Transcription
St. Lawrence Chiropractic Clinic520 St. Lawrence St, PO Box 1118Winchester ON K0C 2K0(613) 774-BACK (2225)Patient #Welcome to our clinic! Please fill out our Confidential Patient Health Record completely andaccurately. Your answers will help determine how chiropractic care can help you.If you have any questions, please don’t hesitate to ask our front desk staff or your chiropractor.PERSONAL INFORMATIONNameAddress Box # City Prov P/CHome Phone E-Mail AddressWork Phone Cell PhoneBirth Date (dd/mm/yyyy) / /AgeHeightWeight Male Female OtherOccupation & EmployerMarital Status S M C/L D WSpouse/PartnerChildrenEmergency Contact & Relationship Phone numberAre you a student? Yes NoIf yes, where?How did you hear about our clinic? Personal referral: Phone Book Internet Sign Health professional: Other:Have you had any previous chiropractic care? Yes No If yes, with whom?Date of last treatmentWere you happy with the results? Yes NoCurrent Family Physician: Phone numberMay we contact your family physician for co-management? Yes NoDo you have Extended Health Benefits? Yes No Provider:Name of insurance holder:Policy #Birthday of insurance holder (yyyy/mm/dd) / / Member ID #REASON(S) FOR YOUR APPOINTMENTIs the purpose of this appointment related to: Job Auto accident Fall Sports Chronic Discomfort Wellness care OtherIf job related, are you claiming under WSIB? Yes NoClaim #If auto accident, are you claiming under insurance? Yes NoClaim #Page 1 of 4
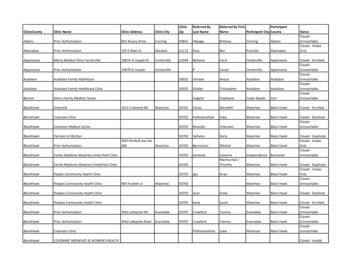
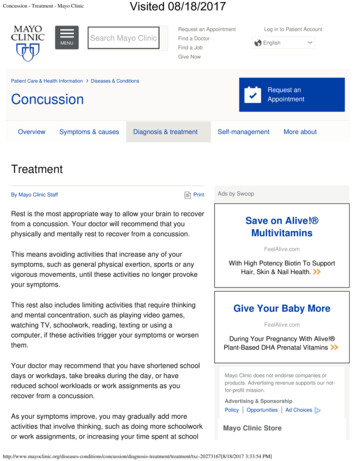
St. Lawrence Chiropractic Clinic520 St. Lawrence St, PO Box 1118Winchester ON K0C 2K0(613) 774-BACK (2225)Patient #Briefly describe your main health concern(s):How long have you had this condition?Is your condition getting: worse / better / same? (circle one)What makes the condition worse?What makes the condition better?What have you tried that has not worked?Have you seen any other physician or healthcare professional for this complaint? Yes NoIf yes, with whom: Date of last treatment:Were x-rays or any other medical testing performed?List any treatments performed:Mark the areas of your body where you feel the described sensations.Use the appropriate symbol, include ALL affected areas.Ache: \\\\Numbness: Pins and Needles: oooBurning: BBBStabbing: SSSThrobbing: TTTUsing the scale provided below, rate yourcurrent level of pain:(No pain) 0 1 2 3 4 5 6 7 8 9 10(Debilitating)Page 2 of 4
St. Lawrence Chiropractic Clinic520 St. Lawrence St, PO Box 1118Winchester ON K0C 2K0(613) 774-BACK (2225)Patient #HEALTH HISTORYPlease mark C beside the condition(s) you currently have (or experience on a recurring basis).Please mark P beside the condition(s) you have had in the past.Musculoskeletal SystemNervous SystemSystemicEar, Eyes, Nose, Throatneck problemsheadachesDiabeteseye problemsjaw problemsloss of feelingHypoglycemiavision problemsupper back problemsnumbnessEpilepsyear dischargeshoulder problemsdizzinessRheumatoidear painelbow / wrist problemsfaintingTBear ringinglow back problemsloss of balanceHIV / AIDShearing lossankle / foot problemsconfusionCancer:sore orgetfulnessParkinson’senlarged glandsmuscle sorenessfatigueThyroid problemsscoliosisanxietyother:Femalevaginal dischargeCirculatory systemGastrointestinal systemGenito-Urinary sytemvaginal bleedinghigh blood pressurepoor appetitepainful urinationpregnancyhigh cholesterolexcessive hungerexcessive urinationmenstrual painheart conditionabdominal painscanty urineirregular cycleaneurysmexcessive thirstdiscoloured urineMenopausal? Yes Nostrokenausea / vomitingvaricose yblack / bloody stoolhay feverMenAsthmaliver/gallbladder troublesinus painprostate problemschest painweight troubledrug allergydifficulty breathingulcerfood allergyOther:other:persistent coughPregnant? Yes NoDue date:Had any broken bones? Yes No ExplainBeen struck unconscious? Yes No ExplainAny significant accidents or injuries? Yes No ExplainHad surgery? Yes No ExplainHad any major strains or sprains? Yes No ExplainUse orthotics, heel lifts, or insoles? Yes No ExplainPage 3 of 4
St. Lawrence Chiropractic Clinic520 St. Lawrence St, PO Box 1118Winchester ON K0C 2K0(613) 774-BACK (2225)Patient #FAMILY HEALTH HISTORYPlease check any boxes that apply to anyone in your Family (not including you) High blood pressure Rheumatoid Arthritis Breathing or lung problems Heart disease Osteoarthritis Cancer: Stroke High cholesterol Neurological problems Diabetes (Type I or Type II) Thyroid / Hormone problems Other:HEALTH & LIFESTYLEYour condition(s) may be affected by your environment, the foods you eat, and your lifestyleactivities and habits. Please answer the following:Please list any medications you are currently taking and for how long:Please list any nutritional supplements you are currently taking and for how long:Exercise level? Low Medium High Activities:How would you describe your eating habits?How many glasses of water do you drink per day?Do you Smoke? Yes NoIf yes, how long and how much?Do you drink alcohol? Yes NoIf yes, how much?Do you sleep well at night? Yes NoIf no, why? Yes NoIf yes, why?Is your job stressful?Have you had any recent changes in body weight? Yes No If yes, how much?List any major life stresses over the last year:List any enjoyable hobbies you participate in:HEALTH GOALSAre you satisfied with your current overall health? Yes NoWhat things would you like to change/improve about your current level of health? Please explain:What is preventing you from achieving your goals?Is there anything else that you are concerned about or would like advice about?The information on this form is true to the best of my memory and I consent to further evaluation asdeemed appropriate by the Chiropractor:Signature of patient or legal guardianDatePage 4 of 4
File #Chiropractic & AcupunctureAdultChildChiropractic Initial Assessment 110 80Chiropractic Adjustment 45 30Reassessment* 85 60Modality (single application) 30 25Modality (multiple applications) 45 30Acupuncture 50 40Acupuncture and Chiropractic Adjustment 70 50Adult: Age 18 and older; Students with valid student card and seniors 65 and older receive a 10%discount on chiropractic servicesChild: Age 17 and younger* Reassessment is required after a patient has not seen their chiropractor for more than 2 years as thepractitioner will require more time to reassess your health status and diagnose your condition.Custom Foot Orthoses (Orthotics)Chiropractic Initial Assessment: Orthotics OnlyOrthotics – standard top coverOrthotics – specialty top coverOrthotics – with sandal or shoeCost of orthotics includes fitting (pick-up) and follow-up assessment. 70 425 475 500All prices are subject to change.Chiropractic Missed Appointment/Late Cancellation PolicyThere is a fee for missed Chiropractic appointments. We require 24 hours notice to cancel orreschedule an appointment. Failure to provide the required notice will result in a rescheduling fee.This will enable us to offer your cancelled time to other patients. Please visit our website for thecomplete clinic policy at stlawrencewchiro.ca.I have had the opportunity to review the St. Lawrence Chiropractic policies, including the missedappointment policy.Name:Signature:Date:
**Please be advised that we have a SCENT-FREE policy.****Please be sure to silence your CELL PHONE before you arrive at the clinic.**Welcome to St. Lawrence Chiropractic Clinic.Please fill out the Health History forms in advance of your appointment. It is important thatyou fill them out with as much accuracy as possible.Appointment questions: Should be directed to the front desk. They will gladly book orreschedule your appointments.Please be organized: We encourage patients to arrive 10 minutes before every appointment.If you are late, understand that you may not get the full allotted time for your appointment.We understand that sometimes situations arise beyond your control i.e. snow storms, freezingrain, etc. and in those circumstances every effort will be made to accommodate you.Cancellations & Missed Appointments: We require 24 hours notice to cancel or reschedule anappointment. There is a fee for missed Chiropractic and Massage appointments, as well asthose cancelled with less than 24 hours notice. This will enable us to offer your cancelled timeto other patients.Reminder emails for appointments are sent out 48 hours before your scheduled appointment(with the exception of weekends and holidays, at which time reminder emails may be sentearlier in order to allow for our 24 hour cancellation policy). Please ensure the front desk hasyour email address to receive reminder emails. Reminder emails are a courtesy and it isultimately your responsibility to remember your scheduled appointments.Scent Free Policy: In order to provide a healthy place of work and care, we have a strictfragrance-free policy. Please ensure that you are not wearing perfume or any strong scents(deodorant, perfume, body wash). Some patients are extremely allergic to scents, and can haveimmediate reactions, therefore this policy must be respected or your appointment can beforfeited.Email: While email is a convenient way to communicate with the office, please be aware thatresponding to emails does take time and expertise. Any emails can be directed through thefront desk to stlawrencechiro@gmail.com.All practitioners are bound by patient confidentiality and privacy laws and are unable to provideany information over email or other electronic means that require access to your patient chart.Contact us if you have a reasonably quick/simple question about your treatment plan or atherapy reaction. Anything the practitioner deems in depth will require another appointment.Any discussion of new treatment options or symptoms requires you to schedule a follow upconsultation.
Custom Foot Orthoses (Orthotics) Chiropractic Initial Assessment: Orthotics Only 70 Orthotics - standard top cover 425 Orthotics - specialty top cover 475 Orthotics - with sandal or shoe 500 Cost of orthotics includes fitting (pick-up) and follow-up assessment. All prices are subject to change.