Care Managers should ask aboutthe patient’s BP readings and canassist to determine if there is aconcern 80.9% have health insurance82.7% report having a usualsource of care63.3% have received caretwo or more times in the pastyear
7Burden if left untreated High BP oftenhas nosymptoms/silentcondition Major riskfactors for heartattacks andstrokePREGNANCYCOMPLICATIONS
8Risk FactorsNon-ModifiableModifiable GenderAgeRace (AA at greater risk)Family historyOverweight/ObesityHigh Sodium DietExcess use of alcoholLack of physical activitySmokingStressPregnancy planning/contraception
9Lifestyle Modifications that Lower BP*Lifestyle Modifications1 (LM)Modification RecommendationApproximate SBP**Reduction (Range)† †WeightreductionMaintain normal body weight (body mass index 18.5–24.9 kg/m2)5–20 mm Hg/10kgAdopt DASH†††eating planConsume a diet rich in fruits, vegetables, and lowfat dairy products with areduced content of saturated and total fat8–14 mm HgDietary sodiumreductionReduce dietary sodium intake to no more than 100 mmol per day (2.4 g sodiumor 6 g sodium chloride)2–8 mm HgPhysicalactivityEngage in regular aerobic physical activity such as brisk walking (at least 30 min 4–9 mm Hgper day, most days of the week which may be broken into shorter time intervalssuch as 10 minutes each of moderate or vigorous effort)Moderationof alcoholconsumptionLimit consumption to no more than 2 drinks (e.g. 24 oz. beer, 10 oz. wine, or 3oz. 80-proof whiskey) per day in most men, and to no more than 1 drink per dayin women and lighter weight persons2–4 mm HgSBP – systolic blood pressure††The effects of implementing these modifications are dose and time dependent, and could be greater for some individuals†††DASH – Dietary Approaches to Stop Hypertension**
10Lifestyle Modification Guidance and ResourcesHealthy Weight: USDA Choose My Plate (www.choosemyplate.gov)
11Lifestyle Modification Guidance and ResourcesDASH Diet: dash brief.pdf Diet that emphasizes fruits, vegetables, fat free or low fat milk andmilk products, whole grains, fish poultry, beans, seeds, and nuts.Also contains less sodium, sweets added sugars and beveragescontaining sugars, fats, and red meats.Sodium Reduction Most of the sodium we consume comes from prepared foods suchas deli meats; pizza; salad dressings; taco or packageseasonings; soups; packaged rice or pasta dishes; sauces andgraviesLower the amount of sodium by;––––––Reading nutrition fact labelsBuy low sodium or reduced sodium or no-salt-added productsLook for fresh, frozen or canned veg. without added sauces orseasoningsChoose fresh or frozen poultry and leans meatsCook more often at homeUse herbs and spices instead of salt to your recipes and dishes
12Lifestyle Modification Guidance and Resources– Moderate drinking : 1 drink per day for women and up to 2 drinksper day for men.– Heavy drinking is defined as 8 drinks or more for women and 15or more for men per week.– Standard Drink: 12 ounces of beer (5% alcohol content).8 ounces of malt liquor (7% alcohol content).5 ounces of wine (12% alcohol content).1.5 ounces or a “shot” of 80-proof (40% alcohol content) distilled spiritsor liquor (e.g., gin, rum, vodka, whiskey).– There is no known safe amount of alcohol use during pregnancyor while trying to get pregnant.
13Lifestyle Modification Guidance and ResourcesPhysical Activity: 2008 guidelines (https://health.gov/paguidelines/pdf/paguide.pdf) Adults need at least:Min /weekIntensityExample150 min (2hr /30min)ModerateBrisk Walk; Bike Flat; Mowing theLawnMuscle Strengthening 2 or moredays per weekWorking all major muscle groupsLegs, Hips, Back, Abdomen, Chest,Shoulders, and Arms75 min (1hr/15 min)VigorousRunning/ Jogging, Bike Hills For extensive health benefits: 300 minutes (5 hours) a week of moderate-intensityaerobic physical activity Healthy women should get at least 150 minutes (2 hours and 30 minutes) per weekof moderate-intensity aerobic activity, such as brisk walking, during and after theirpregnancy. It is best to spread this activity throughout the week Healthy women who already do vigorous-intensity aerobic activity, such as running,or large amounts of activity can continue doing so during and after their pregnancyprovided they stay healthy and discuss with their health care provider how andwhen activity should be adjusted over time
14Lifestyle Modification Guidance and Resources
15Role of a HH Care Manager - LifestyleModification Guidance and Resources Health Home Care Managers have an opportunity to assistpatientsKnowing and understanding the risk factors and the lifestyleof patients you serveConnecting patients to resources and solution focus servicesAbility to connect patient’s lifestyle with wellness and wellbeing outcomesFocus on risk avoidance can lead to avoidable hospitalizationand other life threatening issues i.e. strokes
16Clinical Protocol forControlling HTN
17Best Practices to Improve HTN Control Adopt a HTN treatment protocolPromote self-management and lifestylemodificationCreate HTN Registry with reportingfunctionalityAssess for medication adherence– Morisky Scale 4 part questionAdopt a team based approach to careTrain staff on accuracy in BP measurementRefer patients to HBPM with provider F/U– Train patients on how to take anaccurate BP
18Blood Pressure Self-Monitoring Self-measured BP monitoring sometimes called homeBP monitoring is a patient performed measurement oftheir own BP outside of the clinical setting. Its different from the ambulatory BP 24 hour monitoring Should always be used with additional support from ahealth care professional Is proven to improve BP control when a patient/clinicianfeedback loop is used
19Patient/Clinician Feedback Loop
20Accuracy in BP Measurement
21BP Loaner Program
22BP LoanerProgram
23Special Considerations for Women of Reproductive Age Approximately 45% of births nationally are unintended (mistimed,unplanned or unwanted at the time of conception)Unintended pregnancies minimize the ability to prepare for a healthypregnancy and have proactive conversations with health care providersIt is important to start a universal focus on the importance ofpreconception care to begin to reduce maternal mortality and morbidityAsk about pregnancy intention at each health care visitPreconception care is important for all, but crucial for those with chronicconditions, such as hypertension
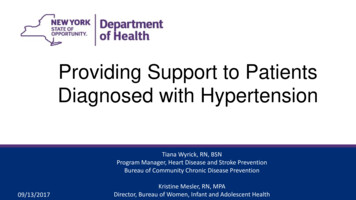
24Unintended PregnancyMistimed Woman did not want to becomepregnant at the time pregnancyoccurred but did want to becomepregnant at some point in thefuture 27% of all pregnanciesUnwanted Woman did not want to becomepregnant then or at any time in thefuture 18% of pregnanciesPotential Health Impacts of Chronic Disease
25Preconception/Prepregnancy Counseling– Desires pregnancy: Discuss with primary health care providerMay refer to maternal-fetal medicine specialistBlood pressure under stable controlOn medication that is safe for use with pregnancy– Does not desire pregnancy: Refer to primary health care provider or women’s health careprovider for contraceptive counseling Discuss availability of effective and highly effective contraception
26Contraceptive Methods
27Importance of Preconception Care Important opportunities to improve outcomes for motherand baby Requires active patient participation and individualizedmanagement plans Topics addressed include: diet, weight, exercise,smoking, use of alcohol and drugs, environmental risks,vaccination status Management of medical conditions
28HH Care Manager’s Role - Women of Reproductive Age HH Care Managers should discuss with women ofreproductive age their pregnancy considerations– Especially since the patients served by HHs have chronicconditions Ask about pregnancy intention Connect the patient or ensure involved providers arediscussing preconception care with the patient– How will the patient’s chronic condition be impacted by apregnancy? If the patient is or becomes pregnant, ensure connection toproviders that can work with the patient to address chroniccondition and the pregnancy- Ensure prenatal services are in place
29Characteristics Associated with MaternalDeaths: Provider-Identified Risk Factors2006-2008 (n 125)At least one risk factoridentified2012-2013 (n 60)*64%85%Hematologic19% (n 29)25% (n 15)Hypertension17% (n 26)17% (n 10)Cardiac13% (n 20)18% (n 11)Pulmonary9% (n 13)18% (n 11)Endocrine8% (n 12)17% (n 10)Psychiatric disorders5% (n 8)12% (n 7)*Preliminary 2012-2013 data
30Best Practices for PregnancyBefore Pregnancy Lifestyle Changes: limit salt intake, get regular physicalactivity, lose weight if overweight/obese Take prescribed medicationsWhile Pregnant Obtain prenatal health care on regular basis Avoid alcohol and tobacco Avoid OTC medications without medical care provider’sconsent
31Best Practice ResourcesProfessional Resources AMA/Johns Hopkins SMBP MonitoringProgramMillion HeartsAccuracy in BP Measurement-trainingmodule (Contact Tiana Wyrick forinformation)CHW online training module– HTN– Asthma– Diabetes– PreDiabetes– Self-ManagementCVD Health and Risk ReductionGuidelines & HTN Guidelines forChildren and AdolescentsPatients Community Based Resources YMCA- BPSM, Health Heart Ambassadors– Westchester, Yonkers, Syracuse– Albany and Yates County (coming soon)Chronic Disease Self-Management Programs:Contact Celest Harp at:managemyhealth@health.ny.gov– January 2018 WebinarHome BP Monitoring
32Resources for Contraception andHypertension During PregnancyContraceptive Counseling and Resources: aceptiveCounselingReplaceable.pdf m a 508tagged.pdf on/index.htmHypertension During Pregnancy: https://www.health.ny.gov/professionals/protocols and guidelines/hypertensive disorders/2013 hdp executive summary.pdf bp-pregnancy od-pressure-duringpregnancy.aspx#
33Additional Patient Educational Resources Million Hearts Tools: s.html AHA: sure-at-Home UCM 301874 Article.jsp#.WawkBOSWyUk YMCA: Blood Pressure Self-Monitoring Program: http://www.ymca.net/bloodpressure-self-monitoring/ Physical Activity https://www.cdc.gov/physicalactivity/index.html Birth Control: https://www.bedsider.org/ Planning for Pregnancy: https://www.cdc.gov/preconception/planning.html
34Thank You!Tiana ne Meslerkristine.mesler@health.ny.gov518-474-0535
Adopt DASH eating plan Consume a diet rich in fruits, vegetable s, and lowf at dair y produc ts with a reduced content of saturated and total fat 8 14 mm Hg Dietar y sodium redu c tion Reduce dietar y sodium intake to no more than 100 mmol per day (2.4 g sodium or 6 g sodium chloride) 2 8 mm Hg Physical activit y