Transcription
APC Revenue Cycle:Tips for SuccessAudio Seminar/WebinarJuly 23, 2009Practical Tools for Seminar Learning Copyright 2009 American Health Information Management Association. All rights reserved.
DisclaimerThe American Health Information Management Association makes norepresentation or guarantee with respect to the contents herein andspecifically disclaims any implied guarantee of suitability for any specificpurpose. AHIMA has no liability or responsibility to any person or entity withrespect to any loss or damage caused by the use of this audio seminar,including but not limited to any loss of revenue, interruption of service, lossof business, or indirect damages resulting from the use of this program.AHIMA makes no guarantee that the use of this program will preventdifferences of opinion or disputes with Medicare or other third party payersas to the amount that will be paid to providers of service.CPT five digit codes, nomenclature, and other data are copyright 2009American Medical Association. All Rights Reserved. No fee schedules, basicunits, relative values or related listings are included in CPT . The AMAassumes no liability for the data contained herein.As a provider of continuing education the American Health InformationManagement Association (AHIMA) must assure balance, independence,objectivity and scientific rigor in all of its endeavors. AHIMA is solelyresponsible for control of program objectives and content and the selectionof presenters. All speakers and planning committee members are expectedto disclose to the audience: (1) any significant financial interest or otherrelationships with the manufacturer(s) or provider(s) of any commercialproduct(s) or services(s) discussed in an educational presentation; (2) anysignificant financial interest or other relationship with any companiesproviding commercial support for the activity; and (3) if the presentation willinclude discussion of investigational or unlabeled uses of a product. Theintent of this requirement is not to prevent a speaker with commercialaffiliations from presenting, but rather to provide the participants withinformation from which they may make their own judgments.The faculty has reported no vested interests or disclosures regarding thispresentation.AHIMA 2009 Audio Seminar Series http://campus.ahima.org/audioAmerican Health Information Management Association 233 N. Michigan Ave., 21st Floor, Chicago, Illinoisi
FacultyArlene Baril, MS, RHIAArlene Baril is president of Baril & Associates Healthcare Consulting in Dallas, TX.Ms. Baril has over 29 years of experience specializing in revenue cyclemanagement and HIM operations. Prior to starting Baril &Associates, she wasexecutive vice president of HIM services at PHNS, Dallas. Arlene has also servedas vice president of HIM and software services for UASI in Cincinnati, OH, directorof HIM and coding services for Pyramid/The HealthCare Financial Group, andregional manager for PricewaterhouseCoopers, LLP. Ms. Baril is a frequentcontributor to many HIM and healthcare financial publications and served as aneditorial advisory board member of Briefings on Coding Compliance and Briefingson APCs. She has presented numerous educational seminars and state andnational conferences around the country.AHIMA 2009 Audio Seminar Seriesii
Table of ContentsDisclaimer . iFaculty . iiPresentation Objectives . 1Count the Silos: . 1Hospital Revenue Cycle Count the Silos? . 2Some Statistics to Ponder: . 2-3Components of the Revenue CycleWhat is the Revenue Cycle? . 4Visual . 5Alphabet Soup . 5What Language Are YOU Speaking? . 6Players in the Revenue Cycle – Departments . 6Functions of the Revenue CycleAdmitting/Access Management . 7Case Management/UR . 7Charge Capture . 8Health Information Management . 8Unbilled Management . 9Patient Financial Services/Business Office . 9Finance .10Compliance .10Program Development: The Revenue Cycle Team . 11-12Sample Revenue Cycle Team Objectives .12Revenue Cycle Team Notes .13Program Development – Unbilled Management – The HIM Role .13Information Systems – Data Collection and Accessibility .14Measurements/Indicators .14Patient Registration – Opportunities .15Information Systems – Opportunities .16Charge Capture Process – Opportunities.16Denials Management – Opportunities .17OCE Editor and CCI EditsThe Outpatient Code Editor (I/OCE) .18Purpose of the OPPS I/OCE:.19The I/OCE Dispositions: .19Sample OCE Edits.20APC OpportunitiesCommon Missed Reimbursement Under OPPS.21Coding – Opportunities . 21-22HIM vs. CDM/Ancillary Charging .23Interventional Procedures . 23-24(CONTINUED)AHIMA 2009 Audio Seminar Series
Table of ContentsTransfusion Services.24Billing Example: Blood Transfusion .25Billing Blood & Blood Products .25Billing Example: Blood Charges.26Case Study – Actual APC AuditThe AuditSelecting a Sample .27What You’ll Need .28What to Look For .28Remittance Advice Statements (RA’s) . 29-30Return to Provider (RTP) .31Audit Summary – Sample Audit .32Breakdown by Case Type/Errors .32Errors by Error Type .33Annualized Financial Opportunity (Forecast) .33Audit Findings – Sample Audit .34After the Audit .34Revenue Cycle Process: Areas to MonitorCharge Description Master (CDM) .35Patient Accounts .36System Issues.36Things to Consider .37Revenue Capture: Critical Success FactorsPhysicians .37Patient Registration .38Clinical Department Operations .38Information Systems.39Business Office.39Claims Review .40Conclusion:.40Resource/Reference List .41Audio Seminar Discussion .41Become an AHIMA Member Today! .42AHIMA Audio Seminar Information Online .42Upcoming Audio Seminars .43Thank You/Evaluation Form and CE Certificate (Web Address) .43Appendix.44Resource/Reference List .45CE Certificate InstructionsAHIMA 2009 Audio Seminar Series
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsPresentation Objectives Identify the components of the RevenueCycleEvaluate the role of each departmentDemonstrate the impact of coding andhealth information management (HIM)Denials in the APC system – Prepare aplan for auditing denialsOPPS Audit OpportunitiesSample Case StudyRevenue Cycle Areas to Monitor1Count the Silos: Organizational silos make it difficult toanticipate surprises Various people have various pieces of thepuzzle, but no one has them allSilos disperse information &responsibilityAssume that someone has responsibility,but actually no one really does2AHIMA 2009 Audio Seminar Series1
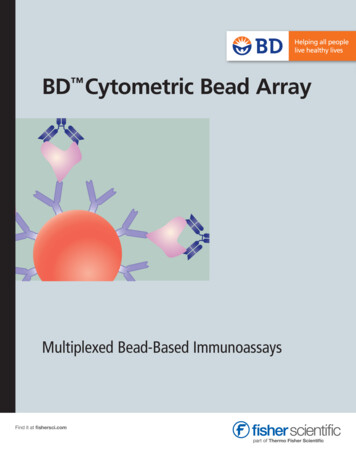
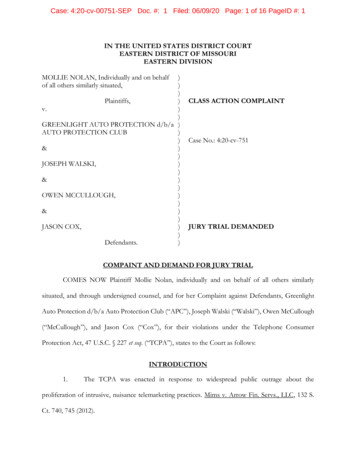
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsHospital Revenue Cycle:Count the Silos?SchedulingRegistrationInsurance VerificationAuthorizations/ReferralsFinancial CounselingEncounterCharge Capture & EntryMedical ManagementMedical Records & CodingCharge Description ion ProcessingClaim Follow-upPayment ProcessingDenial ManagementRejected Claims Remittance AdviceProvider PayerExternalError-free claims depends on the successful execution of numerous front-end revenue cycle functionsData collected and procedures required vary depending on patient’s type of insuranceCurrent process is highly manual and contains multiple opportunities for human errorSource: HFMA3Some Statistics to Ponder: Health care industry experts estimate that 25-30%of all health care claims are denied or rejectedProviders typically lose 3-4% of their net revenueeach year from denialsThe Health Care Advisory Board released a surveyof hospital CEO’s that listed decreased claimreimbursement for services as their highestpriority financial concern (79% of those surveyed)Typically about 50% of denied claim amounts arenot recoveredUsing technology can add about 20% to thebottom line of previously un-recovered amountsSource: Health Care Advisory BoardAHIMA 2009 Audio Seminar Series42
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsSome Statistics to Ponder: Various reviews and surveys haveshown that hospitals don’t collectbetween 4-12% of the monies due tothem, because of: Coding errorsCDM errors due to poor maintenance ofthe CDMInsufficient documentation to supportmedical necessity5Some Statistics to Ponder: Outdated billing and collections systemsand processes can delay payments for upto 75 days Non-healthcare organizations average 28daysExamples of reasons that delay payment:Authorization process failures Poor coding methodologies based on aspecific health plan's requirements Poor charge capture methodologies Billing follow-up failures AHIMA 2009 Audio Seminar Series63
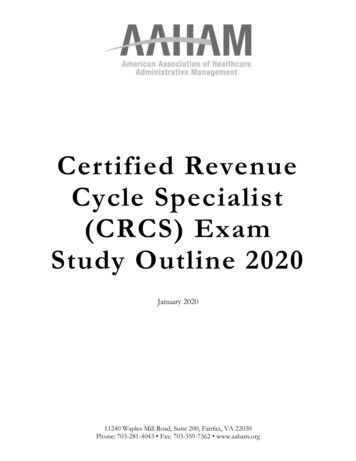
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsComponents of the Revenue Cycle7What is the Revenue Cycle?The processes by which a healthcare facilityreceives payment for services rendered –service point of entry to paymentreceipt/resolution.8AHIMA 2009 Audio Seminar Series4
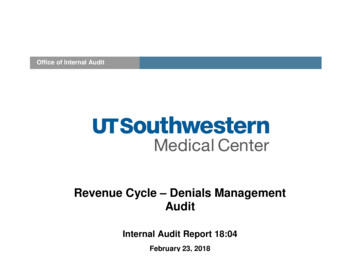
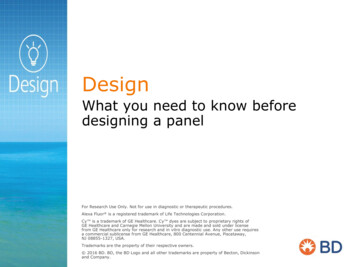
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsWhat is the Revenue Cycle?VisualConsents, sedChargesChargesPostedPostedComplianceService Analysis, Charge Development, ProfitabilityEncounterEncounterCoded sted9What is the Revenue Cycle?Alphabet SoupCaseCasemixMixIndex(CMI)Index sicianQueryRTPRACsCash sDenialsAR DaysMS-DRGsMS-DRGsAHIMA 2009 Audio Seminar SeriesCPT CodesBill ngAuditsRevenueCodes105
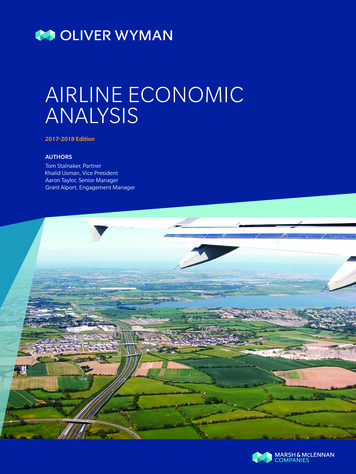
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsWhat Language Are YOU Speaking?ROIRelease of Information(HIM) Return on Investment(Finance) ADRAdditionalDocumentation Request(HIM/Business Office) Average Daily Revenue(Finance) 11Players in the Revenue CycleDepartmentsAdmitting/Access Management Case Management/UR Charge Capture Health Information Management Unbilled ManagementBusiness Office/Patient Financial Services Finance Compliance Information TechnologyAHIMA 2009 Audio Seminar Series126
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsFunctions of the Revenue CycleAdmitting/Access Management lection of insurance informationCollection of co-paysConsents/NoticesIssuance of Advanced BeneficiaryNotices13Functions of the Revenue CycleCase Management/UR Documentation Review-MedicalNecessity MD/Provider Interaction/Education RAC Reviews-Assistance Critical Pathway/Guideline Concurrent MS-DRG AssignmentCDI programGOAL: MINIMIZE retrospective processes 14AHIMA 2009 Audio Seminar Series7
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsFunctions of the Revenue CycleCharge Capture Point of Care vs. Batch Linking to Order Entry Late Charges (non-existent underOPPS) Data Dictionary (Charge Master) Coding Updates (quarterly changes forOPPS)15Functions of the Revenue CycleHealth Information Management Reconciliation of accounts vs.documentation received-Medical Necessity Processing Cycle Order and Timeliness Coding (only 21% in the OP environment) Physician Query Process Coding Accuracy Audits – Internal andExternal Requests for Records/Documentation(ROI)-now includes RAC requests CDI ProgramAHIMA 2009 Audio Seminar Series168
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsFunctions of the Revenue CycleUnbilled Management RTP/Denial ResolutionResponse to Business Office/PFS RequestsEdit Correction (OCE and Groupers)Policy Development Based on CorporateGuidanceData PresentationData AnalysisWrite Off PreparationAdditional Documentation Requests (ADR’s)17Functions of the Revenue CyclePatient Financial Services/Business Office Edits (Front End, Pre/Post Billing)Generation and ResolutionBill GenerationDenials/RTP’s (Return toProvider)Posting (Remits, Payments)Additional Information RequestCoordinationBill Hold SettingsCharge Master MaintenanceAppealsAHIMA 2009 Audio Seminar Series189
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsFunctions of the Revenue CycleFinance Case mix AnalysisPatient Volume Data (MS-DRG Review)Service Line AnalysisDecision SupportData BenchmarkingAR DaysPrimary Data SourceAdministrative Representation of theRevenue Cycle Team19Functions of the Revenue CycleCompliance Legal Watchdog Regulatory Experts Somewhat dependent on background Coding Accuracy Review Coordinator Typically the RAC point person HIPAA Enforcer External Audits20AHIMA 2009 Audio Seminar Series10
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsProgram Development:The Revenue Cycle Team1.2.3.4.5.6.7.Determine the need to have a RevenueCycle Team. YES, you need one!!!Determine who are the members of theTeamAssess what the Team knows (Baseline)Determine if education of Team members isnecessary at this pointDefine Team GoalsIdentify and Define Data Needs and SourcesStandardize Language and Data Reporting21Program Development:The Revenue Cycle TeamDevelop Key Indicators/Measurementalong the entire Revenue cycle9. Define Team and FacilityResponsibilities10. Determine What Functions are and areNOT being done (Gap Analysis)11. Identify Appropriate Types of Issuesfor the Team to address12. Prioritize Issues and Problem Areas8.22AHIMA 2009 Audio Seminar Series11
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsProgram Development:The Revenue Cycle TeamEducate your Team14. Educate your facility13.Revenue Cycle Manual Clinical Staff Targeted Problem Areas Annual Updates RegulatoryCodingCoordination of Upgrades/Updates16. Your work is never done15.23Sample Revenue CycleTeam Objectives Identify issues resulting in increased A/RPrioritize issues to addressCommunicate issues to appropriate areasSolve problems collaborativelyDevelop educational materials and provideeducation (can be done with internal orexternal staff)Develop a “map” or “blueprint” on how toimplement new servicesReview denials and actively discuss appealprocess and successDiscuss intermediate measurements/indicatorsAHIMA 2009 Audio Seminar Series2412
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsRevenue Cycle Team Notes Catalog what process are and are NOT beingdone and whereProcess recommendations/fixes based onproblems resolution solutionsDetailed multidisciplinary process analysisDetermines measures/indicators for facilityProvide EducationOffer Revenue Cycle GuidanceDetermine Write Off thresholdsDetermine High Dollar thresholdReview Appeal Responses (KEY for RAC)25Program DevelopmentUnbilled Management – The HIM Role Liaison between all areasCoded Data ExpertsCoding Accuracy and ConsistencyCase mix AnalysisMS-DRG/APC ExpertsEducationHolder of the “Rework” EffortCoding a common focusRAC and CDIAHIMA 2009 Audio Seminar Series2613
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsInformation SystemsData Collection and AccessibilityDepartments within the Revenue Cyclecommonly “own” component systems. ADT SystemCollects and stores registration information Assigns MR and Account #s Billing SystemGenerate Bills Generates Monitoring and Edit Reports Encoder/GrouperAbstracting Application Account holds for Documentation issues27Measurements/Indicators DNFB (Discharged NotFinal Billed)AR Days% and of WriteOffs% of Clean Claims% of Claim RTP’s(Return toProvider)AHIMA 2009 Audio Seminar Series % of Denials % of AccountsMissingDocuments # of Query Forms % of Late Charges % of AccurateRegistrations2814
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsPatient Registration –Opportunities Develop standardized policies andprocedures to:Ensure authorization documents are obtainedprior to service Ensure all other documentation necessary forbilling is timely and accurate Implement a POS program to collect copayments for all clinic visitsImplement fully functional compliancechecker/medical necessity software tosupport ABN compliance29Patient Registration –Opportunities Establish a central authority for allclinic registration to provideconsistent management of: Standardized documentation, processand data integrity for clinic registrationTraining of new registrarsImplement a comprehensive (financialimpact-oriented) data quality auditprogram30AHIMA 2009 Audio Seminar Series15
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsInformation Systems –OpportunitiesVerify that the Medicare outpatient systemsclaim goes through all appropriate edits beforefinal submission to the fiscal intermediary/MAC Determine the differences between billing editsin the internal system versus those utilized inthe Medicare outpatient code editor Ensure that billing edits are workingappropriately Program appropriate management reports sothat the hospital can evaluate performanceunder OPPS 31Charge Capture Process –Opportunities Develop a concurrent charge capture auditprogram to include: Improved charge capture/increased revenueA “built-in” clinician-to-clinician educationalprocess to support each of the chargingdepartments with specific feedback and selectivetraining, as neededProactive audits for each charging area,identifying and correcting charge captureproblems as they occurLate charge problems identified and correctedprior to the initial bill being sent and correctivefeedback to charging departmentsCharging protocols maintained and updated, asnecessary32AHIMA 2009 Audio Seminar Series16
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsDenials Management –Opportunities Implement a comprehensive denial managementprogram that incorporates all functional areas ofthe revenue cycle and has formalized policies,procedures, and weekly results reporting byaccountable area. Denial Management “Team” would includerepresentatives from key revenue cycle areas,including: Patient AccessHealth Information ManagementFinanceCharge CapturePatient AccountingUtilization ReviewManaged CareFinancial Counseling33Denials Management –Opportunities Form a denials recovery unit Appoint an authorizations clerk Maintain a denials database Consider automation of the process Do a comprehensive contracts review34AHIMA 2009 Audio Seminar Series17
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsOCE Editor and CCI Edits35The Outpatient Code Editor (I/OCE)Processes claims for all outpatient institutional providersincluding OPPS and non-OPPS hospitals Claim will be identified as 'OPPS' or 'Non-OPPS' by passing aflag to the OCE in the claim record, 1 OPPS, 2 Non-OPPS; ablank, zero, or any other value is defaulted to 1 This version of the OCE processes claims consisting ofmultiple days of service. The OCE will perform three majorfunctions: Edit the data to identify errors and return a series of editflags Assign an Ambulatory Payment Classification (APC) numberfor each service covered under OPPS, and return informationto be used as input to a PRICER program Assign an Ambulatory Surgical Center (ASC) payment groupfor services on claims from certain Non-OPPS hospitals The OCE will accept up to 450 line items per claim. The OCEsoftware is responsible for ordering line items by date ofservice36 AHIMA 2009 Audio Seminar Series18
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsPurpose of the OPPS I/OCE:The (I/OCE) software combines editing logic with the new APCassignment program designed to meet the mandated OPPSimplementation. The software performs the following functionswhen processing a claim: Edits a claim for accuracy of submitted data Assigns APCs Assigns CMS-designated status indicators Assigns payment indicators Computes discounts, if applicable Determines a claim disposition based on generated edits Determines if packaging is applicable Determines payment adjustment, if applicable Purpose of the non-OPPS I/OCE functionalityIn addition, the I/OCE program screens each procedure codesagainst a list of approximately 2500 ASC procedures, andsummarizes whether or not the bill is subject to the ASClimitation.37The I/OCE Dispositions:There are currently 83 different edits in the OCE. The occurrence of an edit can result in oneof six different dispositions. Claim Rejection -one or more edits present that cause the whole claim to be rejected.A claim rejection means that the provider can correct and resubmit the claim but cannotappeal the claim rejection. Claim Denial -one or more edits present that cause the whole claim to be denied. Aclaim denial means that the provider can not resubmit the claim but can appeal the claimdenial. Claim Return to Provider (RTP)-one or more edits present that cause the wholeclaim to be returned to the provider. A claim returned to the provider means that theprovider can resubmit the claim once the problems are corrected. Claim Suspension-one or more edits present that cause the whole claim to besuspended. A claim suspension means that the claim is not returned to the provider, butis not processed for payment until the FI/MAC makes a determination or obtains furtherinformation. Line Item Rejection-one or more edits present that cause one or more individual lineitems to be rejected. A line item rejection means that the claim can be processed forpayment with some line items rejected for payment. The line item can be corrected andresubmitted but cannot be appealed. Line Item Denials-one or more edits present that cause one or more individual lineitems to be denied. A line item denial means that the claim can be processed forpayment with some line items denied for payment. The line item cannot be resubmittedbut can be appealed.38AHIMA 2009 Audio Seminar Series19
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsSample OCE Edits 1235681852 60 Invalid diagnosis codeDiagnosis and age conflictDiagnosis and sex conflictE-code as reason for visitInvalid procedure codeProcedure and sex conflictInpatient only procedureObservation does not meet criteriafor separate paymentUse of modifier CA with more thanone procedure not allowed39APC Opportunities40AHIMA 2009 Audio Seminar Series20
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsCommon MissedReimbursement Under OPPS1.HIM vs. CDM/Ancillary Charging2.ER & Clinic Visits3.Infusions and Injections4.Modifier Usage5.Observation Services6.Drugs/Pharmaceuticals7.Wound Care Services8.OCE/CCI edits/UB04 errors9.Cardiology & Interventional Radiology Services10.Transfusion services41Coding – Opportunities Reduce bill hold to industry standard oftwo-four days, and associatedturnaround time for codingTrack all uncoded accounts and report byreason and dollars to responsible areasContract with third party to provide atleast annual audits of facility codingProvide hardware and softwarecapabilities for coders to reduce the needto “toggle back and forth” betweensystems42AHIMA 2009 Audio Seminar Series21
APC Revenue Cycle: Tips for SuccessNotes/Comments/QuestionsCoding – Opportunities Run all bill edits at one time, producing areport that identifies all reasons a bill fails anedit before it is sent back for correctionConsider installing pre-bill edits on theabstracting system to allow coders to correctcoding errors before the abstract is finalized;allow coders to view charges and associatedChargemaster codes at the time ofabstractingPlace responsibility on ancillary departmentsto correct codes by installing a “front end”product to screen for medical necessity andother coding errors43Coding – Opportun
APC Revenue Cycle: Tips for Success AHIMA 2009 Audio Seminar Series 8 Notes/Comments/Questions Functions of the Revenue Cycle Charge Capture Point of Care vs. Batch Linking to Order Entry Late Charges (non-existent under OPPS) Data Dictionary (Charge Master) Coding Updates (quarterly changes for OPPS) 15 Functions of the Revenue Cycle